Assessment of the risk of incident heart failure in patients with osteoporosis: a systematic review and meta-analysis of eligible cohort studies
Key words: incident heart failure, meta-analysis, osteoporosis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Assessment of the risk of incident heart failure in patients with osteoporosis: a systematic review and meta-analysis of eligible cohort studies
Introduction: A relation between cardiovascular diseases and bone health is increasingly reported. However, the association between osteoporosis and incident heart failure (HF) has not been yet determined.
Objectives: We aimed to summarize available evidence to evaluate whether osteoporosis was associated with an increased risk of incident HF.
Patients and methods: Major databases, including PubMed, Embase, the Cochrane library, Web of Science, and ClinicalTrials, were searched for cohort studies reporting the hazard ratio (HR) for incident HF in patients with osteoporosis. The pooled hazard ratios (HRs) and 95% CIs were estimated by using a random‑effects model. Heterogeneity was evaluated by the I2 statistics and the χ2 test.
Results: Three studies with a total of 70 697 patients were included, with the mean (SD) age of 62.9 (13.3) years. Osteoporosis was associated with an increased overall risk of incident HF (pooled HR, 1.17; 95% CI, 1.08–1.26; P <0.001; heterogeneity I2 = 13.28%, P = 0.32). The risk of incident HF was elevated in osteoporotic men (HR, 1.3; 95% CI, 1.05–1.62; P = 0.02; I2 = 71.57%, P = 0.03); however, no significant association was found for women (HR, 1.14; 95% CI, 0.94–1.37; P = 0.19; I2 = 64.66%, P = 0.06). The association between osteoporosis and incident HF risk was positive among individuals of Asian ethnicity (HR, 1.18; 95% CI, 1.06–1.3; P = 0.002; I2 = 52.61%, P = 0.15).
Conclusions: Osteoporosis was associated with a modest but significantly increased risk of incident HF. Considering the limited number and quality of available studies, future high‑quality data are required to further demonstrate the association between osteoporosis and incident HF.
What's new?
The association between bone health and cardiovascular diseases was observed in previous studies. However, whether osteoporosis is related to incident heart failure remains debatable. Data concerning the risk of incident heart failure in osteoporotic patients were systematically reviewed in the present study. We reported an increased overall hazard ratio of incident heart failure in patients with osteoporosis when compared to those without.
Introduction
Heart failure (HF) is a clinical syndrome caused by structural and / or functional cardiac abnormality, resulting in pulmonary and / or systemic congestion and insufficient organ perfusion.1 It usually manifests typical symptoms such as breathlessness, fatigue, and lower limb swelling, which may be accompanied by signs such as pulmonary crackles, peripheral edema, jugular vein engorgement or even distension. The diagnostic workup of HF requires a thorough assessment of symptoms, signs, clinical history, blood biomarkers (eg, B‑type natriuretic peptide, N‑terminal pro‑B‑type natriuretic peptide), and echocardiographic estimates (eg, ejection fraction). Its incidence increases with age. It is reported to be the most common cardiovascular reason for hospitalization in people over 60 years of age and it is associated with a poor prognosis.1-3 It not only greatly impairs patient quality of life and life expectancy but also imposes a heavy burden on the healthcare system.
In terms of etiology, HF is a heterogeneous disorder (eg, coronary artery disease [CAD], hypertension, and diabetes). Substantial effort has been made to treat the underlying causes. However, more risk factors are being suggested with the advancement of knowledge. Osteoporosis, characterized by low bone density and increased bone fragility, is also an age‑dependent disease with high morbidity, affecting up to 200 million people worldwide.4 Low bone mass was reported to be related to cardiovascular diseases.5 It was also found that osteoporosis and HF share common risk factors, such as advanced age, vitamin D deficiency, renal disease, and other comorbidities.6,7 Heart failure is a known risk factor for osteoporosis and vice versa.8-10 However, most of reported studies discussing the association between osteoporosis and HF have a cross‑sectional design. The question whether osteoporosis is related to an increased risk of future HF remains to be answered, which requires longitudinal data. But to date, clinical data regarding the relationship between osteoporosis and the risk of incident HF have been scarcely reported. Thus, the purpose of this study is to assess the risk of incident HF in osteoporosis patients through a systematic review of eligible cohort studies.
Patients and methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta‑Analyses (PRISMA) statement. (Supplementary material, tables S1 and S2)
Search strategy
Two independent reviewers (CC and ZLY) performed database searches in PubMed, Embase, the Cochrane library, Web of Science, and ClinicalTrials by using the following items: (heart failure OR heart insufficiency OR cardiac insufficiency OR myocardial insufficiency OR myocardi* failure OR cardia* failure OR heart decompensation OR cardiac decompensation OR myocardial decompensation) AND (osteoporosis OR osteoporos* OR osteopenia OR bone mineral density OR bone density OR bone densit* OR bone conten* OR bone loss*), from inception to April 16, 2019. There was no language restriction in our searches. We also performed a limited updated search from April 16, 2019 to June 21, 2020. Detailed search strategies in each database are reported in Supplementary material, tables S3-S7.
