Review of different clinical scenarios in patients with cardiovascular disease in the era of the coronavirus pandemic



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Review of different clinical scenarios in patients with cardiovascular disease in the era of the coronavirus pandemic
Introduction
Cardiovascular comorbidities are common in patients with coronavirus disease 2019 (COVID‑19) and associated with a greater risk of morbidity and mortality.1 This special report reviews clinical data on the impact of severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2) infection on patients with cardiovascular disease (CVD)1 (Figure 1). The spread of COVID‑19 requires attention to the immediate and long‑term cardiovascular implications of viral infection. This is of particular importance to patients with pre‑existing CVD.
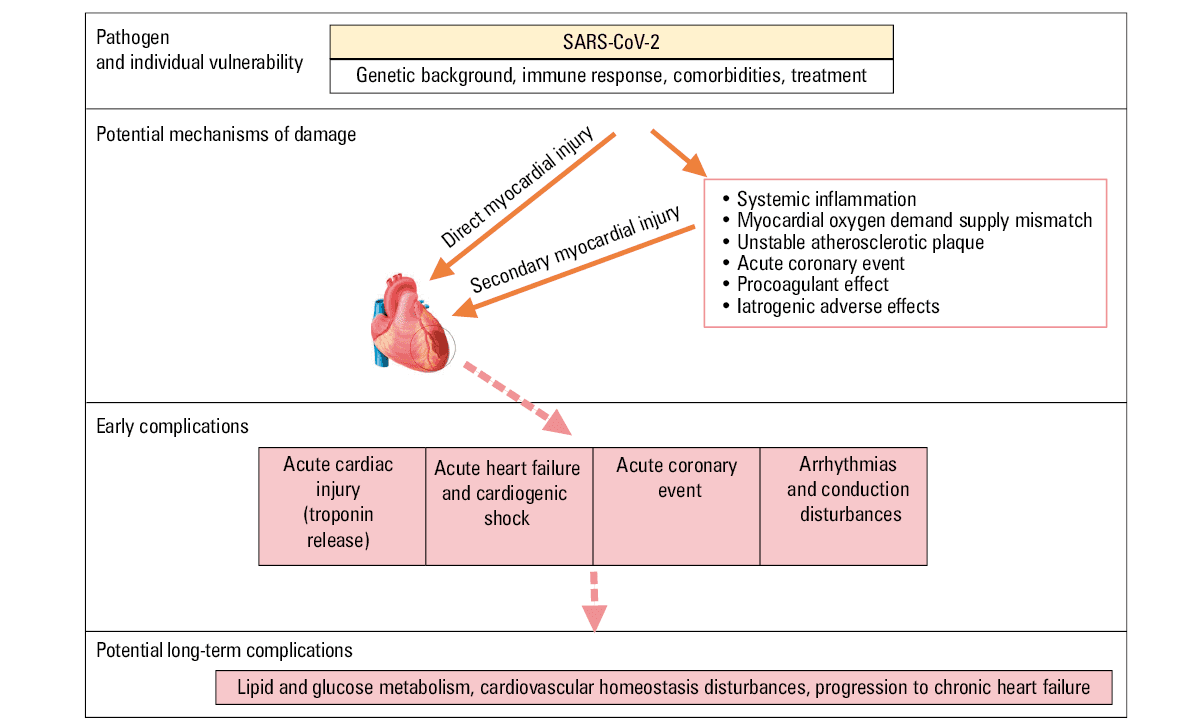
Abbreviations: SARS‑CoV‑2, severe acute respiratory syndrome coronavirus 2
Hypertension
Arterial hypertension is one of the most frequent comorbidities in patients with SARS‑CoV‑2 infection. A recent meta‑analysis of 6 studies including 1527 infected patients showed that the prevalence of hypertension, cardio- and cerebrovascular disease, and diabetes in that population was 17.1%, 16.4%, and 9.7%, respectively.1 What is more, the prevalence of comorbidities was higher among patients who were admitted to intensive care units (ICUs), required mechanical ventilation, or had fatal outcomes.2-5 However, according to current knowledge, hypertension is not an independent risk factor for worse outcomes in patients with COVID‑19.
Notably, the aforementioned comorbidities are often treated with renin–angiotensin system inhibitors, including angiotensin‑converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs). Their beneficial effect on cardiovascular outcomes has been demonstrated in numerous studies. However, recently, the potential of ACEIs and ARBs to cause unfavorable effects—specifically, an increased risk of SARS‑CoV‑2 infection and a more severe course of COVID‑19—has been suggested.6,7 Severe acute respiratory syndrome coronavirus 2 binds to its target cells through angiotensin‑converting enzyme 2 (ACE2)., which is expressed in the lungs, intestines, kidneys, blood vessels, and heart.6,7 In animal models, the upregulation of ACE2 expression in various organs resulted from ACEI and ARB treatment.8-10 Angiotensin‑converting enzyme 2 turns angiotensin II to angiotensin 1‑7, which has a protective role in the cardiovascular system and, potentially, a vasodilatory effect. Moreover, ACE2 prevents acute lung injury.11,12 Possible upregulation of ACE2 expression as a receptor for viral cell entry (with ACEIs or ARBs) may theoretically increase susceptibility to COVID‑19.
Interestingly, a contrasting hypothesis has also been postulated. Angiotensin receptor blockers have been suggested to act beneficially in patients with COVID‑19 by ACE2 upregulation, thus increasing the concentration of vasodilating angiotensin 1‑7 at the expense of angiotensin II causing vasoconstriction, which contributed to lung protection.13,14
Therefore, in the absence of firm evidence regarding beneficial or adverse outcomes of ACEI and ARB treatment in patients with COVID‑19, the European Society of Cardiology (ESC) as well as the American College of Cardiology and American Heart Association do not recommend discontinuation or any modification of clinically indicated therapy. The risk of discontinuing drug use is well known: it may destabilize blood pressure control and consequently increase cardiovascular mortality in patients with COVID‑19.15,16
Chronic coronary syndromes
Reports of outpatient and inpatient cohorts with COVID‑19 showed that 24% of patients had at least 1 comorbidity and 2.5% to 25% had chronic coronary syndromes (CCSs).2-5,17 They were more frequently observed in critically ill patients with respiratory failure (9%) and in nonsurvivors (24%). Chronic coronary syndromes were also a risk factor for in‑hospital death in univariable analysis (odds ratio [OR], 21.4; 95% CI, 4.64–98.76).3 It can be presumed that patients with coronary artery disease are susceptible to cardiac injury and complications from COVID‑19 leading to sudden deterioration.18
Acute inflammation can exacerbate the course of pre‑existing CCSs and may contribute to atherosclerotic plaque rupture leading to cardiovascular events. Therefore, administering drugs like aspirin, statins, β-blockers, and ACEIs, which have the potential to stabilize plaque, is strongly recommended by current guidelines on the management of CCSs.19
Due to the increased likelihood of stent thrombosis due to procoagulant effects of systemic inflammation, some experts advise doctors to assess platelet function and consider intensifying antiplatelet therapy, especially in patients with a history of previous coronary intervention.20
In the era of the COVID‑19 pandemic, numerous hospitals are limiting or cancelling elective diagnostic workup and treatment procedures. High‑risk patients on waiting lists should be prioritized. What is more, single‑day percutaneous coronary interventions (PCIs) should be considered to reduce the risk of transmission.21 As for treatment options, medical management or PCIs may need to be preferentially considered over coronary artery bypass grafting, if feasible, according to current guidelines. A reason for such approach is the limited number of ICUs, beds, and respirators. Second, there is currently a limited amount of packed red blood cells owing to an insufficient number of available blood donors.22
Acute coronary syndromes
The clinical presentation of acute coronary syndrome (ACS) may have signs and symptoms overlapping with those of COVID‑19, including nausea, isolated dyspnea, chest discomfort, fatigue, and tachycardia, making it challenging to differentiate between these 2 entities.23
While the optimal management strategy in patients with ACS during the COVID‑19 epidemic is being widely discussed, no ultimate consensus has been reached so far. Decisions should be individualized, considering the risk of SARS‑CoV‑2 exposure versus the risk of delay in diagnosis or therapy. However, in the case of ST‑segment elevation myocardial infarction (STEMI), it is reasonable to follow the guideline‑recommended treatment, which implies primary PCI within 90 minutes from first medical contact.24
In STEMI patients with active or suspected COVID‑19 in whom PCI is to be performed, appropriate personal protective equipment (PPE) should be worn, such as gowns, gloves, goggles, shields, and FFP2 / FFP3 masks. However, in our opinion, it is reasonable to assume that each patient is a potential SARS‑CoV‑2‑infected person. This assumption is based on the fact that 15% to 20% of infected patients remain asymptomatic yet capable of infecting others.25 Such a strategy, although it requires additional resources, ultimately minimizes the risk of personnel exposure and contamination of the catheterization laboratory. Adoption of these precautions should reduce the risk of catheterization laboratory quarantine or shutdowns, enabling full availability of primary PCI services in a continuous and uninterrupted fashion.
