Worse long-term prognosis in myocardial infarction occurring at weekends or public holidays with insight into myocardial infarction with nonobstructive coronary arteries
Key words: myocardial infarction, myocardial infarction with nonobstructive coronary arteries, prognosis, weekend



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Worse long-term prognosis in myocardial infarction occurring at weekends or public holidays with insight into myocardial infarction with nonobstructive coronary arteries
Introduction: The weekend effect in Polish patients with myocardial infarction (MI) treated in the current network of catheterization laboratories is poorly understood.
Objectives: We sought to investigate long‑term prognosis of patients with MI admitted at weekends or public holidays (NWDs) and on working days (WDs).
Patients and methods: We enrolled 865 patients with MI hospitalized between 2012 and 2017. The long‑term mortality within the median (IQR) time of 68.5 (36.7–78.4) months was determined in 223 patients (25.8%) admitted on NWDs and in 642 (74.2%) on WDs.
Results: Patients admitted on NWDs more often had ST‑segment elevation MI (41.3% vs 30.8%; P = 0.005), left anterior descending artery as an infarct‑related artery (38.1% vs 30.2%; P = 0.031) and incomplete reperfusion expressed as Thrombolysis in Myocardial Infarction flow grade 0/1 following primary angioplasty (6.8% vs 1.6%; P <0.001) as compared with those hospitalized on WDs. Myocardial infarction with nonobstructive coronary arteries (MINOCA) occurred less often on NWDs (4% vs 9%, P = 0.019). The all‑cause long‑term mortality was higher in NWD patients as compared with those admitted on WDs (36.3% vs 28.4%; P = 0.037). By the Cox proportional hazards model with time‑dependent covariates, MI on NWDs (hazard ratio, 1.027; 95% CI, 1.022–1.032; P <0.001) but not MINOCA (hazard ratio, 0.971; 95% CI, 0.595–1.583; P = 0.91) was independently associated with long‑term mortality.
Conclusions: Patients hospitalized on NWDs as compared with those admitted on WDs had a larger ischemic territory and more often had transmural MI with incomplete epicardial reperfusion, which resulted in a higher long‑term mortality. The latter outcome was not influenced by MINOCA.
What's new?
The weekend effect means worse prognosis in patients admitted to hospitals during weekends. Its impact on myocardial infarction has been intensively studied over the recent years. Several hypotheses concerning this phenomenon have been proposed so far, but its etiology has not been fully elucidated. In the current study with over 5‑year follow‑up, it was shown that patients with myocardial infarction admitted at weekends or public holidays had higher long‑term mortality than those hospitalized during working days and this effect was visible after the first year of observation. Patients admitted during nonworking days compared with those admitted during working days had more often ST‑segment elevation myocardial infarction accompanied by more frequent myocardial infarctions with larger ischemic territory and incomplete epicardial blood flow not driven by operator experience. Simultaneously, myocardial infarction with nonobstructive coronary arteries was less often diagnosed on nonworking days, but this finding did not influence long‑term mortality.