Eligibility criteria and study selection
Studies were eligible if they met the following criteria: 1) had a longitudinal design; 2) included patients with osteoporosis or osteopenia (defined by bone mineral density [BMD] assessment using any validated tool according to a clear standard diagnostic criteria or any documented medical or insurance records); 3) included a control group (with normal BMD, or without osteoporosis); 4) the endpoints were incident HF (defined as diagnosis information from any medical or insurance records or self‑reported HF based on a physician diagnosis confirmed by standard diagnostic criteria using medical records documenting series of symptoms, physical signs, and other supporting clinical findings); and 5) provided hazard ratio (HR) for incident HF. The primary outcome of our analysis was the risk of incident HF in patients with osteoporosis, assessed through HRs for incident HF.
Two authors (GZJ and YYY) developed the lists of studies independently during the selection process. A third author (CC) was prepared to adjudicate the lists, and discussed with the above 2 authors to reach a consensus if discrepancies were found. If 2 studies were based on the same cohort, the study with bigger sample size was included. The references of included articles were searched to identify additional potentially relevant publications. We also considered conference abstracts in our database searches. We contacted the corresponding authors to acquire the data to evaluate the eligibility of potentially relevant conference abstracts.
Data extraction and quality assessment
Two reviewers (CC and ZLY) independently extracted data from the included studies using a standard form. Disagreements between the 2 reviewers were solved by a formal discussion to reach a consensus. Data were extracted on: 1) basic characteristics of included studies (first author, publication year, country, race, number of patients, mean age, percentage of female patients, follow‑up period, adjusted covariates); 2) descriptions of exposure measurement (osteoporosis or osteopenia) and endpoint (incident HF); and 3) outcome data (hazard ratio). The quality of prognostic studies was assessed according to the recommendations by Hayden et al11 using the following domains: study participation, study attrition, prognostic factor measurement, outcome measurement, confounding measurement and control, and analysis. Two reviewers (GZJ and YYY) performed the quality assessment of each of the included studies independently. Discrepancies were solved by discussion with a third reviewer (ZLY). The domains would be rated as yes, partly, unsure, or no for its appropriateness, respectively.
Statistical analysis
We performed a random‑effects meta‑analysis using Comprehensive Meta‑Analysis (CMA) 2.0 (Biostat, Englewood, New Jersey, United States).12 In the primary analysis, we calculated the pooled HR and 95% CI from all included studies. We only included the HR adjusted for the highest number of covariates for each study. The same procedure was performed in the post hoc subgroup analysis. Study heterogeneity was evaluated by using the I2 statistics and the χ2 test. A value of over 50% for the former and a P value of less than 0.05 for the latter suggested significant moderate or higher heterogeneity.13 Sensitivity analyses were conducted as follows: First, a fixed‑effect model was additionally used to estimate the pooled HR of all included studies in order to compare with a random‑effects model. Secondly, we estimated the respective HRs by a random‑effects model by excluding one study at a time. Publication bias was not performed because of the limited number of included studies (less than 10) in the present review. A P value of less than 0.05 was considered significant.
Ethics statement
This study was approved by the Academic Administration Committee of Maoming People’s Hospital. Informed consent was not required.