No specific recommendations to alter the routine PCI technique, stent selection, and periprocedural pharmacotherapy have been provided yet. However, in patients with acute cardiovascular and respiratory decompensation, intubation should be considered before admission to a catheterization laboratory, as emergency intubation, suction, and active cardiopulmonary resuscitation (CPR) in the catheterization laboratory setting is likely to result in generating aerosolized respiratory secretions increasing the likelihood of personnel exposure.
Of note, the pandemic may pose a threat to patients with STEMI, as it increases the risk of delayed primary PCIs, resulting from multiple factors. First, there seems to be a significant patient factor, which most probably results from patient reluctance to hospitalization. Specifically, as reported in a preliminary report from China,25 researchers noted a nearly 4‑fold increase in the time from symptom onset to first medical contact. Second, the availability of emergency medical transport may be limited owing to system overload and unavailability of some emergency medical response teams caused by post‑exposure quarantine. Last but not least, one can expect some hospital delay related to the need for providing additional safety procedures, as mentioned above and listed in a recent article.25
Due to the increased risk of delays from symptom onset to PCI, fibrinolysis and an early pharmacoinvasive strategy should be considered in patients with STEMI in whom the expected delay is longer than 90 minutes.
Patients with non–ST‑segment elevation myocardial infarction (NSTEMI) should undergo biomarker evaluation (ie, high‑sensitivity troponin) as well as symptom and electrocardiogram (ECG) monitoring, followed by risk stratification. According to current ESC guidelines, an immediate invasive strategy is recommended only in very high‑risk patients, which means that, in the majority of patients with NSTEMI, timing should allow for diagnostic testing for COVID‑19 prior to cardiac catheterization and more informed decision making regarding infection status.26 Of note, a troponin rise is observed in up to 17% of patients with COVID‑19, which is likely related to acute cardiac injury and / or type 2 myocardial infarction.3 That is why, in light of lack of any other signs of ischemia, conservative treatment should be considered as the default strategy.
Myocarditis
The actual incidence of myocarditis in patients with SARS‑CoV‑2 infection is impossible to be determined, as endomyocardial biopsy is used infrequently. Among more than 21 million known COVID‑19 cases worldwide, the scenario of clinically suspected myocarditis is uncommon. Using the search terms (“coronavirus” OR “SARS‑CoV‑2” OR “COVID‑19” AND “myocarditis”), there can be found only several dozens of case reports and a small number of retrospective studies reporting clinically suspected myocarditis—few using positive cardiac magnetic resonance imaging—but none of them were proven by biopsy.3,27-31 Cardiac magnetic resonance imaging should be performed in all cases of suspected myocarditis in order to increase the likelihood of proper diagnosis, but it increases the risk of facility contamination. What is more, sputum or nasal / throat swab testing is not sufficient to prove the association of clinically suspected myocarditis with SARS‑CoV‑2 infection, since only biomolecular testing (polymerase chain reaction or in‑situ hybridization) of the myocardial tissue provides definite diagnosis. In addition, SARS‑CoV‑2 is not among cardiotropic viruses that are known to be associated with myocarditis (like parvovirus B19, enterovirus, or adenovirus). In a single case report, autopsy showed only few interstitial mononuclear inflammatory infiltrates yet no signs of myocardial damage.32 However, it is postulated that there is a potential way of direct cardiac involvement through ACE2, the receptor for SARS‑CoV‑2.33 This theory requires further investigation.
