Multichamber intracardiac thrombi successfully treated with apixaban in a patient with dilated cardiomyopathy and sinus rhythm



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Multichamber intracardiac thrombi successfully treated with apixaban in a patient with dilated cardiomyopathy and sinus rhythm
Multichamber intracardiac thrombi (MCICT) occur mainly in severe heart failure (HF) and / or in the presence of prothrombotic factors. The frequency of MCICT in HF and sinus rhythm has not been exactly determined. In patients with left ventricular (LV) thrombus, coexisting (locally formed) thrombi in the right ventricle (RV), right atrium (RA) and, alternatively, left atrium (LA) can rarely be found. Such patients are at increased risk of developing systemic and pulmonary embolism. There has been growing interest in intracardiac thrombi therapy replacing vitamin K antagonists (VKAs) with direct oral anticoagulants (DOACs) such as apixaban, rivaroxaban, edoxaban, and dabigatran. However, observations are particularly focused on left ventricular thrombi (LVT) and based mainly on case reports or case series1,2 as well as, more recently, on single multicenter cohort studies or retrospective studies3,4 comparing DOACs with VKAs.
A 60‑year‑old man with dilated cardiomyopathy was referred to our institution because of advanced HF with markedly decreased ejection fraction (15%; reference range >56%) and global longitudinal strain (–4%; reference range >–20%); no atrial fibrillation or flutter were observed. Transthoracic echocardiography (TTE) and transesophageal echocardiography revealed intracardiac thrombi involving 3 chambers (figure 1A, 1C, 1E, and 1G): a single one of irregular shape in the LV (6 × 2 cm), attached to the lateral wall and extending lengthwise to the apex; 3 oval ones near the RV apex (0.8–1 cm in diameter); and a single one of longitudinal shape arising from the RA appendage (4.5 × 1 cm). Thrombi were also detected on computed tomography, which additionally confirmed coexistent pulmonary embolism despite the absence of deep vein thrombosis. Anticoagulation with apixaban was started, initially at a dose of 10 mg twice daily (for 10 days), and then continued at 5 mg twice daily. Follow‑up TTE was performed every day for 2 weeks, then 3 times a week. Transesophageal echocardiography was repeated when the TTE image suggested a significant change of any thrombus. Thrombus resolution was monitored at different time intervals: in the RV after 2 weeks, in the LV after 3 weeks, and in the RA after 5 weeks (figure 1B, 1D, 1F, and 1H). No complications related to anticoagulation, particularly systemic and (new) pulmonary embolism or bleeding, were observed. Heart failure was treated with an angiotensin‑converting enzyme inhibitor, a β-blocker, and diuretics.
