Exacerbation of Crohn disease mimicking menstrual cramping: the diagnostic value of contrast-enhanced ultrasound in assessing acute inflammatory lesions



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Exacerbation of Crohn disease mimicking menstrual cramping: the diagnostic value of contrast-enhanced ultrasound in assessing acute inflammatory lesions
Inflammatory bowel disease has become a global problem with the highest prevalence (often exceeding 0.3%) in Europe and North America.1 Current international guidelines and recommendations (European Crohn’s and Colitis Organization, European Society of Gastrointestinal and Abdominal Radiology, American College of Gastroenterology) emphasize the role of diagnostic imaging both in initial and periodic evaluation of patients with Crohn disease (CD). Magnetic resonance enterography (MRE) and computed tomography enterography exhibit similar diagnostic characteristics, with MRE being preferred due to absence of radiation. We aimed to prove an equally high diagnostic value of contrast‑enhanced ultrasound (CEUS) in imaging of patients with CD.2-4
A 43‑year‑old woman presented to the emergency room due to an exacerbation of persistent bile‑stained vomiting (8 episodes on the day of admission) and acute abdominal pain within the right lumbar and iliac regions. No symptom alleviation was observed after the intravenous administration of antispasmodic agents (drotaverine hydrochloride) and nonsteroidal anti‑inflammatory drugs (metamizole). She was in the first phase (period) of the menstrual cycle. The patient was diagnosed with CD 12 years before, had a history of multiple perianal fistulae removal, and appendectomy at the age of 15. She had recently finished biologic treatment (infliximab), and at the time of admission was treated with azathioprine and mesalazine.
The physical examination showed blood pressure of 95/78 mm Hg, pain on palpation limited to previously mentioned abdominal regions with moderate bloating, no muscle guarding or peritoneal symptoms. Digital rectal examination was unremarkable except for scarring related to healed perianal fistulae. Abdominal X‑ray showed single intestinal air‑fluid level in the mid abdomen. Laboratory testing indicated an elevated C‑reactive protein level of 61.3 mg/l (reference range, 0–5 mg/l), which was comparable with the levels during the recent biologic treatment, without leukocytosis (white blood cell count 7.65 × 103/µl; reference range, 4–10 × 103/µl). The consulting surgeon assessed the clinical findings as related to menstruation.
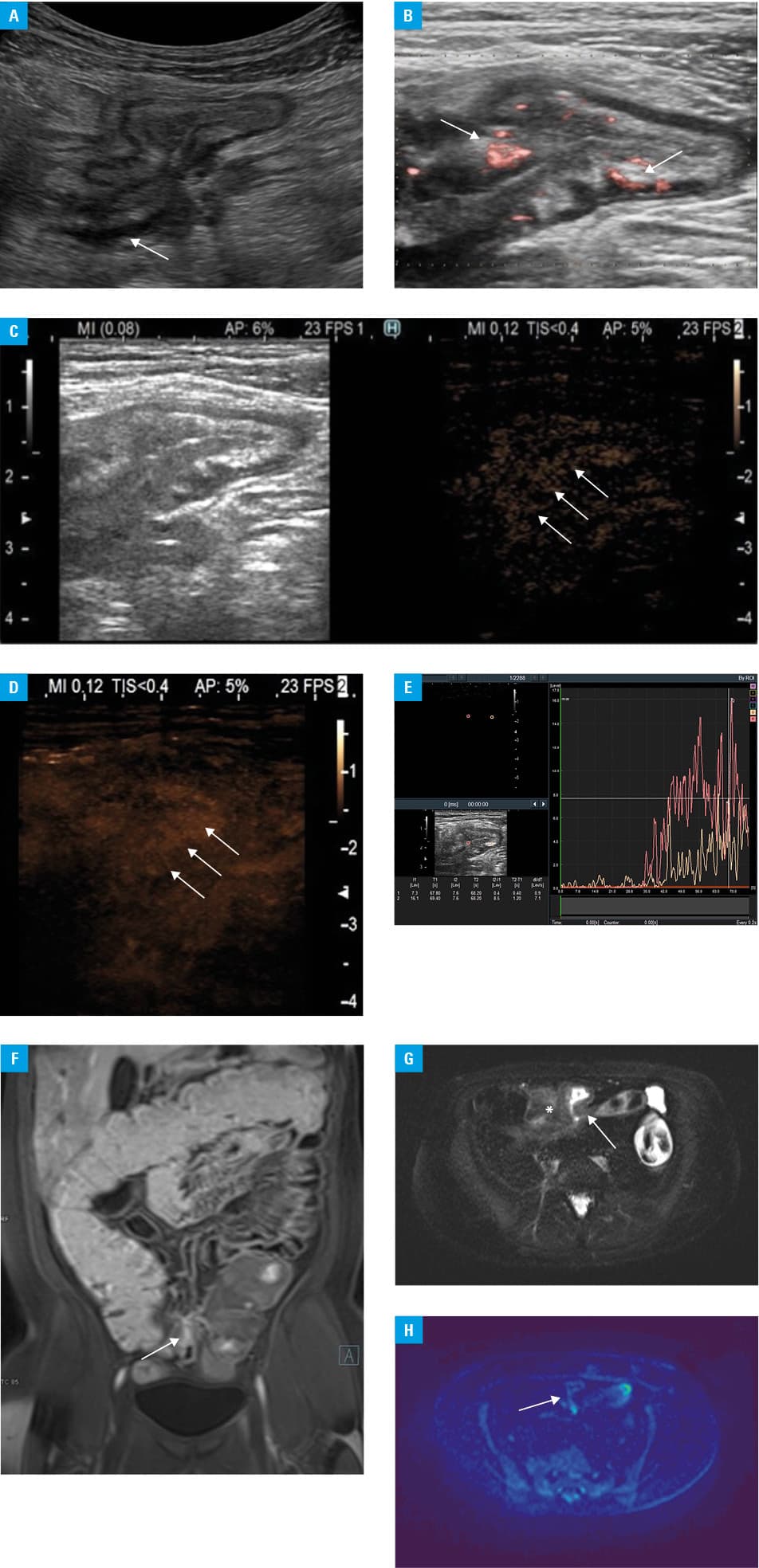
However, given the previous medical history and poor clinical condition, the patient was transferred to the gastroenterology department where abdominal ultrasound was performed. It indicated mild jejunal distension, bowel wall thickening with preserved mural stratification, and hyperemia within both the terminal ileum and the angulated ileal loop in the lower abdominal region. Increased echogenicity of the surrounding mesenteric fat and peri‑intestinal trace of fluid within the hypogastrium were reported as well. There was no apparent lymphadenopathy. It was decided to include CEUS and MRE in the diagnostic imaging protocol. CEUS was performed using the Hitachi Aloka Arietta 850 ultrasound setup with the L441 2–12 MHz linear transducer. It confirmed prior ultrasound findings; additionally it revealed an asterisk shaped configuration of both previously reported ileal loop localized within the hypogastrium and the adjacent large intestine, raising the suspicion of fistula with surrounding inflammation (figure 1A and 1B). Following the initial anatomic assessment, the patient received contrast medium injection (SonoVue, Bracco, Milan); the examination demonstrated marked enhancement of the abnormal, tethered ileal loop’s wall, particularly within the mucosal and submucosal layers, suggestive of active inflammation (figure 1C-1E). All outcomes were further confirmed with a reference modality, that is, MRE (figure 1F-1H).
The patient received optimal medical treatment, including intravenous corticosteroids, mesalazine, azathioprine, and metronidazole, due to her CD activity index score of 459.82 indicating an acute exacerbation of CD. Based on imaging findings, she was qualified for an elective surgery of a complex ileosigmoid fistula.
The presented case proves that CEUS might be an effective and reliable diagnostic modality to evaluate the activity and severity of CD.
- Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population‑based studies. Lancet. 2018; 390: 2769‑2778. | Crossref
- Maaser C, Sturm A, Vavricka SR, et al. ECCO‑ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J Crohns Colitis. 2019; 13: 144‑164. | Crossref
- Lichtenstein GR, Loftus EV, Isaacs KL, et al. ACG clinical guideline: management of crohn’s disease in adults. Am J Gastroenterol. 2018; 113: 481‑517. | Crossref
- Caraiani C, Yi D, Petresc B, Dietrich C. Indications for abdominal imaging: when and what to choose? J Ultrason. 2020; 20: e43‑e54. | Crossref
ARTICLE INFORMATION