Myocarditis is more common in children and young adults, may occur at middle age, and is rare in the elderly, while the median age of patients with COVID‑19 has been approximately 55 years, and comorbidities have been present in at least half of patients.1-4 In patients with COVID‑19, the predominant clinical presentation was pneumonia accompanied by signs and symptoms of systemic infection, while chest pain (2% of patients), palpitations, and / or arrhythmia were observed at low frequency.30,34 In the overall population, elevated natriuretic peptide and troponin levels were noted in a low proportion of patients (approximately 30% and 10% to 20%, respectively), with a higher prevalence among those requiring intensive care.4,35,36 Deceased patients had significantly more complications such as acute respiratory distress syndrome (ARDS), acute kidney injury, shock, and disseminated intravascular coagulation. In deceased groups, acute cardiac injury with elevated troponin and natriuretic peptide levels was also significantly more frequent than in survivors, which is likely due to multiorgan damage (including liver and renal failure), cytokine storm, or unknown etiology.37 There is evidence showing that acute infections are associated with an increased risk of myocardial damage.38 Abnormal troponin levels do not equate heart failure, myocarditis, or myocardial infarction in COVID‑19. Other potential mechanisms of troponin elevation include high myocardial oxygen demand accompanied by hypoxia due to acute respiratory failure, plaque rupture, and coronary thrombosis enabled by systemic inflammation and dyselectrolytemia, especially hypokalemia related to the interaction between SARS‑CoV‑2 and the renin–angiotensin system.1,20,39 Additionally, the drugs used in COVID‑19 such as antivirals, corticosteroids, chloroquine, and azathioprine may pose a risk of cardiac toxicity, interact with cardiac drugs, and prolong the QT interval, thus leading to arrhythmia.40 Therefore, current epidemiological data do not support the hypothesis that myocarditis is associated with COVID‑19, or that it is common.
In the abovementioned studies, patients with clinically suspected myocarditis were treated with corticosteroids, intravenous immunoglobulin (IVIG), or antiviral treatment (alone or in combination), although these agents have no proven beneficial role in clinically suspected myocarditis.41 According to the current ESC recommendations, immunosuppressive treatment or immunomodulation should be prescribed after ruling out the presence of the virus in the myocardium on endomyocardial biopsy.27 What is more, patients with COVID‑19 who received corticosteroids and / or IVIG did not benefit from this treatment or even had an increased risk of death.3 Use of corticosteroids in viral infection (a high risk of coinfection with other respiratory pathogens was also reported in COVID‑19) is controversial and may lead to reduced viral clearance and an increased risk of sepsis.42 Administration of IVIG for hypothetical myocarditis in COVID‑19 might be useless, since human IVIG does not contain immunoglobulin G against COVID‑19 (except for patients recovered from COVID‑19). It has also been postulated that up to 50% of patients with acute myocarditis show spontaneous healing.27
Intensive cardiac care
Current research shows that patients requiring ICU treatment were more likely to suffer from hypertension, diabetes, or ischemic heart disease.43,44 The infection may not only indirectly affect the circulatory system, exacerbating the symptoms of already existing diseases, but also directly contribute to the occurrence of specific diseases and cardiac complications (eg, myocarditis, ACS, myocardial injury, acute heart failure leading to cardiogenic shock, malignant ventricular arrhythmias, or venous thromboembolism). Most likely, this is due to uncontrolled immune response to the virus, resulting in acute neurohormonal stress, release of a large number of proinflammatory cytokines, which leads to significant disorders of the coagulation system.3 In addition, infection can lead to complications specific to COVID‑19 such as pneumonia, ARDS, septic shock, or multiorgan failure. All this means that individual disease syndromes can superimpose each other, which can greatly impede the diagnostic process and implementation of appropriate treatment. Prioritized patients with severe COVID‑19 should be referred to the ICU, where specific equipment and medical staff experienced in intensive care are available. However, it seems very likely that a patient with COVID‑19 will be transferred to an intensive cardiac care unit because of a primary cardiac disease or no ICU available.
