Atrial fibrillation is more frequently associated with nonobstructive coronary lesions: the Bialystok Coronary Project
Key words: by Kozieł, see p. 1024



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Atrial fibrillation is more frequently associated with nonobstructive coronary lesions: the Bialystok Coronary Project
Introduction: Atrial fibrillation (AF) and chronic coronary syndrome (CCS) share common risk factors and frequently coexist. Additionally, AF symptoms may mimic CCS.
Objectives: The aim of the study was to investigate the hypothesis indicating absence of significant coronary lesions in patients with AF as compared with those with sinus rhythm.
Patients and methods: We conducted a single‑center retrospective study including consecutive patients referred for elective coronary angiography between 2007 and 2016.
Results: The study population included 8288 patients out of whom 1674 had AF. There were substantial differences between groups with and without AF. Patients with AF were significantly older, more often were men and had diabetes, and more frequently were diagnosed with both chronic kidney disease and heart failure. On the other hand, they had history of hyperlipidemia less often. CCS was less frequently detected in patients with AF as compared with those with sinus rhythm (37.5% vs 41.1%; P <0.001). Additionally, the latter group more often underwent subsequent coronary angioplasty (19.2% vs 22.3%; P = 0.004). Multivariable analysis identified AF as an independent factor associated with absence of significant coronary lesions (odds ratio, 1.57; 95% CI, 1.32–1.87; P <0.001). Moreover, a comparison between patients with and without angiographically significant CCS revealed a higher prevalence of AF in the latter group (18.7% vs 21.2%; P = 0.006).
Conclusions: In our study, AF was associated with the absence of significant coronary lesions on angiography, reflecting difficulties with qualifying patients with AF for invasive CCS diagnostic workup. Our findings suggest the need for more efficacious noninvasive diagnostic approach for patients with AF and suspected CCS.
What's new?
In this study, the number of nonsignificant findings on coronary angiography was 1.6‑fold higher in patients with atrial fibrillation (AF) than in patients without AF. Atrial fibrillation was associated with absence of significant coronary lesions and patients with AF less frequently underwent coronary angioplasty as compared with those with sinus rhythm. This raises the possibility that it may be difficult to select patients with AF for invasive procedures, given the increased findings of nonsignificant chronic coronary syndromes (CCS) on coronary angiography. The reason for these findings might be multifactorial: AF symptoms mimic CCS symptoms, ST‑segment depression during AF poorly predicts obstructive CCS, stress tests are rarely proceeded in patients with AF, and rapid rhythm makes computed tomography scan difficult to interpret. A more efficacious noninvasive diagnostic approach is needed in patients with AF and suspected CCS.
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia associated with excessive risk of ischemic stroke and heart failure as well as reduced life expectancy.1,2 On the other hand, chronic coronary syndrome (CCS) remains the main cause of morbidity and mortality in an aging population. Both disease entities share common risk factors such as hypertension, diabetes, and obesity.3-5
The prevalence of CCS in patients with AF varies from 17% to 47%,3,6,7 whereas AF in patients with CCS is much less common, ranging from 0.2% to 5%.8-12 Patients with AF more often have concomitant CCS as compared with sinus rhythm controls.13,14 Additionally, AF is more frequently present in patients with either peripheral or cerebrovascular artery disease than in nonatherosclerotic individuals.15
Patients with AF in the course of arrhythmia may present with chest pain, which can be accompanied by transient ischemic‑type ST‑segment changes, sometimes with marginally elevated cardiac necrosis markers, thus mimicking symptoms of CCS.16 There are contradictory data on angiographic findings among patients with AF.14 It is important to look at the prevalence of significant CCS lesions in patients with AF compared with those with sinus rhythm to prevent unnecessary coronary angiography in patients with AF.
On the other hand, there are several studies including the ARIC (the Atherosclerosis Risk in Communities) study, the MESA (Multi‑Ethnic Study of Atherosclerosis), and the Rotterdam Study which found an association between subclinical atherosclerosis and incident AF.17
The aim of the present study was to investigate the hypothesis indicating the absence of significant coronary lesions in patients with AF as compared with those with sinus rhythm referred for elective coronary angiography. This indicates that some patients with AF may have undergone coronary angiography needlessly.
Patients and methods
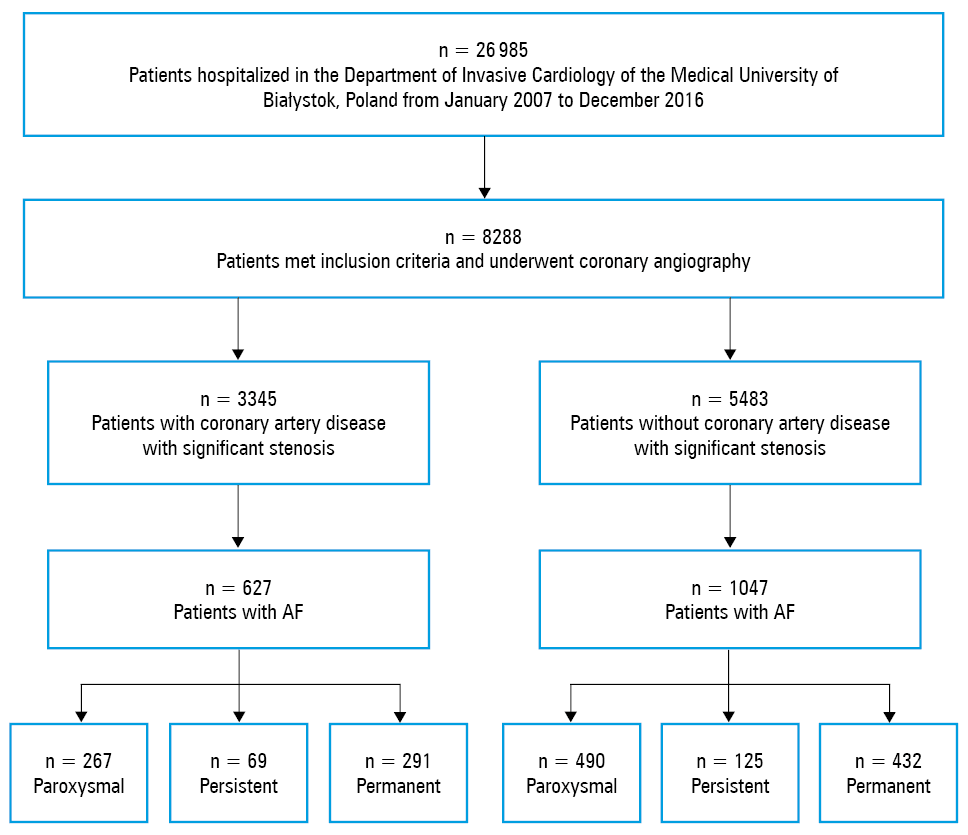
We reviewed medical records of 26 985 patients hospitalized in the Department of Invasive Cardiology of the Medical University of Bialystok, Poland, who had coronary angiography performed because of exacerbated angina (recurrent chest pain, classical stable angina, long history of chest pain / angina, or other symptoms such as dyspnea) between 2007 and 2016. The Bialystok Coronary Project is an observational research project that includes hospitalized patients with AF and CCS. It is focused on diagnostics and therapy of this population. We excluded patients with acute coronary syndromes (ACS), Takotsubo cardiomyopathy, and history of ischemic heart disease, as well as those referred for coronary angiography before heart valve surgery. Prior cardiosurgical valve replacement was also the exclusion criterion. The set of extracted variables included demographic data, medical history, physical examination, resting electrocardiogram, routine transthoracic echocardiogram, coronary angiogram, and percutaneous coronary intervention (PCI). Eventually, our final study cohort included 8288 patients. Concomitant diseases were defined via the International Statistical Classification of Diseases, Tenth Revision (ICD‑10) codes, not prescription claims.
We analyzed whether history of AF was associated with the absence of significant coronary lesions on coronary angiography. We also investigated factors connected with the absence of significant coronary lesions on angiography. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki, and was approved by the local ethics committee.
