Comparison of the 12-month kinetics of the serum markers of fibrosis between treatment with angiotensin receptor–neprilysin inhibitors and angiotensin-converting enzyme inhibitors in patients with heart failure with reduced ejection fraction



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Comparison of the 12-month kinetics of the serum markers of fibrosis between treatment with angiotensin receptor–neprilysin inhibitors and angiotensin-converting enzyme inhibitors in patients with heart failure with reduced ejection fraction
Introduction
Myocardial fibrosis (MF) plays a crucial role in cardiac remodeling during the course of heart failure with reduced ejection fraction (HFrEF).1 The dynamics of MF may be indirectly assessed by measuring the levels of circulating serum markers of fibrosis.2 The clinical use of multilevel neurohormonal blockers (eg, β-adrenergic blockers) and antagonists of the renin–angiotensin–aldosterone system (eg, angiotensin‑converting enzyme inhibitors [ACEIs], angiotensin receptor blockers [ARBs], and mineralocorticoid receptor antagonists) show numerous beneficial effects in HFrEF as well as attenuates MF.3 A recently introduced class of agents—angiotensin receptor–neprilysin inhibitors (ARNIs)—has proven to be superior in patients with HFrEF of various etiologies in comparison to ACEIs and ARBs; however, the role of ARNI treatment in MF remains poorly understood.4-6
In this study, we investigated the kinetics of serum fibrosis markers in ARNI‑treated patients with HFrEF and compared the results with a control group of HFrEF patients treated with ACEIs.
Methods
It was a nonrandomized, prospective, observational, longitudinal open‑label study with a control group. From January 2017 to November 2018, we included 28 patients with HFrEF who started ARNI therapy. Patients treated with ARNIs were compared with an age- and sex‑matched control group consisting of 28 HFrEF patients treated with ACEIs. Both groups were followed up for 12 months and all patients had blood samples collected for biomarker tests at baseline as well as at 3 and 12 months. We analyzed the following serum markers of collagen synthesis: procollagen type I carboxyterminal propeptide and procollagen type III aminoterminal propeptide (PICP and PIIINP; Cloud Clone Corp. Houston, Texas, United States), and fibrosis controlling factors: transforming growth factor β1 (TGF-β1; Diaclone SAS, Besancon Cedex, France) and connective tissue growth factor (CTGF; Cloud Clone Corp., Houston, Texas, United States). The study was approved by an appropriate ethics committee, and patients provided written informed consent to participate in the study.
Statistical analysis
Statistical analyses were performed using the Statistica PL software (Dell Inc., Round Rock, Texas, United States). The significance level was set at 0.05. Normality of variable distribution was assessed with the Shapiro–Wilk test. In both study groups, continuous data were compared using the t test or the Mann–Whitney test, as appropriate, whereas categorical values, with the χ2 test. Blood levels of fibrosis biomarkers were compared at specific and predefined time points, ie, at baseline and at 3 and 12‑month follow‑up. Both groups (ie, ARNI- and ACEI‑treated patients) were matched by propensity score matching according to age and sex. Values were expressed as median (interquartile range [IQR]) or mean (SD) values, whereas nominal variables, as numbers and percentages.
Results
Both study groups were matched with the following crucial variables: age (mean [SD]: ARNI group, 52.9 [15.3] years vs ACEI group, 49.3 [11.6] years; P = 0.23) and male sex (ARNI group, 21 [75%] vs ACEI group, 24 [87%]; P = 0.51). In addition, other clinically relevant parameters were also similarly distributed between the groups: New York Heart Association class (class I: ARNI group, 1 [3.6%] vs ACEI group, 3 [10.7%]; class II: ARNI group, 15 [53.6%] vs ACEI group, 11 [39.3%]; class III: ARNI group, 12 [42.9%] vs ACEI group, 12 [42.9%]; class IV: ARNI group, 0 vs ACEI group, 2 [7.1%]; P = 0.4), ejection fraction (mean [SD]: ARNI group, 24.7% [7.6%] vs ACEI group, 21.8% (8.3%); P = 0.16), and N‑terminal fragment of the prohormone brain natriuretic peptide levels (mean [SD]: ARNI group, 2156.6 (1478) pg/ml vs ACEI group, 2493 (1872) pg/ml; P = 0.6). The detailed baseline characteristics of the ARNI and ACEI groups, respectively, were as follows: mean (SD) body mass index—25.3 (10.8) kg/m2 and 27.1 (5.2) kg/m2 (P = 0.65); hypertension—11 (40.7%) and 14 (50%) (P = 0.49); diabetes—11 (40.7%) and 4 (14.3%) (P = 0.03); dyslipidemia—15 (55.6%) and 10 (35.7%) (P = 0.14); smoking—8 (29.6%) and 15 (53.6%) (P = 0.07); atrial fibrillation—9 (32.1%) and 6 (21.4%) (P = 0.36); QRS width—137.3 (40.4) ms and 109.6 (36.8) ms (P = 0.15); mean (SD) left ventricular end‑diastolic diameter—67.1 (9.1) mm and 71.5 (15.9) mm (P = 0.19); mean (SD) left ventricular end‑diastolic volume—251.7 (106.7) ml and 279.8 (151.7) ml (P = 0.44); the median (IQR) ratio of early mitral inflow velocity (E wave) to early myocardial diastolic velocity (E/E’)—11.5 (10.7–18.5) and 20 (12.3–26.4) (P = 0.01); pulmonary artery systolic pressure—32.5 (15.9) mm Hg and 30.4 (14.2) mm Hg (P = 0.63); mean (SD) hemoglobin level—13.8 (1.8) g/dl and 14.4 (1.6) g/dl (P = 0.17); median (IQR) creatinine level—95.5 (78.2–124.7) μmol/l and 87.5 (69.5–104) μmol/l (P = 0.69); median (IQR) high‑sensitivity C‑reactive protein level—2.6 (0.32–5.3) mg/l and 3.7 (1.1–6.5) mg/l (P = 0.37). The following drugs were used for HF therapy: β-blockers—in 28 patients (100%) in the ARNI group and in 28 patients (100%) in the ACEI group (P = 1); mineralocorticoid receptor antagonists—25 (89.3%) in the ARNI group and 24 (85.7%) in the ACEI group (P = 0.69); loop diuretics—17 (60.7%) in the ARNI group and 19 (69.7%) in the ACEI group (P = 0.58); digoxin—6 (22.2%) in the ARNI group and 5 (17.9%) in the ACEI group (P = 0.69); implantable cardioverter‑defibrillator—11 (39.3%) in the ARNI group and 10 (35.7%) in the ACEI group (P = 0.85); and cardiac resynchronization therapy— 5 (17.9%) in the ARNI group and 4 (14.3%) in the ACEI group (P = 0.85).
The baseline median (IQR) values of serum markers of collagen synthesis were similar for patients treated with ARNIs and ACEIs: PICP—0.09 (0.07–0.32) ng/ml in the ARNI group and 0.15 (0.1–0.25) ng/ml in the ACEI group (P = 0.41); and PIIINP—2537.7 (1873.8–9413.4) pg/ml in the ARNI group and 3043.7 (2923.9–5454.9) pg/ml in the ACEI group (P = 0.58). However, over the follow‑up period, PICP levels were significantly lower in patients treated with ARNIs (at 3 months: 0.09 [0.08–0.21] ng/ml in the ARNI group and 0.23 [0.18–0.28] ng/ml in the ACEI group; at 12 months: 0.1 [0.08–0.22] ng/ml in the ARNI group and 0.34 [0.29–0.36] ng/ml in the ACEI group; all P <0.01) (figure 1A). The levels of PIIINP were similar at 3 months in patients treated with ARNIs and ACEIs (2949.6 [1 359.7–10 437.9] pg/ml vs 4084.2 [3182.9–4642.1] pg/ml; P = 0.89); however, at 12 months, PIIINP levels were significantly higher in patients receiving ARNIs compared with those treated with ACEIs (3471.2 [1 962.9–12 546.1] pg/ml vs 1299.2 [809.8–2875.9] pg/ml; P <0.021) (figure 1B).
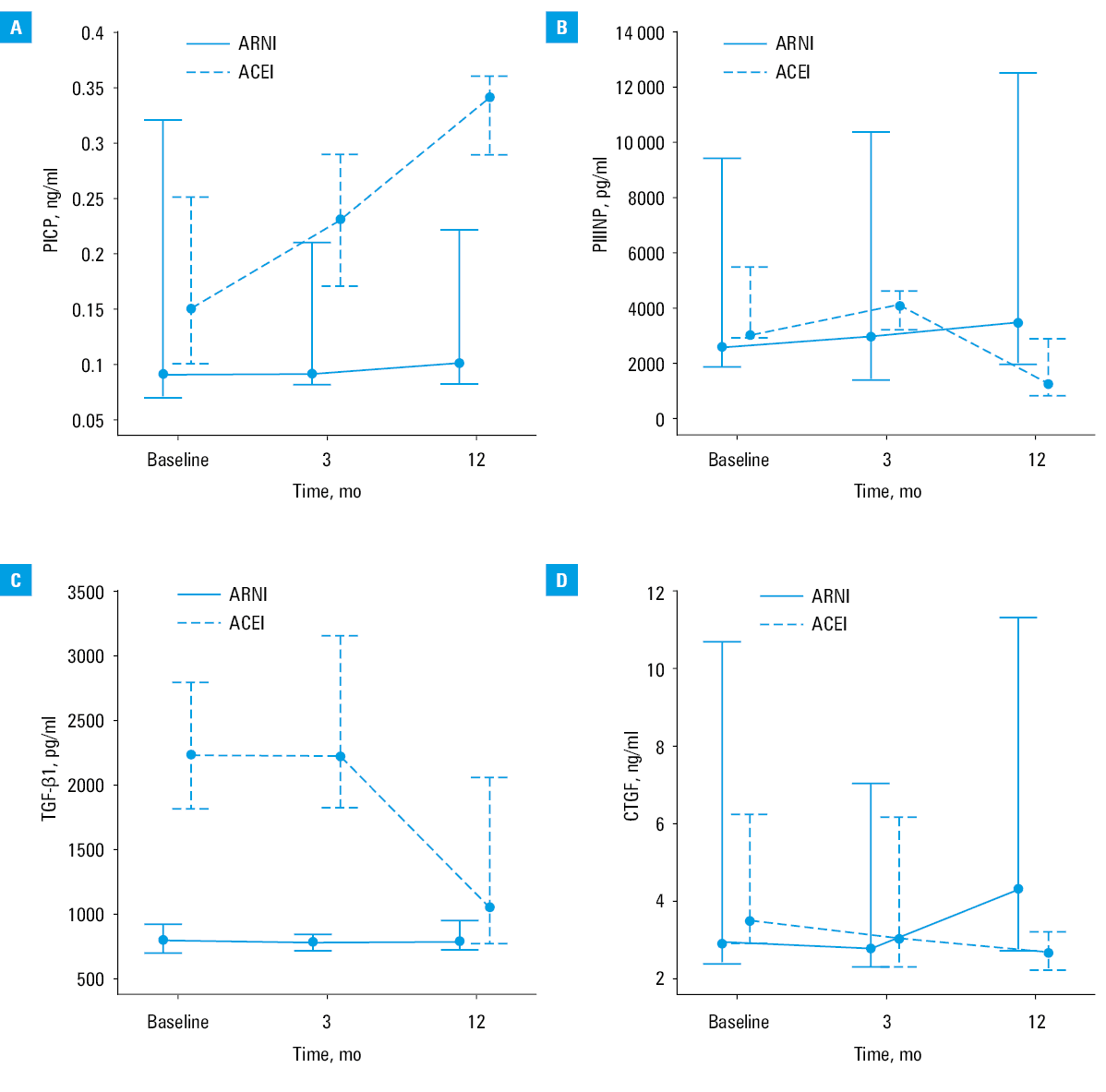
The median (IQR) levels of TGF-β1 were significantly lower in the ARNI group compared with the ACEI group at each time point during the follow‑up period, including at baseline (783.8 [693.5–907] pg/ml in the ARNI group vs 227 [1809–2787] pg/ml in the ACEI group [P <0.001]); at 3 months (769.1 [697–831.8] pg/ml in the ARNI group vs 2226 [1816‑3145] pg/ml in the ACEI group [P <0.001]); and at 12 months (776.5 [722‑934] pg/ml in the ARNI group vs 1031 [763‑2055] pg/ml in the ACEI group [P <0.002]) (figure 1C). The median (IQR) levels of CTGF were similar at baseline (2.9 [2.38–10.7] ng/ml in the ARNI group and 3.4 [2.8–6.2] ng/ml in the ACEI group [P = 0.8]) and at 3 months (2.75 [2.3–6.9] ng/ml in the ARNI group and 3 [2.3–6.1] ng/ml in the ACEI group [P = 0.92]). Interestingly, at 12 months, CTGF was found to be significantly higher in the ARNI group (median [IQR], 4.3 [2.7–11.3] ng/ml) in comparison to the ACEI group (2.6 [2.2–3.2] ng/ml) (P <0.002) (figure 1D).