This fact sets new challenges for cardiologists and certainly diverges from the current routine practice.
Available reports clearly show that the presence of CVD in patients infected with SARS‑CoV‑2 is associated with a dramatic increase in in‑hospital mortality when the existing cardiovascular pathologies are accompanied by respiratory failure, infectious myocardial damage, or new, treatment‑resistant cardiac arrhythmias.43
Heart failure
It has been shown that heart failure occurred in 52% of nonsurvivors and in 12% of survivors.3 Surprisingly, although respiratory disease is the major clinical manifestation of COVID‑19, the case‑fatality rate in patients with pre‑existing CVD is greater (10.5%) than in those with pre‑existing chronic respiratory disease (6.3%).43
Heart failure in patients with suspected or confirmed COVID‑19 should be managed according to the current guidelines.45 To limit the risk of viral exposure, it is recommended to avoid blood testing (to measure troponin and natriuretic peptide levels) or echocardiography in patients with COVID‑19, unless they are necessary and affect treatment.46 Treatment of acute left ventricular failure complicated by pulmonary edema in patients with COVID‑19 should follow the same rules as for noninfected individuals. The difficulty physicians face is to establish the cause of acute left ventricular decompensation and differentiate with noncardiogenic pulmonary edema caused by massive pneumonia or ARDS. Radiological symptoms are unreliable in the acute phase of edema and it is difficult to perform more advanced diagnostic workup owing to the patient’s clinical status. In this case, the initial inference should be probably based on assessing the dynamics of withdrawal of pulmonary edema symptoms in response to the use of typical pharmacological treatment. It should be assumed that persons who, despite treatment, develop respiratory failure symptoms leading to the need for mechanical ventilation, may show primary pulmonary or mixed pathology. Properly performed endotracheal intubation by qualified medical staff wearing PPE and patient sedation enable healthcare personnel to perform imaging, including chest computed tomography and lung ultrasound, which, in combination with serial arterial blood gas tests, will help establish diagnosis and implement appropriate treatment.47 The management of patients with COVID‑19 should follow the accepted principles, yet with a special emphasis on patients’ prognosis.48
Pulmonary embolism
Pulmonary embolism is another cardiac condition that requires treatment in the intensive cardiac care unit and it may occur as a direct consequence of COVID‑19. Patients with COVID‑19 are at increased risk of developing venous and arterial thromboembolism. In hemodynamically unstable patients, rescue fibrinolysis should be used or, in case it is ineffective, surgical or percutaneous thrombectomy can be considered. In many cases, this may unfortunately involve the need to transfer the patient to a center offering highly specialized treatment and simultaneous access to hemodynamic support. It seems that, especially in the era of COVID‑19, such decisions regarding treatment of severe pulmonary embolism should be made by interdisciplinary teams. According to the current guidelines, low‑risk patients may be hospitalized shortly and should be discharged on oral treatment after exclusion of viral infection.3
Acute aortic syndrome
Patients with acute aortic syndrome should be referred to cardiac surgery centers after establishing their serological status, if testing is allowed in their state. If serological evaluation is unavailable, the abnormalities seen on chest computed tomography may support the decision to take appropriate precautions to prevent virus transmission.
Diverse principles in ventilation support
Interestingly, noninvasive ventilation (continuous positive airway pressure and bilevel positive airway pressure) is the recommended first‑line method of ventilation support in selected patients with acute heart failure.49 Currently, it is not advised to use it owing to the high risk of virus transmission to medical staff, and the preferred methods include endotracheal intubation and mechanical ventilation. As experts suggest, a strategy should be adopted to identify patients who will require intubation in the near future in order to avoid performing a procedure with a high risk of virus transfer without adequate protection of the personnel with PPE. The passive methods include using only high‑flow nasal catheters and face masks, without positive inspiratory pressures. The National Early Warning Score 2 comprises the following criteria: respiratory rate, hypercapnic respiratory failure, room air or supplemental oxygen, temperature, systolic blood pressure, pulse, and the consciousness level. The score is now validated for patients with COVID‑19.
In severe ARDS, it is recommended to adjust ventilation therapy to serial arterial oxygen pressure values. Frequently, there is a need to use high posiitive end‑expiratory pressure (PEEP; 4–6 mm of H2O under normal conditions) values with relatively small inspiratory volumes (4–6 ml per 1 kg of body weight). However, the increased value of PEEP may not be sufficient to improve oxygenation.47 Simultaneously, increased PEEP may worsen hemodynamic instability and hypotension. In this case, the effectiveness of ARDS treatment will be significantly limited by poor hemodynamic parameters and a consequent need for extracorporeal membrane oxygenation therapy.50
Cardiopulmonary resuscitation
Some modifications regarding CPR procedures in patients with COVID‑19 should be emphasized. The key recommendation is to identify patients who may require CPR as early as possible in order to ensure required equipment and avoid performing CPR without personal protection. The National Early Warning Score 2 can help recognize patients at increased risk.
Importantly, it is recommended to start compression‑only CPR with the quick assessment of the patient’s cardiac arrest rhythm, until endotracheal intubation with full PPE protection is provided. Mouth‑to‑mouth ventilation should not be used in order to limit aerosol spread. In the case of shockable rhythms (hemodynamically unstable ventricular tachycardia or ventricular fibrillation), it is advised to perform defibrillation as soon as possible.17
Potential serious adverse events of currently proposed treatment protocols in coronavirus disease 2019
Based on the encouraging results of preliminary studies, chloroquine / hydroxychloroquine and azathioprine have been widely prescribed to patients with COVID‑19. However, these drugs favor QT interval prolongation and, therefore, may provoke subsequent ventricular arrhythmia, including torsade de pointes, and are not currently recommended. Clinicians taking care of patients with COVID‑19 should be aware of potential adverse cardiovascular effects of proposed therapeutic options. Moreover, adequate monitoring of treatment safety is warranted, especially in highly vulnerable patients with underlying cardiac, renal, or hepatic dysfunction and in those receiving medications known to cause QT interval prolongation.40
Arrhythmia, ablation, and implantable devices
In patients with COVID‑19, the risk of arrhythmia is increased due to possible heart failure, suspected myocarditis, proinflammatory effects, cardiac injury, and increased sympathetic stimulation. Although arrhythmia is listed among potential cardiovascular complications of SARS‑CoV‑2 infection, a precise distribution of various heart rhythm disturbances is not available.
Nonspecific heart palpitations were reported in 7.3% of 137 patients admitted due to COVID‑19.34 In 138 patients with COVID‑19 who were hospitalized in Wuhan, cardiac arrhythmia was noted in 16.7% of them and more commonly seen in ICU patients (44.4%) compared with non‑ICU patients (6.9%).4 Unfortunately, the types of arrhythmia were not specified in those reports. In another study evaluating the association between underlying CVD and myocardial injury with fatal outcomes, patients with high troponin T levels presented a higher incidence of malignant arrhythmias compared with those with normal levels (11.5% versus 5.2%).49
In patients with CIEDs who are already followed up with remote monitoring and do not require in‑person evaluation, it is recommended to consider replacing routine visits with remote visits (eg, via video or telephone, remote CIED monitoring). In other patients, it is advised to enroll them in remote monitoring. Ambulatory monitors can also be mailed to patients without CIEDs who require rhythm monitoring. Electrocardiogram acquisition by a smartphone or a smartwatch may be considered. Routine in‑hospital in‑person device interrogation in stable patients in long‑term care facilities is not recommended.51
Telemedicine
A global pandemic was officially announced on March 11, 2020 by the World Health Organization.52 The spread of SARS‑CoV‑2 across the world has changed the organization of numerous industries, including the healthcare system, which had to adjust to prevailing conditions and clinical demands. Telemedicine accelerated its growth, limiting social contact at the same time, which includes limiting regular medical appointments. Use of telemedicine had been recommended by international societies before the emergence of the COVID‑19 pandemic.53,54 However, there have always been some barriers, which stopped the expansion of telemedicine.55 Reorganization of healthcare systems, clinicians’ reluctance, poor computer skills, and small financial reimbursement are listed among the reasons for its slow development observed so far.56
Nonetheless, physicians across the world are nowadays forced to provide consultations using mobile phones and computers in order to stop the virus spread and enable the treatment of patients, especially those isolated or during quarantine. Medical teleconsultation has been legalized by several governments. This approach is also evidence‑based and has been justified by several randomized trials. Video consultations proved to be a useful, financially profitable tool and showed high satisfaction rates among both patients and physicians, without differences in disease progression.57-59
However, we should be careful in selecting patients for consultations due to reasons other than those related to COVID‑19 and identify those who can and will benefit from this solution. Patients whose general condition is unstable or require acute care still need to have a traditional visit scheduled.