Coronary angiography
All patients underwent coronary angiography and the number of diseased vessels were assessed. Coronary angiography was performed according to the Judkins technique.18 Diagnosis of CCS and indication for PCI was performed according to the current European guidelines.19 Significant stenosis of the coronary vessel was defined as more than 50% in the main stem of the left coronary artery and 70% in the rest of the epicardial arteries. The degree of CCS was classified as single-, double-, or triple‑vessel disease.
Echocardiographic analysis
Left ventricular ejection fraction (LVEF) was assessed in transthoracic echocardiography using the modified biplane Simpson method (Philips Ultrasound System, Sonos 5500, Aalborg, Denmark, equipped for harmonic imaging with a 3.6 MHz transducer) and was derived in accordance with the recommendations of the European Society of Echocardiography.20
Definition of atrial fibrillation
Atrial fibrillation was defined as the presence of AF on electrocardiogram during the index hospitalization and / or as indicated by a diagnosis found in medical records, the hospital inpatient database, or outpatient databases. Electrocardiographic AF was defined as an irregular rhythm with fibrillatory waves and no defined P waves. Diagnoses and AF classification were based on physician‑assigned diagnoses in the medical records and / or the presence of corresponding codes from the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD‑9‑CM) for AF (427.31) in the hospital discharge or outpatient databases. Atrial fibrillation was further divided into the following categories: paroxysmal AF or chronic AF (persistent and permanent).1
Statistical analysis
Continuous data were expressed as means (SD) or medians and interquartile ranges (IQRs) when appropriate. Relative frequencies were used to present categorical variables. Normality of the distribution was assessed with the Kolmogorov–Smirnov test, while the 2‑tailed t test was applied for the comparative analysis of variables. Nonnormally distributed data were compared with the Mann–Whitney test. Categorical variables were compared using the χ2 test. The multivariable logistic regression backward stepwise Wald method was used to determine the odds ratio (OR) for the absence of significant coronary lesions. A 2‑tailed P value of less than 0.05 was considered statistically significant. The IBM SPSS version 25.0 software package (SPSS, Chicago, Illinois, United States) was used.
Results
Out of 26 985 patients admitted for elective coronary angiography, a total of 8288 patients were included in the final analysis (Figure 1, Table 1). Over 80% of study participants had hypertension, 66.9% had hyperlipidemia, and 25.7% had diabetes. Chronic kidney disease (CKD) and chronic heart failure (CHF) were diagnosed in 32.5% and 20.6% of the study population, respectively. Detailed characteristics of the study population is provided in Table 2.
Abbreviations: AF, atrial fibrillation
Patients | Value |
Data are presented as number (percentage) of patients.
Abbreviations: NSTEMI, non–ST‑segment elevation myocardial infarction; STEMI, ST‑segment elevation myocardial infarction; UA, unstable angina | |
All | 26 985 (100) |
Included in the final analysis | 8288 (30.7) |
Admitted for coronary angiography before heart valve surgery | 3499 (13) |
Hospitalized due to NSTEMI | 3126 (11.6) |
Hospitalized due to STEMI | 3102 (11.5) |
With history of ischemic heart disease | 2940 (10.9) |
Hospitalized due to UA | 2503 (9.3) |
Admitted for scheduled percutaneous coronary intervention | 2211 (8.2) |
Other | 1316 (4.9) |
Variable | All study participants (n = 8288) | Patients with AF (n = 1674) | Patients without AF (n = 6614) | P value |
Data are presented as number (percentage) of patients unless otherwise indicated. The percentage is calculated within the subgroup.
Abbreviations: BMI, body mass index; CAD, coronary artery disease; CCS, Canadian Cardiovascular Society Angina Grading Scale; Cx, circumflex artery; DIAG, diagonal artery; eGFR, estimated glomerular filtration rate; HFmrEF, heart failure with moderate ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; IQR, interquartile range; LAD, left anterior descending; LM, left main artery; NYHA, New York Heart Association Functional Classification; OM, left marginal artery; PCI, percutaneous coronary intervention; RBC, red blood cells; RCA, right coronary artery; others, see Figure 1 | ||||
Male sex, n (%) | 4500 (54) | 1018 (61) | 3482 (53) | <0.001 |
Age, y, mean (SD) | 65.2 (10.2) | 68.6 (9.6) | 64.3 (10.2) | <0.001 |
BMI, kg/m2, mean (SD) | 29.1 (4.9) | 30 (5.2) | 28.9 (4.7) | <0.001 |
NYHA class, median (IQR) | 2 (2–3) | 3 (2–3) | 2 (2–3) | 0.22 |
CCS class, median (IQR) | 2 (2–2) | 2 (2–2) | 2 (2–2) | 0.26 |
CAD with significant stenosis on coronary angiography | 3345(40.4) | 627 (37.5) | 2718 (41.1) | <0.001 |
Single‑vessel CAD | 1507 (18.2) | 342 (20.4) | 1165 (17.6) | <0.001 |
Double‑vessel CAD | 807 (9.7) | 126 (7.5) | 681 (10.3) | <0.001 |
Triple‑vessel and / or significant LM stenosis | 1031 (12.4) | 159 (9.5) | 872 (13.2) | <0.001 |
Hyperlipidemia | 5548 (66.9) | 961 (57.4) | 4587 (69.4) | <0.001 |
Hypertension | 6886 (83.1) | 1370 (81.8) | 5516 (83.4) | 0.14 |
Diabetes mellitus | 2132 (25.7) | 477 (28.5) | 1655 (25) | 0.005 |
Chronic heart failure | 2690 (32.5) | 1038 (62) | 1652 (24.9) | <0.001 |
HFrEF | 1381 (51.3) | 621 (59.8) | 760 (46) | <0.001 |
HFmrEF | 599 (22.3) | 220 (21.2) | 379 (22.9) | |
HFpEF | 710 (26.4) | 197 (18.9) | 513 (31.1) | |
Left ventricular ejection fraction, %, median (IQR) | 55 (42–60) | 45 (30–55) | 56 (50–60) | <0.001 |
Chronic kidney disease | 1706 (20.6) | 556 (33.2) | 1150 (17.4) | <0.001 |
Creatinine, mg/dl, median (IQR) | 0.89 (0.78–1.05) | 0.97 (0.82–1.17) | 0.87 (0.78–1.02) | <0.001 |
eGFR, ml/min/1.73 m2, mean (SD) | 76.4 (19.1) | 70 (20) | 77.9 (18.5) | <0.001 |
eGFR >90 ml/min/1.73 m2 | 2095 (26) | 266 (16.4) | 1829 (28.6) | <0.001 |
eGFR 60–90 ml/min/1.73 m2 | 4455 (55.2) | 855 (52.8) | 3600 (55.9) | |
eGFR 45–60 ml/min/1.73 m2 | 967 (12) | 302 (18.6) | 665 (10.3) | |
eGFR 30–45 ml/min/1.73 m2 | 406 (5) | 161 (9.9) | 245 (3.8) | |
eGFR 15–30 ml/min/1.73 m2 | 79 (0.9) | 27 (1.7) | 52 (0.1) | |
eGFR <15 ml/min/1.73 m2 | 63 (0.8) | 10 (0.6) | 53 (0.9) | |
RBC, 106/mm3, median (IQR) | 4.58 (4.28–4.88) | 4.58 (4.23–4.89) | 4.58 (4.29–4.8) | <0.001 |
Total cholesterol, mg/dl, median (IQR) | 171 (146–203) | 167 (141–198) | 172 (148–204) | 0.006 |
High‑density lipoprotein cholesterol, mg/dl, median (IQR) | 46 (39–55) | 45 (38–53) | 47 (39–56) | <0.001 |
Low‑density lipoprotein cholesterol, mg/dl, median (IQR) | 99 (77–127) | 97 (75–124) | 99 (78–128) | 0.037 |
Triglycerides, mg/dl, median (IQR) | 117 (85–165) | 113 (82–159) | 118 (85–167) | 0.4 |
Presence of any significant stenosis on coronary angiography | 3345 (40.4) | 627 (37.5) | 2718 (41.1) | <0.001 |
LM stenosis | 245 (3) | 42 (2.5) | 203 (3.1) | 0.2 |
LAD stenosis | 2013 (24.3) | 336 (20.1) | 1677 (25.3) | <0.001 |
DIAG stenosis | 735 (8.9) | 132 (7.9) | 603 (9.1) | 0.09 |
Cx stenosis | 1096 (13.2) | 174 (10.4) | 922 (14) | <0.001 |
OM stenosis | 664 (8) | 104 (6.2) | 560 (8.5) | <0.001 |
RCA stenosis | 1481 (17.9) | 224 (13.4) | 1257 (19) | <0.001 |
Patients qualified for conservative management | 5330 (64.3) | 1126 (67.3) | 4204 (63.6) | 0.004 |
Patients qualified for the Heart Team discussion | 1161 (14) | 227 (13.6) | 934 (14.1) | 0.55 |
Patients treated with PCI | 1796 (21.7) | 321 (19.2) | 1475 (22.3) | 0.004 |
PCI LM | 34 (0.4) | 7 (0.4) | 27 (0.4) | 0.95 |
PCI LAD | 1115 (13.4) | 206 (12.3) | 909 (13.7) | 0.11 |
PCI DIAG | 182 (2.2) | 34 (2) | 148 (2.2) | 0.6 |
PCI Cx | 451 (5.4) | 81 (4.9) | 370 (5.6) | 0.2 |
PCI OM | 61 (0.7) | 13 (0.8) | 48 (0.7) | 0.83 |
PCI RCA | 404 (4.9) | 64 (3.8) | 340 (5.1) | 0.015 |
A total of 1674 (20.2%) patients had AF. Paroxysmal AF was the most frequent type of the analyzed arrhythmia. However, we found only a marginally lower prevalence of permanent AF (Figure 1).
Atrial fibrillation population
There were substantial differences in terms of clinical characteristics between groups with and without AF. Patients with AF were older, more often men, and more often had diabetes, and had higher body mass index and more frequently were diagnosed with both CKD and CHF. On the other hand, they were less likely to have history of hyperlipidemia. Mean (SD) HAS‑BLED score was 2.14 (0.87), CHA2DS2-VASc score was 3.99 (1.6).
The highest mean (SD) HAS‑BLED and CHA2DS2-VASc scores were noted in patients with permanent AF: 2.2 (0.91) and 4.3 (1.6), respectively. In patients with paroxysmal AF, the mean (SD) HAS‑BLED was 2.15 (0.84) and in persistent AF, it was 1.9 (0.81).
The lowest mean (SD) CHA2DS2-VASc score was noted in the group of patients with paroxysmal AF (3.74 [1.5]). In the group of patients with persistent AF, the mean (SD) CHA2DS2-VASc score was 3.87 (1.5). A detailed comparison between the 2 groups is shown in Table 2.
Coronary angiography
Out of 8288 patients who underwent coronary angiography, significant lesions were found in 3345 study participants (40.4%). Importantly, patients without significant CCS were more frequently women and more commonly presented with AF (Table 3). Additionally, CCS was markedly less frequently detected on coronary angiography in patients with AF than in those with sinus rhythm. Furthermore, the latter group significantly more often underwent subsequent coronary angioplasty (Table 2).
Variable | Patients with CAD (n = 3345) | Patients without CAD (n = 5483) | P value | |
Data are presented as number (percentage) of patients unless otherwise indicated.
a The percentage is calculated within the subgroup.