Results
Description of included studies
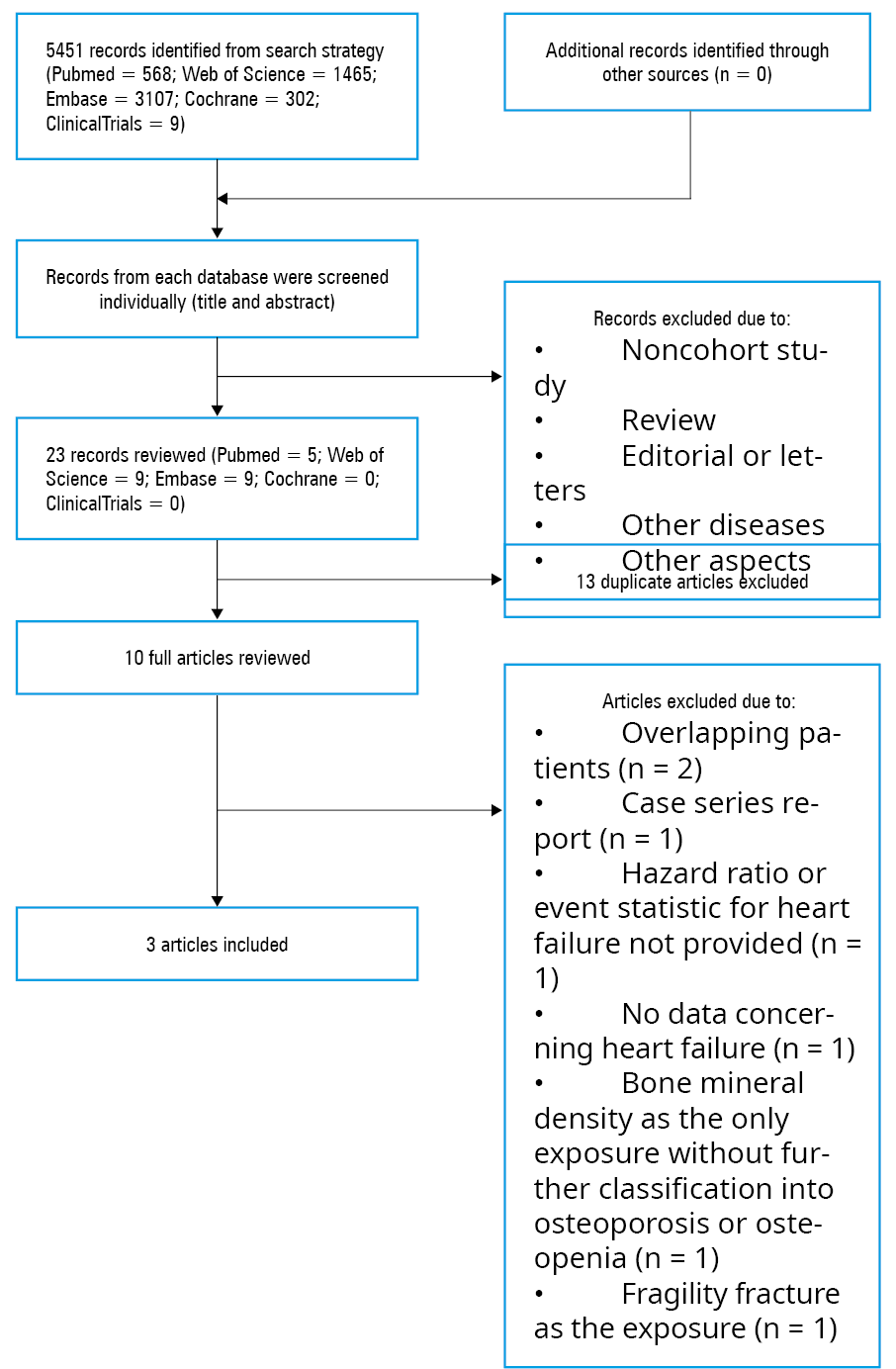
A total of 5451 articles were identified in the search. All articles were derived from the abovementioned databases, and no other sources of studies or unpublished studies were used. Then, 5428 articles were excluded after the screening of their titles and abstracts. Twenty‑three articles (5 in PubMed, 9 in Web of Science, 9 in Embase) were reviewed. Thirteen duplicated articles were excluded. Out of the 10 remaining full‑text studies, 7 were further excluded (mainly because of overlapping cohorts, case series reports, and missing HR data for incident HF) (Supplementary material, table S8), and 3 studies were ultimately included (figure 1).14-16 Among included studies, the cohort study conducted in the United States had a prospective design,14 while the other 2 from Taiwan had a retrospective design.15,16 The main features of the included studies are shown in table 1. All participants were recruited from patients with end‑stage renal disease (ESRD) in the study of Yu et al.16
Study, country | Setting | Participants, n | Race, % | Female sex, % | Follow‑up, y | Age, y, mean (SD) | Adjusted covariates, n | Match | Exposure measure | HF ascertainment |
- Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016; 37: 2129‑2200.
- Rossignol P, Hernandez AF, Solomon SD, Zannad F. Heart failure drug treatment. Lancet. 2019; 393: 1034‑1044. | Crossref
- Balsam P, Ozierański K, Kapłon‑Cieślicka A, et al. Differences in clinical characteristics and 1‑year outcomes of hospitalized patients with heart failure in ESC‑HF Pilot and ESC‑HF‑LT registries. Pol Arch Intern Med. 2019; 129: 106‑116. | Crossref
- Qaseem A, Forciea MA, McLean RM, Denberg TD. Treatment of low bone density or osteoporosis to prevent fractures in men and women: a clinical practice guideline update from the American College of Physicians. Ann Intern Med. 2017; 166: 818‑839. | Crossref
- Veronese N, Stubbs B, Crepaldi G, et al. Relationship between low bone mineral density and fractures with incident cardiovascular disease: a systematic review and meta‑analysis. J Bone Miner Res. 2017; 32: 1126‑1135. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION