Necrotizing fasciitis secondary to the immunosuppressive treatment of eosinophilic fasciitis: radiological imaging, treatment modalities, and outcome



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Necrotizing fasciitis secondary to the immunosuppressive treatment of eosinophilic fasciitis: radiological imaging, treatment modalities, and outcome
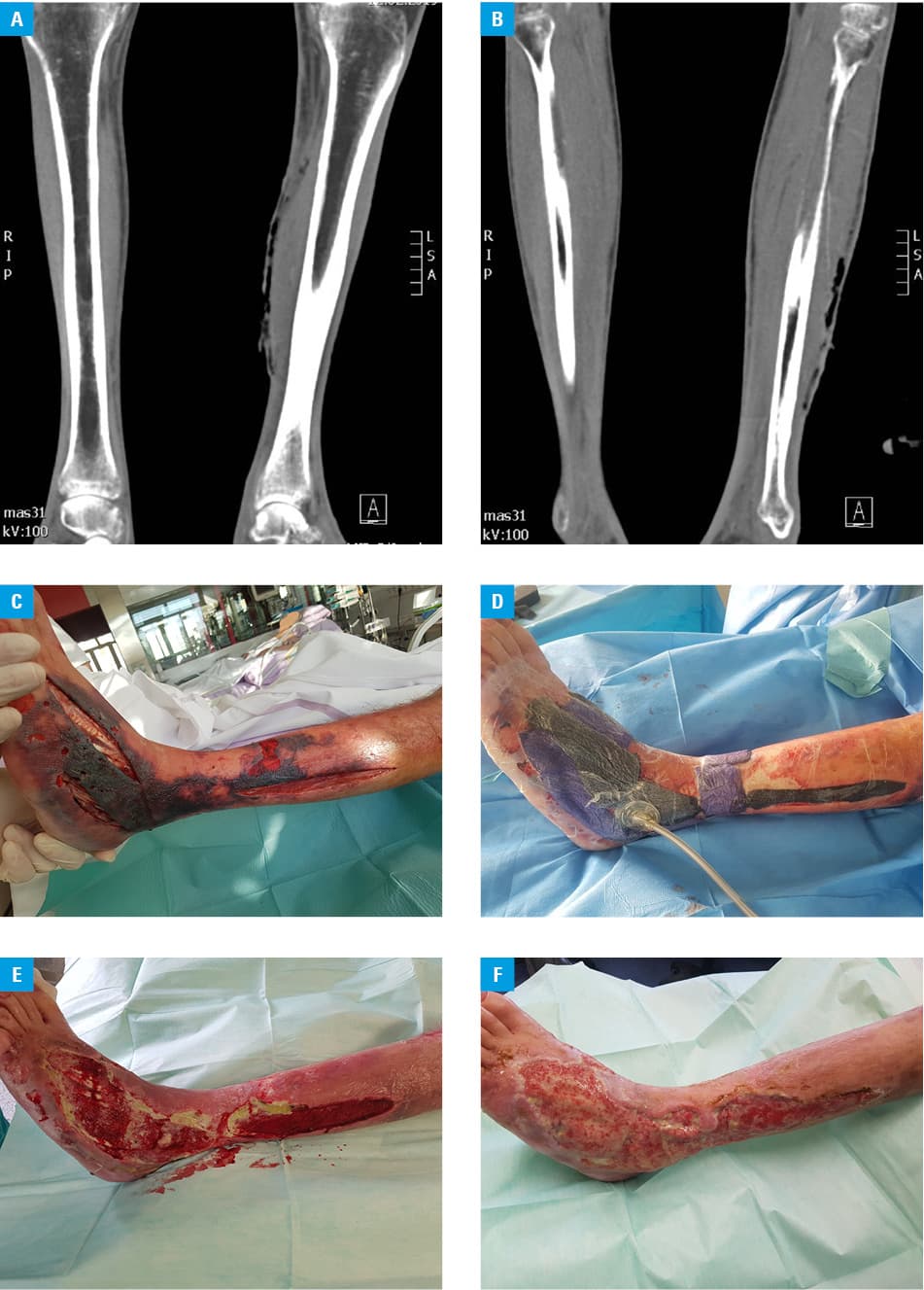
A 60‑year‑old Caucasian man in a good overall condition presented with a history of ankle edema and skin reddening, followed by persistent severe myalgia symmetrically affecting lower extremities. The symptoms escalated, leading to skin rash most prominent in the ankle region. On examination, the range of motion in the lower and upper limbs was decreased due to the developing hardening of the skin and fascia. Blood tests revealed mild hypoalbuminemia at 30.7 g/l and the elevated C‑reactive protein level of 429 nmol/l (reference range, 0–48 nmol/l). Differential blood count showed absolute and relative eosinophilia, with the total leukocyte count of 7.34 × 109/l and 27% of eosinophils. Prior to the diagnosis, the patient was evaluated by various consultants, including an infectious disease specialist and a rheumatologist. Lyme disease was suspected and Borrelia burgdorferi testing was performed. An enzyme‑linked immunospot assay indicated weak cellular activity against B. burgdorferi. The patient was treated for Borrelia infection with antibiotics and hyperthermia. The antinuclear antibody titer was marginally increased (1:80), while anti–extractable nuclear antigen antibodies and antineutrophil cytoplasmic antibodies remained within normal limits. Myofascial biopsy revealed inflammatory myopathy with mostly lymphocytic infiltrates in the perimysium, endomysium, and fascia. Apart from lymphocytes and macrophages, eosinophils were occasionally found. Based on these findings, 4 months after symptom onset, the diagnosis of eosinophilic fasciitis (EF) was established. Methylprednisolone at a dose of 48 mg/d (with dose reduction of 4 mg weekly until 16 mg) and methotrexate at a weekly dose of 15 mg were administered. Four months after treatment, the patient was admitted to the Department of Surgical Infections in Ljubljana (Slovenia) with type II necrotizing fasciitis (NF) of the left lower limb. On admission, the patient was febrile, hypotensive, had altered mental status, a C‑reactive protein level of 2410 nmol/l, disease hallmarks on computed tomography (CT; Figure 1A and 1B) and septic shock. The patient received antibiotic therapy with imipenem and clindamycin. Methotrexate was discontinued, and methylprednisolone substituted with hydrocortisone. Fasciectomy (Figure 1C) and debridement were performed. After a few days, the patient stabilized. Postfasciectomy wound therapy using negative pressure (Figure 1D) and a hyperbaric oxygen chamber (Figure 1E and 1F) was initiated.