| ||||
Male sex | 2238 (67) | 2262 (46) | <0.001 | |
Age, y, mean (SD) | 66.9 (9.7) | 64 (10.3) | <0.001 | |
BMI, kg/m2, mean (SD) | 28.8 (4.6) | 29.33 (5) | <0.001 | |
NYHA class, median (IQR) | 3 (4–3) | 2 (2–3) | 0.04 | |
CCS class, median (IQR) | 2 (2–2) | 2 (2–2) | 0.03 | |
Left ventricular ejection fraction, %, median (IQR) | 55 (44–60) | 55 (42–60) | 0.5 | |
Chronic heart failure | 1247 (37.3) | 1443 (29.2) | <0.001 | |
HFrEF | 601 (48.2) | 780 (54.1) | <0.001 | |
HFmrEF | 301 (24.1) | 298 (20.6) | ||
HFpEF | 345 (27.7) | 365 (25.3) | ||
Hyperlipidemia | 2348 (70.2) | 3200 (64.7) | 0.001 | |
Hypertension | 2891 (86.4) | 3995 (80.8) | <0.001 | |
Diabetes mellitus | 1014 (30.3) | 1118 (22.6) | <0.001 | |
AF | Any | 627 (18.7) | 1047 (21.2) | 0.006 |
Paroxysmal | 267 (42.6)a | 490 (46.8)a | 0.09 | |
Persistent | 69 (11)a | 125 (11.9)a | 0.56 | |
Permanent | 291 (46.4)a | 432 (41.3)a | 0.04 | |
Chronic kidney disease | 824 (24.6) | 882 (17.9) | <0.001 | |
Creatinine, mg/dl, median (IQR) | 0.93 (0.81–1.1) | 0.86 (0.77–1.01) | <0.001 | |
eGFR, ml/min/1.73 m2, mean (SD) | 70 (20) | 77.8 (18.6) | <0.001 | |
eGFR >90 ml/min/1.73 m2 | 754 (23.2) | 1341 (27.9) | <0.001 | |
eGFR 60–90 ml/min/1.73 m2 | 1775 (54.5) | 2680 (55.7) | ||
eGFR 45–60 ml/min/1.73 m2 | 441 (13.6) | 526 (10.9) | ||
eGFR 30–45 ml/min/1.73 m2 | 214 (6.6) | 192 (4) | ||
eGFR 15–30 ml/min/1.73 m2 | 37 (1.1) | 42 (0.1) | ||
eGFR <15 ml/min/1.73 m2 | 32 (1) | 31 (0.6) | ||
RBC, 106/mm3, median (IQR) | 4.58 (4.26–4.89) | 4.58 (4.28–4.87) | 0.55 | |
Total cholesterol, mg/dl, median (IQR) | 169 (144–200) | 173 (147–204) | 0.008 | |
High‑density lipoprotein cholesterol, mg/dl, median (IQR) | 44 (38–52) | 48 (40–57) | 0.075 | |
Low‑density lipoprotein cholesterol, mg/dl, median (IQR) | 99 (77–125) | 99 (77–128) | 0.006 | |
Triglycerides, mg/dl, median (IQR) | 121 (87–170) | 114 (83–162) | 0.34 | |
Predictors of nonsignificant coronary findings in the multivariable analysis
In the logistic regression model, the odds ratio of nonsignificant findings on coronary angiography were 1.6‑fold higher in patients with AF than in those without AF (OR, 1.57; 95% CI, 1.32–1.87; P <0.001). The indexed OR for a 5‑kg/m2 increase in body mass index was 1.24 (95% CI, 1.15–1.35; P <0.001), and for a 5‑mg/ml increase in high‑density lipoprotein cholesterol concentration, 1.16 (95% CI, 1.1–1.24; P <0.001). The OR for CHF was 0.68 (95% CI, 0.56–0.83; P <0.001), other cardiovascular risk factors such as hypercholesterolemia, 0.64 (95% CI, 0.55–0.75; P <0.001), diabetes, 0.69 (95% CI, 0.59–0.81; P <0.001), hypertension, 0.68 (95% CI, 0.56–0.82; P <0.001), CKD, 0.79 (95% CI, 0.66–0.94; P <0.001) and women as compared with men, 0.39 (95% CI, 0.34–0.46; P <0.001). Additionally, for a 10‑year increase in age, the OR was 0.71 (95% CI, 0.65–0.76; P <0.001; Figure 2)
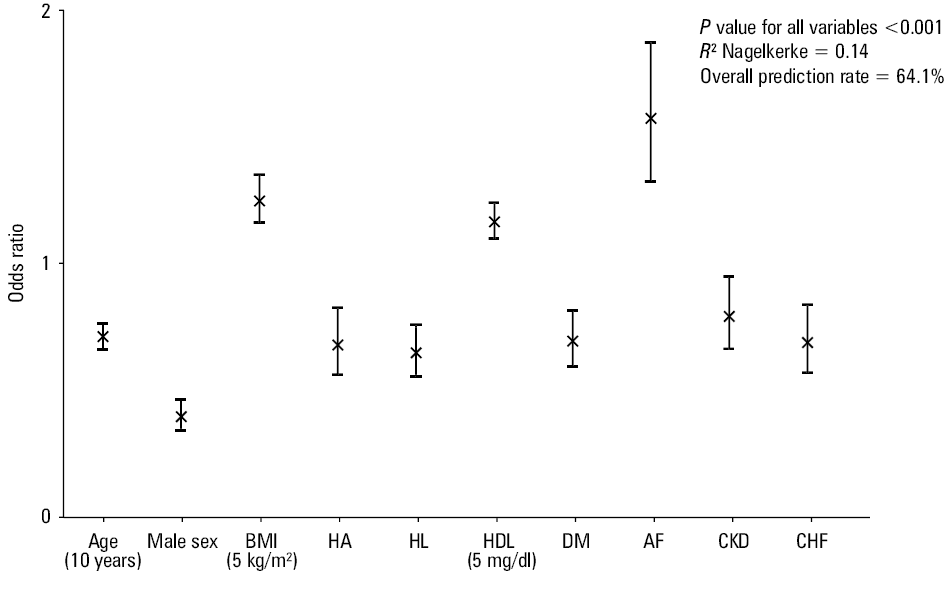
Abbreviations: CHF, chronic heart failure; CKD, chronic kidney disease; DM, diabetes mellitus; HA, hypertension; HDL, high‑density lipoprotein; HL, hyperlipidemia; others, see Figure 1 and Table 2
Complications of coronary angiography
There were 48 cases of significant vascular complications related to the puncture of the site (0.5%). In 75% of complications, the femoral artery was affected, and in 25% of cases, it was the radial artery. Out of those cases, 16 (1%) were patients with AF and 32 (0.4%) had sinus rhythm (P = 0.004).