Telecare can abolish barriers to receiving cardiac care during the SARS‑CoV‑2 pandemic. First of all, telecare diminishes patient exposure, thus reducing the risk of infection. Second, it resolves patient problems with transportation during a pandemic, when public transport is not recommended. What is more, this solution will allow for a better allocation of hospital beds to the seriously ill patients or those with COVID‑19.
For the sake of safety, it is necessary to review upcoming appointments in advance to identify 3 groups of patients: 1) those who must be seen face‑to‑face (traditional visit); 2) those who might be seen virtually (telecare visit); 3) those who can be safely rescheduled a few months later, at a more appropriate time posing a lower risk of infection (postponed visit).
Of note, some practical issues of telecare should be discussed here. There are various types of virtual visits such as video consultation and consultation by phone or a special dedicated system for e‑consultations. During virtual visits, physicians can review results from previous examinations together with patients and discuss vital sign trends from remote monitoring. Televisits can be aimed at educating patients about the disease process and treatment targets. Education and counseling on diet or physical activity can also be provided in this way.
Another form of telecare, apart from televisits, is the remote monitoring of implanted cardiac devices using special, dedicated systems. It is recommended to call every patient whose scheduled visit for routine monitoring and reprogramming of cardiac devices cannot be conducted in order to assess their medical status (new symptoms such as dizziness, loss of consciousness, history of shock delivery).60-62
Key points
Several take‑home messages regarding the management of CVD in the era of the COVID‑19 pandemic can be derived from this review:
-
Patients with cardiovascular risk factors and CVD are at greater risk of morbidity and mortality related to COVID‑19.
-
In acute cardiac conditions such as ACS, heart failure, and cardiogenic shock decisions on the management strategy should be taken on a case‑by‑case basis, considering the risk of exposure to SARS‑CoV‑2 versus the risk of delay in diagnosis or therapy.
-
Troponin release is a common and multifactorial cardiac manifestation of COVID‑19 and is associated with an increased risk of morbidity and mortality.
-
Myocarditis is highly overdiagnosed as one of the common cardiac complications of COVID‑19, but there is no firm evidence showing that SARS‑CoV‑2 is a novel cardiotropic virus causing direct cardiomyocyte damage. The term ‘myocarditis’ should be used only for diagnosis confirmed by endomyocardial biopsy or autopsy.
-
Various non–evidence‑based treatment strategies in patients with COVID‑19 (ie, antivirals, corticosteroids, chloroquine, and azathioprine) may pose a risk of cardiac toxicity and should not be used at all or with extreme caution.
-
The global COVID‑19 pandemic poses challenges to healthcare systems. Implementing telemedicine solutions for daily care is beneficial, particularly in patients with stable, chronic diseases. However, it should not delay the management of patients who require in‑person visits.
- Li B, Yang J, Zhao F, et al. Prevalence and impact of cardiovascular metabolic diseases on COVID‑19 in China. Clin Res Cardiol. 2020; 109: 531‑538. | Crossref
- Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020; 382: 1708‑1720.
- Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID‑19 in Wuhan, China: a retrospective cohort study. Lancet. 2020; 395: 1054‑1062. | Crossref
- Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus‑infected pneumonia in Wuhan, China. JAMA. 2020; 323: 1061‑1069. | Crossref
- Zheng YY, Ma YT, Zhang JY, Xie X. COVID‑19 and the cardiovascular system. Nat Rev Cardiol. 2020; 17: 259‑260. | Crossref
ARTICLE INFORMATION