Using the neutrophil-to-lymphocyte ratio to estimate the severity of coronavirus disease 2019



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Using the neutrophil-to-lymphocyte ratio to estimate the severity of coronavirus disease 2019
To the editor
We have read with great interest a recent article by Zeng et al,1 who described a notable relevance of the neutrophil‑to‑lymphocyte ratio (NLR) to identify patients with severe coronavirus disease 2019 (COVID‑19). As low levels of leukocytes and, conversely, high levels of neutrophils are observed in patients with a severe status of COVID‑19, the NLR can exaggerate the converse direction of neutrophils and lymphocytes. This finding is clinically useful, because the NLR is easily calculated during routine blood tests even at community clinics and hospitals (where many patients with COVID‑19 are seen).
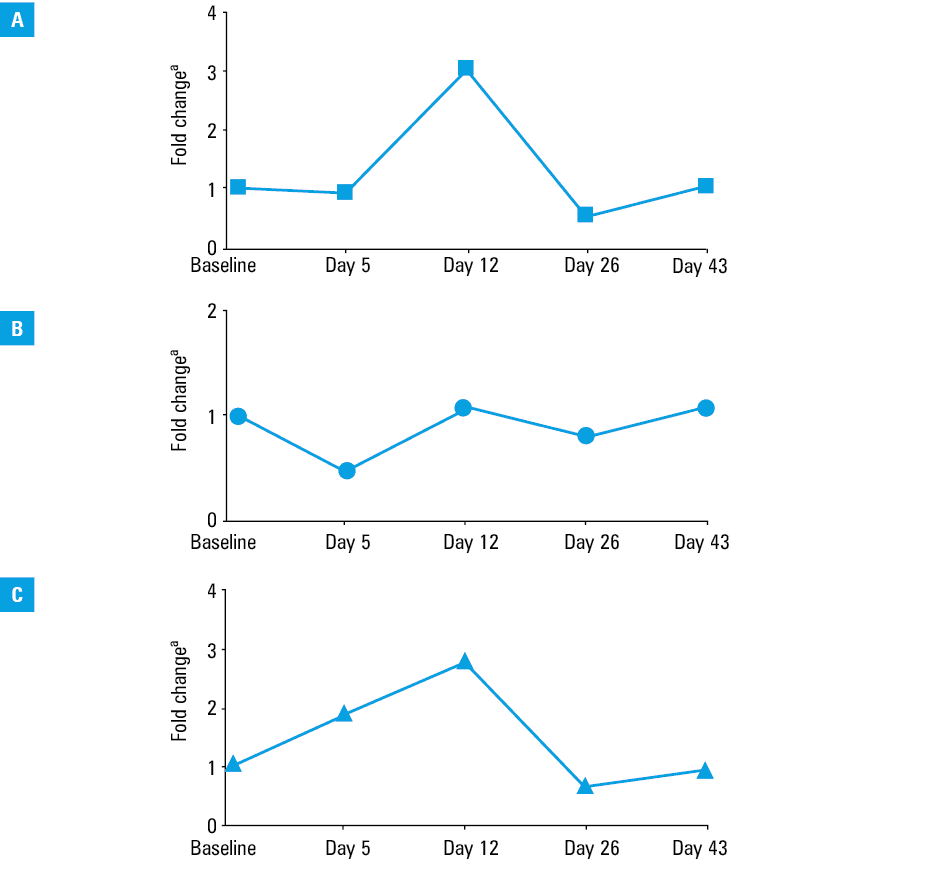
We would like to provide some suggestions related to the use of the NLR. Although the NLR measured at a single point was reported in most studies, as analyzed in the article by Zeng et al,1 the nadir (the lowest point) for leukocytes and the peak (the highest point) for neutrophils can differ during the clinical course of COVID‑19. For instance, early lymphopenia and late neutropenia have been reported during the course of influenza.2 In our experience of treating an adult patient with severe COVID‑19, such phenomena were indeed observed (Figure 1). Monitoring the NLR (eg, by the change rate) may produce a sensible finding of the disease conditions. Additionally, the cutoff values of the NLR remain to be determined in order to predict the severity of COVID‑19. It is seemingly necessary to establish the cutoff values considering the transiently different behaviors of both leukocytes and neutrophils. Further studies to effectively use the NRL are therefore warranted.
- Zeng F, Li L, Zeng J, et al. Can we predict the severity of coronavirus disease 2019 with a routine blood test? Pol Arch Intern Med. 2020; 130: 400‐406. | Crossref
- Sharon N, Talnir R, Lavid O, et al. Transient lymphopenia and neutropenia: pediatric influenza A/H1N1 infection in a primary hospital in Israel. Isr Med Assoc J. 2011; 13: 408‐412.
ARTICLE INFORMATION