In 9 patients (0.11%), neurological disorders associated with the procedure were recorded in 7 patients (0.1%) with sinus rhythm and in 2 patients (0.12%) with AF. All computed tomography (CT) examinations performed in these patients failed to show any signs of intracranial bleeding. In 19 patients, cardiac arrest occurred during hospitalization: 7 patients (0.4%) with AF and 12 patients with sinus rhythm (0.2%). Overall composite complications were more common in patients with AF.
Discussion
In this study, nonsignificant findings on coronary angiography were 1.6‑fold higher in patients with AF than in patients without AF. Second, AF was associated with significantly less atherosclerotic narrowing on coronary angiography (627 [37.5%] vs 2718 [41.1%] in patients without AF; P <0.001) and patients with AF less frequently underwent coronary angioplasty as compared with the population with sinus rhythm. This raises the possibility that AF may result in difficulties in selecting patients with AF for invasive procedures, given the increased findings of nonsignificant CCS on coronary angiography.
The reason for these findings might be complex and multifactorial. Patients with AF often present with typical or atypical chest pain, transient ST‑segment depression, and elevated cardiac markers. These findings may mimic symptoms of CCS.21 Moreover, rapid tachycardia is often observed in patients with AF, and ST‑segment changes at these rates have been linked with myocardial ischemia. For example, Tsigkas et al21 reported ST‑segment depression in 38% of patients with AF and rapid rhythm and only about 50% of these patients had significant CCS on coronary angiography. ST‑segment depression may frequently occur during significant tachycardia, even without CCS, and it is not necessarily typical for cardiac ischemia if the ST segment depression is less than 2 mm.21,22
Moreover, ST‑segment depression during rapid AF has less significant value than ST‑segment depression during exercise tests in patients with sinus rhythm.23 Only 4% of patients without ST‑segment depression during rapid AF had positive noninvasive tests for myocardial ischemia and CCS on angiography.23 Troponin release was shown in 15% of patients with AF and symptoms of ischemia, although CCS at angiography was absent.25 In a database of patients referred for coronary angiography, history of AF correlated with no obstructive CCS.24,26
On the other hand, Kralev et al27 showed that left main stem and right coronary artery (RCA) disease was present more frequently in patients with AF compared with controls. They also suggested that significant atherosclerotic narrowing in the proximal RCA and the circumflex artery (Cx) prior to the takeoff of the atrial arteries raises the risk of AF. In our study, significant RCA and Cx disease were less common than in patients with sinus rhythm. Another analysis of 3220 patients referred for coronary angiography revealed that only 43% of patients with CCS and AF had a diseased RCA or Cx.21
Does AF contribute to CCS or vice versa? There is a debate on this topic and opinions are often contradictory. Motloch et al28 found that the anatomical distribution of coronary artery stenoses did not contribute to AF in CCS patients; however, AF was linked to worse CCS severity, which might predispose individuals to AF by driving ischemic heart disease and changes in left ventricular function. In our study, patients with AF had less prevalent multivessel CCS. It is possible that in patients with AF, ischemia at the level of microcirculation of the myocardial muscle (rather than epicardial vessels) is responsible for the presence of typical angina. Unfortunately, our study did not explore the impact of cardiac ischemia induced by coronary small‑vessel disease.
