A double-edged sword of immunotherapy: new category of colitis mimicking inflammatory bowel disease



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
A double-edged sword of immunotherapy: new category of colitis mimicking inflammatory bowel disease
The dynamic progress in immunotherapy is constantly expanding therapeutic possibilities for various diseases by introducing several new monoclonal antibodies that specifically target molecular pathways involved in inflammation and oncogenesis. However, alongside a considerable improvement in therapeutic outcomes, the novel therapies also gave rise to some unexpected dangers.
We present 4 patients with colitis induced by biological agents characterized by different mechanisms of action and used for multiple indications. However, in each case, the clinical scenario and endoscopic images of colitis were similar.
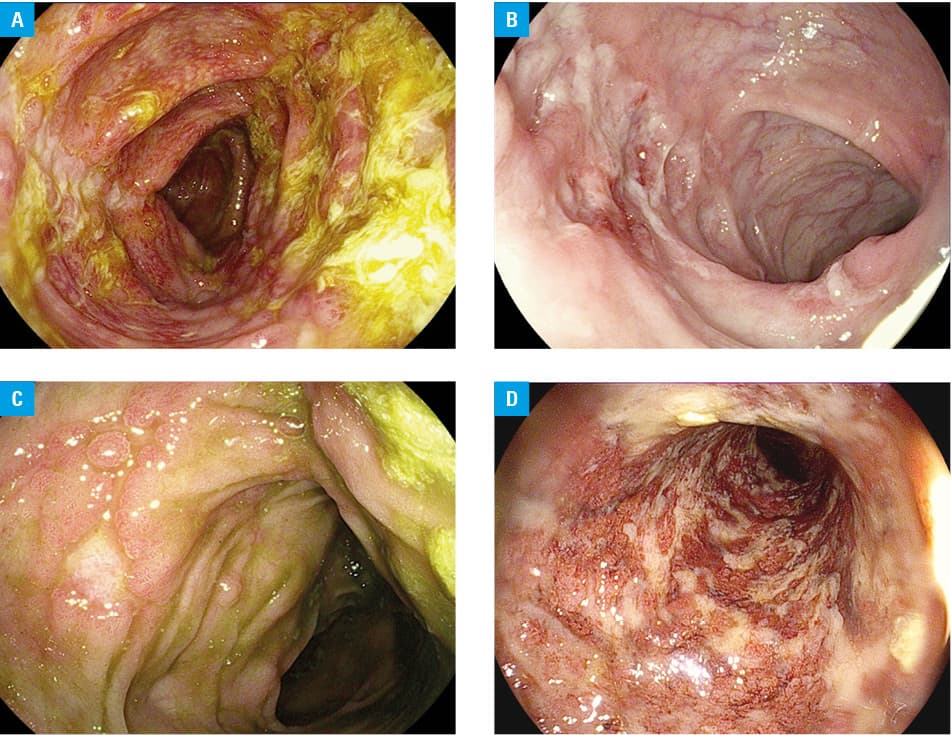
All patients presented with persistent bloody diarrhea, fever, abdominal pain, and weight loss. Physical examination showed abdominal tenderness in the right lower quadrant. Infectious causes were ruled out. Laboratory findings showed elevated inflammatory parameters. In each case, colonoscopy was performed and showed discontinuous inflammatory lesions, longitudinal ulcers, and aphthous ulcerations, mimicking inflammatory bowel disease (IBD). Histopathological findings, though not characteristic, bore some similarities to IBD.
The first patient (a woman aged 34 years), diagnosed with psoriasis 8 years ago, received secukinumab (anti‑interleukin [IL]-17A) for the past year (figure 1A). Another patient (a man aged 58 years), diagnosed with follicular lymphoma 3 years ago, was treated with rituximab (anti‑CD20; figure 1B). Two other men aged 65 and 73 years were treated with anti‑programmed cell death‑1 protein (PD‑1) agents due to metastatic renal cancer (nivolumab; figure 1C) and melanoma (pembrolizumab; figure 1D), respectively.
The first symptoms in all cases occurred within a few weeks to a few months of treatment. After cessation of immunotherapy and starting intravenous hydrocortisone, inflammatory markers decreased, and clinical symptoms eased. In 2 cases, the symptoms recurred a couple of weeks after discontinuation of steroids, and there was a need for restarting prednisone. All patients are monitored in outpatient settings.
The use of immunotherapy is increasing worldwide. Rituximab‑induced colitis is a well‑known side effect.1 However, its pathogenesis is poorly understood. It is speculated that CD20 lymphocytes can have immunoregulatory functions in the gut, and a blockade of this protein may lead to the activation of immune response in the gastrointestinal tract.2 Secukinumab has strong anti‑inflammatory properties by blocking IL‑17A, which is also believed to play an important role in the pathogenesis of IBD. Surprisingly, a clinical trial for secukinumab in Crohn disease had to be prematurely terminated due to a significant worsening of the disease’s inflammatory activity.3 The mechanisms underlying this paradoxical phenomenon are poorly understood.
In contrast to that, the pathophysiological background of colitis induced by the immune checkpoint inhibitors is well established.4 Blockade of cytotoxic T‑lymphocyte–associated protein‑4 (CTLA‑4) or PD‑1 activates immune response leading to cytotoxic effects on malignant cells. Immune checkpoint inhibitors revolutionized the therapy of several oncological disorders. However, the broader use of these drugs might be limited due to side effects resulting from their proinflammatory properties.
Since immunotherapy‑induced colitis resembles IBD, therapeutic algorithms share many similarities, although little is known about the long‑term prognosis in these difficult cases. Steroids are the first‑choice drugs; however, in a severe and / or relapsing disease course, biological therapy (anti‑TNF antibodies, vedolizumab, ustekinumab) can be considered.5 Thus paradoxically, monoclonal antibody‑induced colitis can be treated with other monoclonal antibodies.
- Mallepally N, Abu‑Sbeih H, Ahmed O, et al. Clinical features of rituximab‑associated gastrointestinal toxicities. Am J Clin Oncol. 2019; 42: 539‑545. | Crossref
- Eckmann JD, Chedid V, Quinn KP, et al. De novo colitis associated with rituximab in 21 patients at a tertiary center. Clin Gastroenterol Hepatol. 2020; 18: 252‑253. | Crossref
- Hueber W, Sands BE, Lewitzky S, et al. Secukinumab, a human anti‑IL‑17A monoclonal antibody, for moderate to severe Crohn’s disease: unexpected results of a randomised, double‑blind placebo‑controlled trial. Gut. 2012; 61: 1693‑1700. | Crossref
- Nishida T, Iijima H, Adachi S. Immune checkpoint inhibitor‑induced diarrhea/colitis: Endoscopic and pathologic findings. World J Gastrointest Pathophysiol. 2019; 10: 17‑28. | Crossref
- Abu‑Sbeih H, Ali FS, Alsaadi D, et al. Outcomes of vedolizumab therapy in patients with immune checkpoint inhibitor‑induced colitis: a multi‑center study. J Immunother Cancer. 2018; 6: 142. | Crossref
ARTICLE INFORMATION