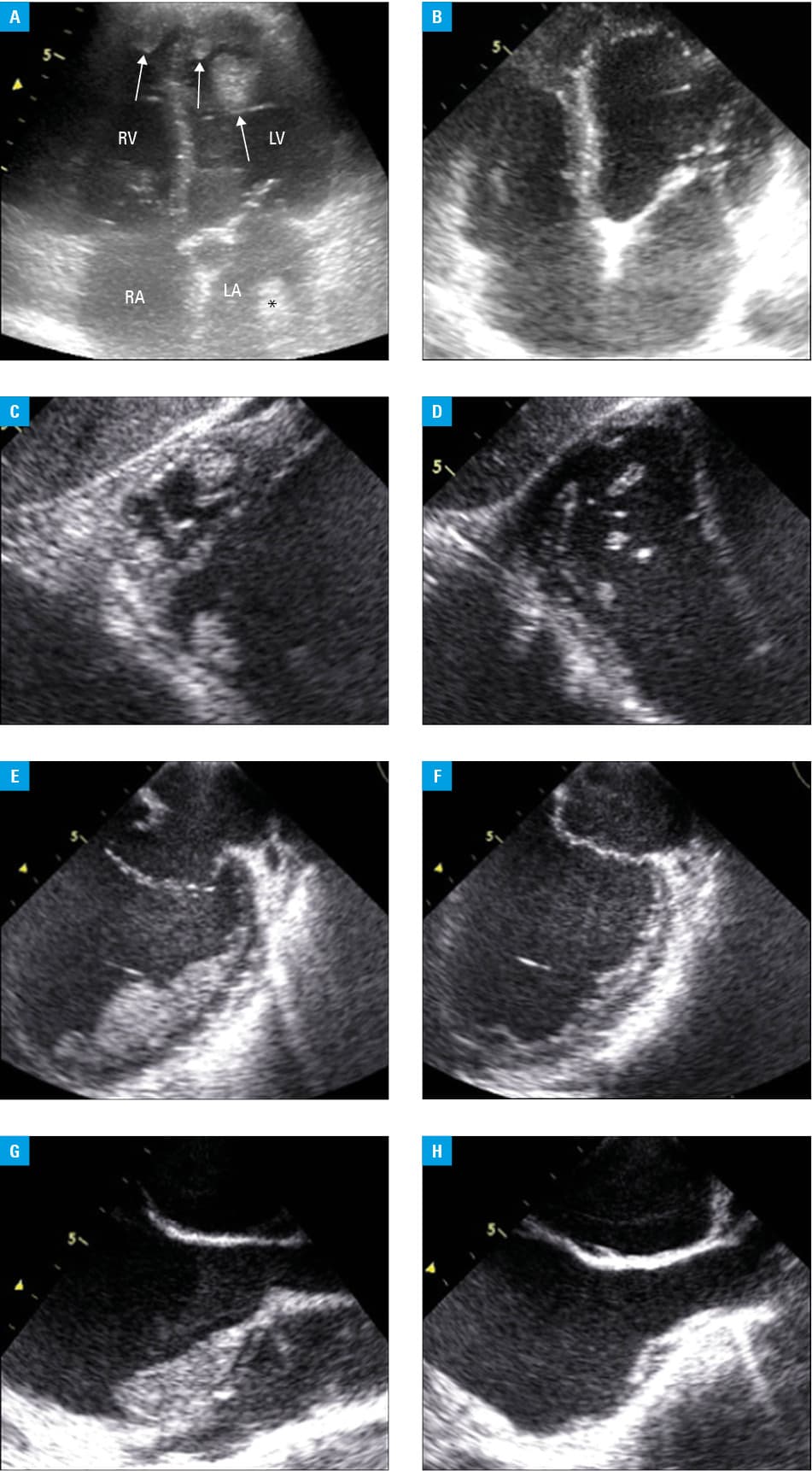
Abbreviations: LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle
The occurrence of MCICTs in patients with HF and sinus rhythm seems to be underestimated, because TTE may not detect all thrombi. Even a study including the largest number of patients with LVTs did not provide data on other coexisting intracardiac thrombi.4 Multichamber intracardiac thrombi were reported, eg, in myocarditis, dilated cardiomyopathy, and Behçet disease. Patients were usually treated with heparin or VKAs; none of them used DOACs. Studies on the effectiveness and safety of LVT treatment with DOACs have yielded conflicting results. Some authors suggest more frequent stroke episodes,3 while others claim that DOACs could constitute a valuable option of such therapy, although still off‑label.4 Therefore, randomized controlled trials are needed. Coexistent pulmonary embolism indicates a proper initial dose of DOACs, eg, 2 × 10 mg of apixaban and 2 × 15 mg of rivaroxaban. Permanent severe cardiac damage or irreversibly increased thrombotic risk promote long‑lasting therapy, which should prevent the recurrence of intracardiac thrombi. Of note, caution should be exercised with regard to implementing this therapy.5
- Daher J, Da Costa A, Hilaire C, et al. Management of left ventricular thrombi with direct oral anticoagulants: retrospective comparative study with vitamin K antagonists. Clin Drug Investig. 2020; 40: 343‑353. | Crossref
- Sedhom R, Abdelmaseeh P, Megaly M, et al. Use of direct oral anticoagulants in the treatment of left ventricular thrombi, a systematic review. Am J Med. 2020 Jun 19. [Epub ahead of print].
- Robinson AA, Trankle CR, Eubanks G, et al. Off‑label use of direct oral anticoagulants compared with warfarin for left ventricular thrombi. JAMA Cardiol. 2020; 5: 685‑692. | Crossref
- Iqbal H, Straw S, Craven TP, et al. Direct oral anticoagulants compared to vitamin K antagonist for the management of left ventricular thrombus. ESC Heart Fail. 2020 Jun 25. [Epub ahead of print]. | Crossref
- Pruszczyk P, Tomaszuk‑Kazberuk A, Słowik A, et al. Management of bleeding or urgent interventions in patients treated with direct oral anticoagulants: 2017 recommendations for Poland. Pol Arch Intern Med. 2017; 127: 343‑351. | Crossref
ARTICLE INFORMATION