Using the neutrophil-to-lymphocyte ratio to estimate the severity of coronavirus disease 2019. Authors' reply



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Using the neutrophil-to-lymphocyte ratio to estimate the severity of coronavirus disease 2019. Authors' reply
Authors’ reply
We would like to thank Prof. Kotani et al for their interesting comments to our article on the clinical value of the neutrophil‑to‑lymphocyte ratio (NLR) to estimate the severity of coronavirus disease 2019 (COVID‑19).1 Kotani et al closely tracked the dynamic changes of neutrophils, lymphocytes, and the NLR in a patient with severe COVID‑19 for 43 days from admission. They concluded that the NLR, a marker easily accessible from the routine blood test, could be used to predict the severity of COVID‑19, which was consistent with our previous finding.1
Furthermore, Kotani et al observed that the time of the leukocyte nadir is not the same as that of the neutrophil peak in a patient with severe COVID‑19. Lu et al2 and Sun et al,3 who observed patients with severe COVID‑19, supported the finding. We are not surprised by the observations. However, if you check the data carefully, you will find different dynamic changes even in neutrophils, lymphocytes, and the NLR between these patients with severe COVID‑19 (Figure 1). Besides, the dynamic changes were inconsistent even in patients with different degrees of disease severity.3 Based on that, more caution needs to be taken when drawing conclusions on the time difference between the leukocyte nadir and the neutrophil peak. More importantly, nowadays, there is no evidence suggesting that the difference could dampen the predictive value of the NLR, which reflects the progress of the disease course.3 Therefore, we should not care too much about the difference, but pay more attention to the dynamic change of the NLR.
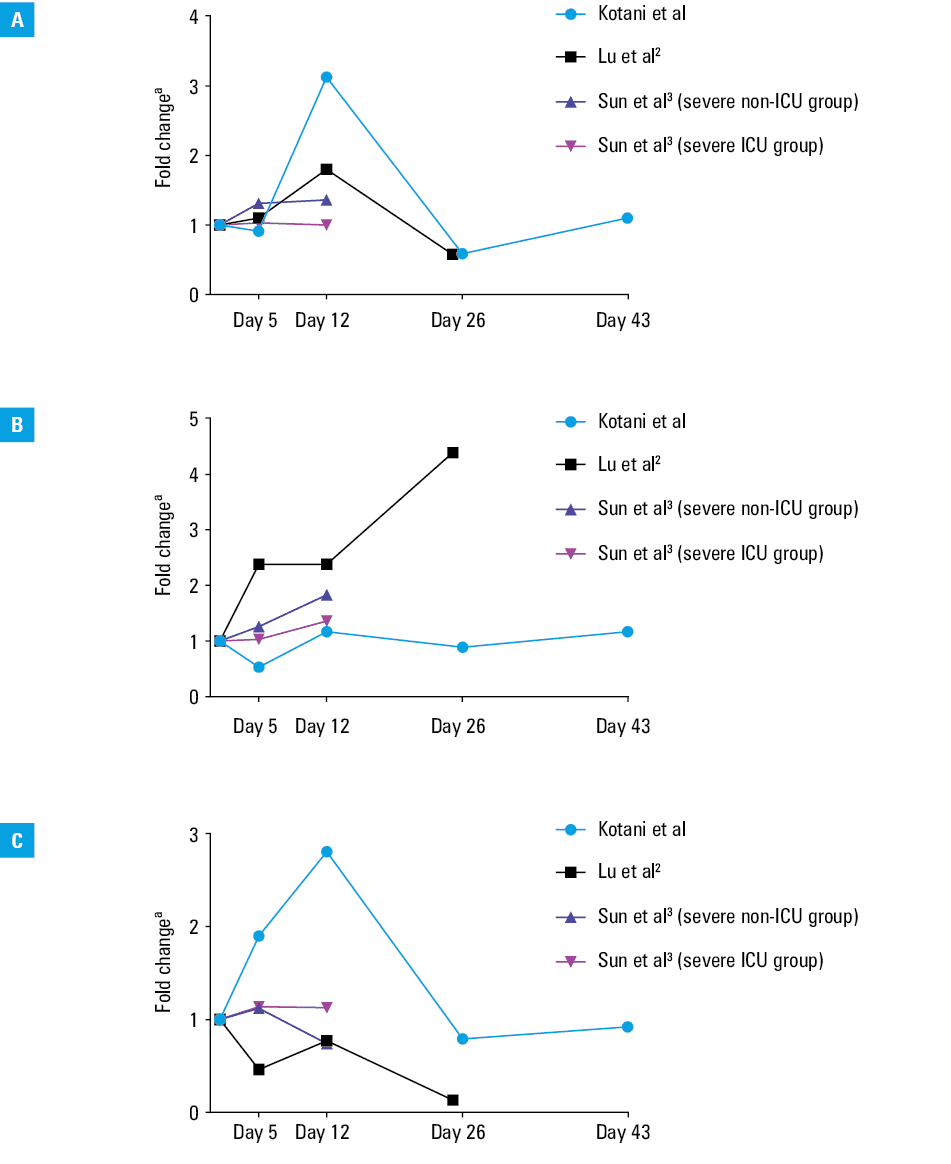
Abbreviations: ICU, intensive care unit
a Y axis shows changes in concentrations with regard to baseline values.Additionally, Kotani et al demonstrated that the cutoff of the NLR should be determined for clinical use. We appreciate their proposal and, nowadays, there are some studies on this issue. For example, through maximizing the Youden index in the receiver operating characteristic curve, Tatum et al4 identified 4.94, 9.95, and 11.4 as the NLR cutoffs for endotracheal intubation and mortality prediction on days 1, 2, and 5. They found out that the NLR is a prognostic factor for endotracheal intubation and an independent predictor of mortality risk in patients with COVID‑19. Moreover, Ma et al5 used the median as the cutoff (9.8) to divide the patients into 2 groups. They found that the high‑NLR group showed a higher incidence of acute respiratory distress syndrome and a higher rate of noninvasive and invasive mechanical ventilation. To conclude, the NLR cutoff should be determined according to the clinical purpose and disease progression. It is not reasonable to determine a specific value for the NLR cutoff in all clinical circumstances.
Thank you for your comments again. Taken together, the NLR is a prognostic predictor of COVID‑19 severity, but it is a long way to go to determine its cutoff in different clinical circumstances.
- Zeng F, Li L, Zeng J, et al. Can we predict the severity of coronavirus disease 2019 with a routine blood test? Pol Arch Intern Med. 2020; 130: 400‑406. | Crossref
- Lu G, Wang J. Neutrophil‑to‑lymphocyte ratio as a predictive biomarker for moderate‑severe ARDS in severe COVID‑19 patients. Clin Chim Acta. 2020; 508: 98‑102.
- Sun S, Cai X, Wang H, et al. Abnormalities of peripheral blood system in patients with COVID‑19 in Wenzhou, China. Clin Chim Acta. 2020; 507: 174‑180. | Crossref
- Tatum D, Taghavi S, Houghton A, et al. Neutrophil‑to‑lymphocyte ratio and outcomes in Louisiana COVID‑19 patients. Shock. 2020 Jun 19. [Epub ahead of print]. | Crossref
- Ma A, Cheng J, Yang J, et al. Neutrophil‑to‑lymphocyte ratio as a predictive biomarker for moderate‑severe ARDS in severe COVID‑19 patients. Crit Care. 2020; 24: 288. | Crossref
ARTICLE INFORMATION