Eosinophilic fasciitis is a rare disease: less than 300 cases were reported between 1977 and 2012. Borrelia burgdorferi is the main postulated EF trigger, which is in line with our observations.1 Eosinophilic fasciitis may mimic NF on magnetic resonance imaging and CT, which adds to the complexity of its radiological interpretation. In both EF and NF, dermal thickening, increased soft tissue opacity, and thickening or edema of myofascial structures can be observed. In this case, CT changes were accompanied by gas collection, which is typical of NF.2 Necrotizing fasciitis is a medical emergency. Out of the established for risk factors NF, such as diabetes and peripheral vascular diseases, only immunosuppression and advanced age were present in our patient’s case.3 Since this is the first report of EF followed by NF, it is impossible to assess if the eosinophilic inflammation of the fascia was an additional local risk factor for necrosis development. Corticosteroid therapy can provoke NF relapse; therefore, alternative treatment should be considered. Treatment options include infliximab, which proved to be effective in several patients with EF,4 as well as psoralen and ultraviolet A therapy.5 Since the treatment of EF may cause NF, it should be carefully monitored.
- Turan Y, Şendur ÖF, Karataş-Berkit I, et al. Eosinophilic fasciitis: a case report and review of the literature. Turkish J Rheumatol. 2010; 25: 208‑213. | Crossref
- Chaudhry AA, Baker KS, Gould ES, Gupta R. Necrotizing fasciitis and its mimics: what radiologists need to know. Am J Roentgenol. 2015; 204: 128‑139. | Crossref
- Das DK, Baker MG, Venugopal K. Risk factors, microbiological findings and outcomes of necrotizing fasciitis in New Zealand: a retrospective chart review. BMC Infect Dis. 2012; 12: 348. | Crossref
- Khanna D, Agrawal H, Clements PJ. Infliximab may be effective in the treatment of steroid‑resistant eosinophilic fasciitis: report of three cases. Rheumatology (Oxford). 2010; 49: 1184‑1188. | Crossref
- Schiener R, Behrens‑Williams SC, Gottlöber P, et al. Eosinophilic fasciitis treated with psoralen‑ultraviolet: a bath photochemotherapy. Br J Dermatol. 2000; 142: 804‑807. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION