Delayed left subclavian artery pseudoaneurysm following transcatheter aortic valve implantation



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Delayed left subclavian artery pseudoaneurysm following transcatheter aortic valve implantation
In 10% to 15% of patients undergoing transcatheter aortic valve implantation (TAVI), the femoral artery approach is precluded owing to the insufficient caliber or tortuosity of the vessel.1 In that population, the subclavian or axillary access can be used; these have been proven to be equivalent to the femoral artery approach in terms of both survival and vascular complication rates.2 The subclavian or axillary approach usually requires surgical cutdown under general anesthesia or deep sedation, although some cases have been described in which the percutaneous technique was adopted.2-4 Furthermore, the subclavian or axillary access may be burdened by complications such as vessel perforation or rupture and the formation of aneurysms at the site of incision.4,5 In particular, in an interesting study, Ozturk et al5 demonstrated that the diameter of the axillary artery has an impact on the risk of aneurysm yet not on vascular dissection. Furthermore, compared with the transfemoral access, the shorter distance between the delivery sheath and the aortic valve is an advantage allowing operators to better position and control the device.2,5
Here, we report the case of a 79‑year‑old woman who was admitted to our hospital owing to worsening dyspnea and severe aortic stenosis (mean transvalvular gradient, 53 mm Hg). As the patient was frail and suffered from various comorbidities, the Heart Team decided to perform TAVI.
Preoperative computed tomography (CT) showed noncritical lesions of both the medial anterior interventricular artery and the medial circumflex artery. Moreover, the abdominal aorta and the subclavian arteries appeared to be atheromatous, and severe peripheral arteriopathy was noted. The left subclavian artery was therefore chosen. Access was obtained through a 4‑cm incision in the deltopectoral groove, under general anesthesia. Care was taken to avoid damaging the brachial plexus, and a 5‑0 polypropylene purse‑string suture was then fixed to the anterior wall of the artery.
A 26‑mm Medtronic CoreValve Evolut R was implanted. The purse‑string suture was tied under direct visualization, without complications. After valve implantation, the subclavian, radial, and ulnar pulses were detectable. The patient was discharged in good cardiovascular condition.
A week later, however, the patient started complaining of left arm dysesthesia, weakness, and pain. Cerebral CT and the vascular ultrasound scan of the subclavian artery at the site of incision were unremarkable, but the neurological evaluation was indicative of brachial plexus compression.
Subsequently, CT angiography demonstrated a 2.5 × 2.8 cm left subclavian pseudoaneurysm, proximal to the site of incision, which compressed the cervical spine (Figure 1A).
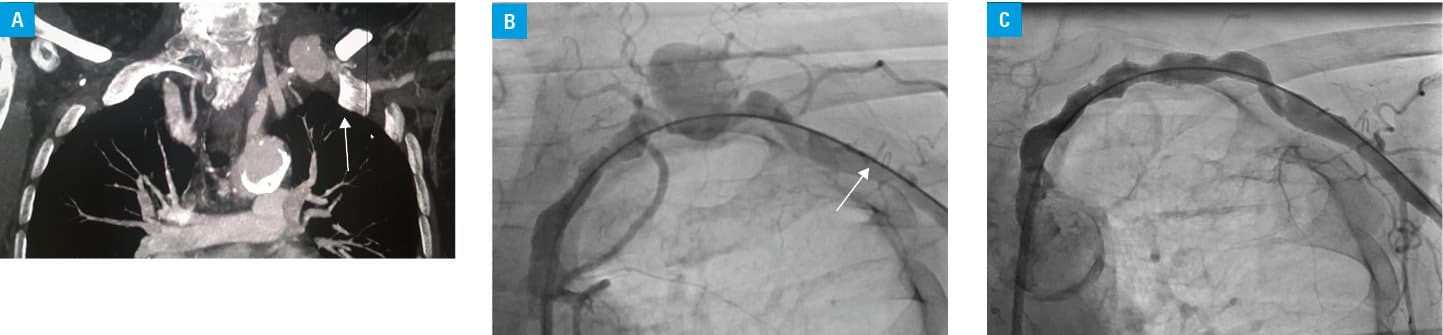
The vascular lesion was treated with the implantation of an 8 × 5‑mm Gore Viabahn covered stent, which yielded a good final angiographic result (Figure 1B and 1C). The patient was discharged with the residual functional limitation of the left arm, which improved over the following weeks. However, she fully regained the neurological function of the arm after 6 months.
To our knowledge, this is a very rare case of subclavian pseudoaneurysm caused by the TAVI procedure. While vascular suclavian access complications are usually acute,2 in this patient, the pseudoaneurysm developed later. Notably, it occurred proximally to the site of incision, in a challenging spot for ultrasound detection.
It may be hypothesized that the insertion of the delivery sheath into the vessel may have dislodged a pre‑existing atherosclerotic plaque, thereby causing a pseudoaneurysmatic lesion. Neurological consequences were not immediate and might have been due to the compression of the brachial plexus.
Of note, when the subclavian TAVI approach is adopted and the patient manifests neurological symptoms possibly related to nerve compression, a careful multimodal evaluation of the entire vessel should be performed in order to rule out any possible vascular complications, even if the site of incision is not strictly involved.
- Pascual I, Carro A, Avanzas P, et al. Vascular approaches for transcatheter aortic valve implantation. J Thorac Dis. 2017; 9: S478‑S487. | Crossref
- Caceres M, Braud R, Roselli EE. The axillary/subclavian artery access route for transcatheter aortic valve replacement: a systematic review of the literature. Ann Thorac Surg. 2012; 93: 1013‑1018. | Crossref
- Petronio AS, De Carlo M, Bedogni F, et al. Safety and efficacy of the subclavian approach for transcatheter aortic valve implantation with the CoreValve revalving system. Circ Cardiovasc Interv. 2010; 3: 359‑366. | Crossref
- Vavuranakis M, Vrachatis DA, Filis K, Stefanadis C. Transcatheter aortic‑valve implantation by the subclavian approach complicated with vessel dissection and transient left‑arm paralysis. Eur J Cardiothorac Surg. 2011; 39: 127‑129. | Crossref
- Ozturk C, Iyisoy A, Sahin MA, et al. Left subclavian artery dissection and repair after transcatheter aortic valve implantation. Int J Cardiol. 2016; 204: 77‑80. | Crossref
ARTICLE INFORMATION