Introduction
The weekend effect and its impact on the outcomes of myocardial infarction (MI) treatment has been intensively studied over the recent years. The first comprehensive report regarding the weekend effect was presented in 2001 by Bell and Redelmeier.1 Based on their analyses of 3 789 917 broadly defined acute care admissions, they stated a significantly higher in‑hospital mortality in various disease entities.1 Previous findings have been summarized in 2 meta‑analyses. Sorita et al2 ascertained a higher in‑hospital (odds ratio [OR], 1.05; 95% CI, 1.03–1.08) and 30‑day mortality (OR, 1.05; 95% CI, 1.02–1.09) in patients admitted off‑hours. According to their observations, these differences might have eventuated out of the substantially longer door‑to‑balloon time in ST‑segment elevation MI (STEMI). Kwok et al3 have recently confirmed that with observations regarding a slightly higher early mortality in weekend admissions (OR, 1.06; 95% CI, 1.03–1.09). The hypothesis regarding the impact of the timing of admission on clinical outcomes has not been confirmed based on more recent studies.3
There is scarce evidence regarding the weekend effect in Polish patients. Słonka et al4 demonstrated similar rates of in‑hospital complications as well as 2‑year mortality in patients treated with percutaneous coronary intervention (PCI) in the daytime and during off‑shift hours in the years 1998 to 2003. Noteworthy, the significantly higher rate of stent implantations was observed in the daytime group.4 A similar analysis of patients with STEMI collected in the EUROTRANSFER registry showed that thrombolytic therapy was more frequently administered to patients hospitalized off‑hours (4.1% vs 2.3%; P = 0.041). Surprisingly, the time from chest pain onset to diagnosis of STEMI was shorter in the off‑hours group by 10 minutes (P = 0.007); nevertheless, 1‑year mortality rates were similar in both groups.5 Despite the above‑mentioned observations, there are no available data solely describing the relationship between the current organization of cardiac catheterization laboratories in Poland working for 24 hours, 7 days a week and the long‑term prognosis in patients with MI admitted on nonworking days. This problem has been partly raised by Walicka et al.6 In their recently published study, the authors determined the predictors of in‑hospital mortality based on the large number of 2 855 029 nonsurgical hospitalizations.6 As was shown, vascular diseases were characterized by the highest mortality, whereas weekend admissions (Saturday: OR, 1.40; 95% CI, 1.36–1.43; Sunday: OR, 1.29; 95% CI, 1.26–1.32) and public holidays (OR, 1.25; 95% CI; 1.20–1.30) were independent predictors of in‑hospital mortality.
In this study we sought to investigate whether the occurrence of MI at weekends or public holidays influences the long‑term prognosis in Polish patients treated in a high‑volume university center and to determine the potential causes of these relationships.
Patients and methods
We enrolled 865 consecutive patients hospitalized between 2012 and 2017 in our hospital with a MI diagnosis and in whom coronary angiography was performed. A total of 223 (25.8%) were admitted on a nonworking day (NWD) including weekends (Saturdays or Sundays) (200 [23.1%]) or public holidays (23 [2.7%]). In turn, 642 (74.2%) patients were admitted on a working day (WD) (figure 1). Patient age, anthropometric data, medical history, clinical presentation, baseline laboratory measurements, and data regarding the course of hospitalization were collected.7 Patients were classified as STEMI or NSTEMI in accordance with current guidelines.8,9 Renal failure was diagnosed when the creatinine clearance calculated by means of the Cockcroft–Gault formula was lower than 60 ml/min.10 Between 2 and 4 days after admission, left ventricular ejection fraction (LVEF) was assessed by 2‑dimensional transthoracic echocardiography at rest.11
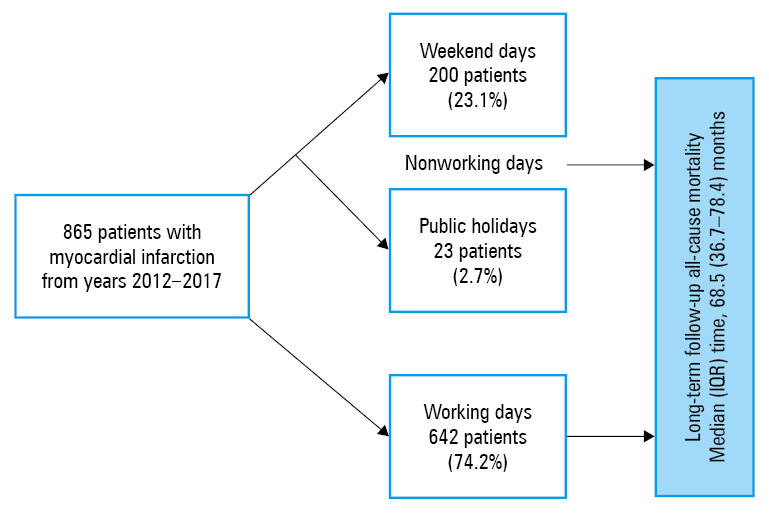
Abbreviations: IQR, interquartile range
A detailed evaluation of both the infarct‑related artery (IRA) as well as the result of the primary PCI procedure were performed based on angiography done for each artery in 2 contralateral projections.12 Two experienced and blinded physicians reviewed each coronary angiogram. In case of disagreement between the 2 physicians, a third opinion was sought, and a conclusion was drawn.13,14 Myocardial infarction with nonobstructive coronary arteries (MINOCA) has been defined by the universal criteria of MI and no lesion of 50% or greater on coronary angiography.15 Moreover, patients with MINOCA were analyzed for the presence of insignificant stenosis in epicardial arteries and were divided into 2 groups with 1) normal coronary arteries or minimal intracoronary irregularities with stenosis of less than 30% or with 2) mild to moderate lesions of at least 30% and less than 50%.16 Epicardial blood flow was evaluated by means of the Thrombolysis In Myocardial Infarction (TIMI) scale in all patients.17 TIMI epicardial blood flow grade 2 or 3 without flow limiting dissection not covered by the stent was recognized as the optimal PCI result, whereas TIMI flow grade 0 or 1 was the equivalent of incomplete epicardial reperfusion.17-19 According to the commonly accepted American College of Cardiology Foundation / American Heart Association / American College of Physicians clinical competence statement, operators performing less than 50 PCIs per year, 50 to 100 PCIs per year, or more than 100 PCIs per year were defined as low, intermediate-, or high‑volume, respectively.20,21
Long‑term follow‑up of all‑cause mortality was obtained from the Polish National Death Registry. The study protocol was complied with the Declaration of Helsinki and was approved by the local ethics committee. All patients included in the study gave their informed consent.
Statistical analysis
Statistical analyses were performed with the SPSS Statistics software (version 25.0.0.2, IBM, Armonk, New York, United States). Continuous variables were first checked for normal distribution and expressed as median (interquartile range) or mean (SD), whereas categorical variables as number (percentage). Continuous variables were compared by the t test or the Mann–Whitney test if the distribution was normal or different than normal, respectively. Categorical variables were analyzed by means of the χ2 test or the Fisher exact test. Kaplan‑Meier curves of all‑cause mortality in the study groups were performed and compared with the log‑rank test. Finally, the proportional hazard assumption was verified with the model interaction of the covariate of interest with time. If such a variable turned out to be significant, the proportional hazard assumption would be violated.22 Afterwards, the Cox proportional hazards model with time‑dependent covariates was performed to find the independent determinants of all‑cause mortality. A 2‑tailed P value of less than 0.05 was considered statistically significant.
Results
Clinical characteristics
The baseline characteristics of the enrolled patients are shown in table 1. Patients in NWD and WD groups were similar in terms of demographic data, cardiovascular risk factors, history of MI, stroke, prior percutaneous and / or surgical coronary revascularization, and the distribution of Killip class on admission. The significant differences were observed in the clinical presentation of MI. STEMI was more frequent on NWDs (41.3% vs 30.8%; P = 0.005) accompanied by higher values of baseline creatine kinase (median [IQR], 202 [112–527] IU/l vs 169 [105–335] IU/l; P = 0.02) and isoenzyme MB of creatine kinase (median [IQR], 24 [16–61] vs 21 [14–39] IU/l, P = 0.003) as compared with those admitted on WDs. There were no differences in the remaining laboratory parameters on admission (table 1).
Characteristic | Nonworking days (n = 223) | Working days (n = 642) | P value | |
- Bell CM, Redelmeier DA. Mortality among patients admitted to hospitals on weekends as compared with weekdays. N Engl J Med. 2001; 345: 663‑668. | Crossref
- Sorita A, Ahmed A, Starr SR, et al. Off‑hour presentation and outcomes in patients with acute myocardial infarction: systematic review and meta‑analysis. BMJ. 2014; 348: f7393. | Crossref
- Kwok CS, Al‑Dokheal M, Aldaham S, et al. Weekend effect in acute coronary syndrome: a meta‑analysis of observational studies. Eur Heart J Acute Cardiovasc Care. 2019; 8: 432‑442. | Crossref
- Słonka G, Gąsior M, Lekston A, et al. Comparison of results of percutaneous coronary interventions in patients with ST‑segment elevation myocardial infarction during routine working hours or off‑hours. Kardiol Pol. 2007; 65:1171‑1180.
- Siudak Z, Rakowski T, Dziewierz A, et al. Primary percutaneous coronary intervention during on- vs off‑hours in patients with ST‑elevation myocardial infarction. Results from EUROTRANSFER Registry. Kardiol Pol. 2011; 69: 1017‑1022.
ARTICLE INFORMATION