Hypoganglionosis is a very rare disease that presents with severe chronic constipation resembling clinical features of Hirschsprung disease and may give rise to megacolon. The median age at diagnosis is considerably higher in this group of patients due to difficulties in diagnosis that is based in general on the findings of full‑thickness biopsy that may indicate, but often cannot prove, hypoganglionosis. Moreover, no consensus on the diagnostic criteria poses an additional challenge in the diagnostic workup.1 A delayed diagnosis leads to chronic constipation poorly treated with enemas and laxatives, lowers the quality of life, and may have fatal complications. A systematic review in 2010 of 92 cases presented in 11 publications revealed that only 32% of cases were diagnosed in newborns.2
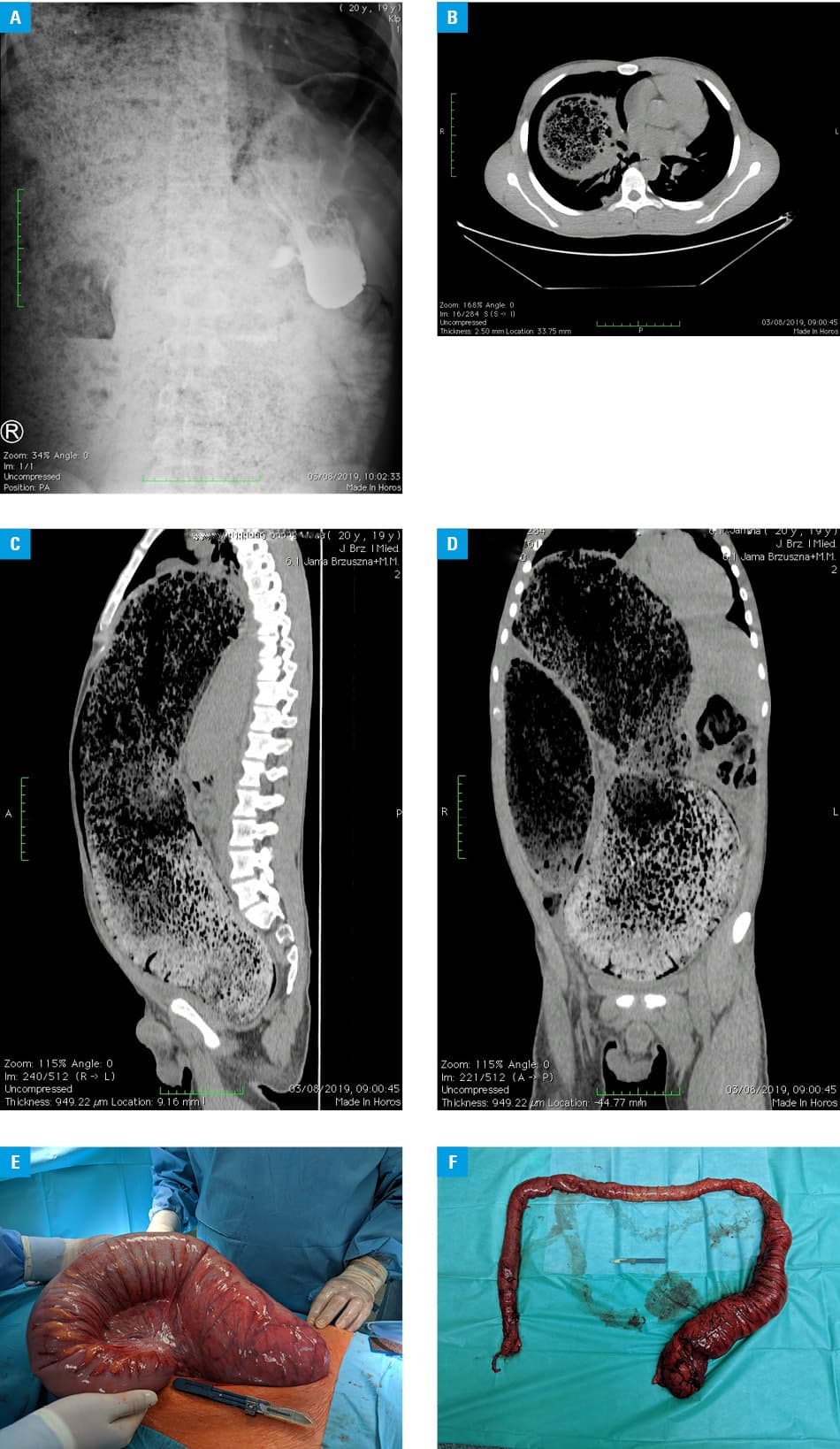
We present a 19‑year‑old man with chronic severe constipation who had been tested for Hirschsprung disease since early childhood but never received the diagnosis due to negative biopsy results. He underwent 3 rectal biopsies, which were negative for aganglionosis. He was diagnosed with chronic idiopathic constipation. The patient self‑medicated to attenuate symptoms with chronic use of laxatives, enemas, cigarette smoking, and food restriction, which led to poor health‑related quality of life. The patient was admitted with symptoms of acute obstruction, distention, painful abdomen, and vomiting. Laboratory findings were unremarkable. Abdominal X‑ray (Figure 1A) showed fecal impaction, and computed tomography scans (Figure 1B-1D) showed megacolon with compression on both abdominal and chest organs. The clinical and radiological presentation was typical of Hirschsprung disease in adults.3 Apart from acute symptoms, the patient was also malnourished (body mass index, 18.1 kg/m2; weight, 62 kg after manual disimpaction) and in poor mental health. Before the planned surgical treatment, the patient received total parenteral nutrition and underwent 2 sessions of manual disimpaction under general anesthesia as a mechanical preparation of the bowel. He displayed a high degree of emotional lability and did not consent to restorative proctocolectomy with ileal pouch‑anal anastomosis. Instead, he insisted on total proctocolectomy with a definitive ileostomy formation. Due to 19 years of suffering from chronic constipation, the patient’s quality of life was low, and he was not willing to bear the risk of ileal pouchitis or higher frequency of bowel movements. The surgery started with a laparoscopic approach, but due to lack of working space, it was converted to laparotomy. Intraoperatively, an enormously distended, thick‑walled megacolon with a maximum diameter of 20 cm was visualized; total proctocolectomy with definitive ileostomy formation was performed as planned. After the initial surgery, the patient presented with prolonged postoperative ileus and was, therefore, qualified for the second laparotomy during which stoma revision was performed. To our surprise, histopathology once again revealed sparse myenteric ganglia with nerve plexuses proliferation with a reduction of nerve cells toward the distal resection line without aganglionosis in the specimen leading to the final diagnosis of isolated hypoganglionosis.
The purpose of this case report is to highlight the radiological and clinical similarity of isolated hypoganglionosis to Hirschsprung disease, making the diagnosis difficult in the early period with rectal biopsies that can be false negative, thus leading to delayed diagnosis and treatment with subsequent poor quality of life.
- Friedmacher F, Puri P. Isolated Hypoganglionosis. In: Puri P, ed. Hirschsprung’s disease and allied disorders. Springer; 2019: 311‑312.
- Dingemann J, Puri P. Isolated hypoganglionosis: systematic review of a rare intestinal innervation defect. Pediatr Surg Int. 2010; 26: 1111‑1115. | Crossref
- Vorobyov GI, Achkasov SI, Biryukov OM. Clinical features’ diagnostics and treatment of Hirschsprung’s disease in adults. Color Dis. 2010; 12: 1242‑1248. | Crossref
ARTICLE INFORMATION