Discussion
So far, only 3 studies have addressed the issue of ARNI treatment with regard to MF in patients with HF: 2 studies on HFrEF (both being subanalyses of the landmark PARADIGM‑HF (Prospective Comparison of ARNI with ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure) trial, although with populations of slightly different sizes),and a single study on HF with preserved EF (HFpEF).6-8 Similar to our study, these studies investigated MF by means of a variety of circulating markers of fibrosis. In the first subanalysis of the PARADIGM‑HF trial, Zile et al7 observed that, after 8 months of ARNI therapy, the levels of circulating fibrosis‑bound biomarkers, including soluble suppression of tumorigenicity 2 (sST2), matrix metalloproteinases (MMP‑2 and MMP‑9), tissue inhibitor of matrix metalloproteinase, galectin‑3 (Gal‑3), N‑terminal propeptide of collagen I, and PIIINP, decreased to a greater degree in the ARNI group compared with the enalapril group. In a similar analysis, authors from the same group confirmed more pronounced reductions of sST2 levels in ARNI‑treated patients and an association between baseline sST2 levels and outcomes.7 The effect of ARNIs on 4 fibrosis biomarkers: sST2, Gal‑3, MMP‑2, and PIIINP in patients with HFpEF was studied by the PARAMOUNT investigators; however, in contrast to the findings obtained in HFrEF patients, ARNI treatment did not influence the blood levels of the measured biomarkers.8
Thus, this is the first report on the potential effects of ARNI therapy on MF in patients with HFrEF outside of the highly controlled environment of randomized controlled trials. The obvious limitation of our study, which should be acknowledged, is that it was based on a much smaller study population than used in any randomized controlled trial. In addition, the increased risk of false‑positive results when comparing laboratory data at different time points should also be considered. Nonetheless, our study focused on previously unstudied biomarkers of fibrosis (in this context), such as PICP (a potential marker of collagen type I synthesis) as well as TGF-β1 and CTGF. Collagen type I and III is the major component of myocardial fibrous tissue, and its ratio is distorted during MF in HFrEF (ie, there is an excess of collagen type I at the expense of collagen type III). Collagen type I, being stronger and less elastic, leads to a stiffer and less compliant left ventricle, whereas collagen type III is more elastic and compliant.9,10 Therefore, the gradual increase of PICP levels (over the follow‑up period) in patients treated with ACEIs indicated the ongoing overproduction of collagen type I, whereas ARNI‑treated patients had a sustained attenuation of collagen type I production. On the other hand, the production of collagen type III seems to gradually rise in ARNI‑treated patients over a long period of time, whereas it remains at the same level in the ACEI treatment group. In brief, 2 diametrically opposed patterns emerge in terms of collagen type I and III synthesis: one pattern is seen in ARNI‑treated patients, characterized by low collagen type I synthesis and increased synthesis of collagen type III; conversely, in ACEI‑treated patients, an increase in collagen type I synthesis and a decrease in collagen type III production are observed.
Regarding fibrosis controlling factors, it is more challenging to elucidate this issue, as TGF-β1 values were initially significantly higher in the ACEI group and this effect persisted during the follow‑up, ie, TGF-β1 levels were higher at 3 and 12 months. Finally, CTGF levels seemed to rise in the ARNI group over a long period of time, since we noted that CTGF values differed between the study groups only at 12 months. However, the true significance of these TGF-β1 and CTGF patterns in patients receiving ARNIs and ACEIs is far from clear and, as such, it is difficult to interpret these findings at this stage. The initial experience with ARNI therapy in HFrEF is very encouraging and further research is needed to elucidate the mechanisms of its action, such as fibrosis‑attenuating effects.11
Conclusions
In summary, we investigated the potential role of ARNIs in MF in a real‑world setting and observed that treatment with ARNIs may potentially improve the distorted ratio of collagen type I and III synthesis. This, in turn, may translate into favorable changes in the morphology and function of the left ventricle in HFrEF.
- Kong P, Christia P, Frangogiannis N. The pathogenesis of cardiac fibrosis. Cell Mol Life Sci. 2014; 71: 549‑574. | Crossref
- Rubis P, Wiśniowska-Śmiałek S, Wypasek E, et al. 12‑month patterns of serum markers of collagen synthesis, transforming growth factor and connective tissue growth factor are similar in new‑onset and chronic dilated cardiomyopathy in patients both with and without cardiac fibrosis. Cytokine. 2017; 96: 217‑227. | Crossref
- Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2016; 37: 2129‑2200. | Crossref
- Thorvaldsen T, Lund LH. Improving outcomes in heart failure requires improving implementation of heart failure therapy. Pol Arch Intern Med. 2019; 129: 73‑74. | Crossref
- McMurray JJ, Packer M, Desai AS, et al. Angiotensin‑neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014; 371: 993‑1004. | Crossref
ARTICLE INFORMATION