Our findings reflect difficulties with selecting AF patients for invasive coronary investigations. In the general population, the sensitivity of exercise testing ranges from 60% to 70% and specificity is approximately 85%.29 As mentioned before, ST‑segment depression is a common finding in AF patients,30 and ST‑depression during rapid AF has relatively higher sensitivity and lower specificity, when compared with exercise testing. Thus, the absence of ST‑depression during rapid AF has satisfactory sensitivity for excluding significant CCS.21 Low positive predictive values for significant CCS of ST‑segment depression have been reported at approximately 32%.23,24 Patients with AF are not optimal candidates for coronary CT angiography during a rapid cardiac rhythm. However, it is a good diagnostic modality for patients in sinus rhythm with low CCS probability.
Not only are patients with AF improperly referred for invasive coronary investigations, but they are at an increased risk of complications. In a study of 13 498 patients, it was shown that patients with a history of AF were more likely to have post procedural bleeding, more often needed blood transfusion, and more often had exacerbation of heart failure, cardiogenic shock, and in‑hospital mortality, but there were no differences in the incidence of postprocedural stroke or vascular complications in matched cohorts.30,31 Similarly, several studies reported that AF patients were more likely to experience postprocedural heart failure and cardiogenic shock.32-34 In the present study, there were 48 cases of significant vascular complications concerning femoral and radial artery related to the puncture of the site, and were more frequent in patients with AF than patients with sinus rhythm. Also, neurological disorders associated with the procedure were recorded more frequently in patients with AF than those with sinus rhythm. All CT examinations performed thereafter did not show signs of intracranial bleeding. Cardiac arrest during hospitalization was numerically higher in patients with AF. Apart from this, it was already demonstrated that AF patients with NSTEMI undergoing PCI can be predisposed to contrast induced nephropathy.35
Limitations
Our study has several limitations. First, our findings were obtained in a retrospective single‑center study and should be confirmed in a multicenter prospective study. However, our data represent real life, as they were obtained during daily clinical practice. Second, we excluded from our analysis patients with ACS. Third, fractional flow reserve measurements were not performed on regular basis. This could cause an inaccurate assessment of the significance of coronary stenosis. Therefore, only cases of stenosis with a reduction of 70% were defined as significant.32 Fourth, we were able neither to reliably assess stress tests before invasive diagnostics nor to measure concentrations of natriuretic peptides. Fifth, our study did not explore the impact of myocardial ischemia induced by coronary microvascular disease. Six, patients with AF were less likely to have lipid disorders, which may affect the results. Seven, due to a very large group of patients included in the study (nearly 10 000) and nearly 10 years of analysis (2007–2016), we were unable to obtain reliable data on smoking in the analyzed group. Over the years, the approach to smoking addiction and the way it is coded has changed. Our diagnoses were based on the diagnoses established by the physicians in charge and were not verified again. Additionally, it would be interesting to perform more detailed echocardiographic examinations of all study participants. Furthermore, retrospective chart databases provide easy and cheap access to large numbers of patients although limitations such as potential selection bias should be taken into consideration. The last thing, one of the subtypes of AF is newly diagnosed AF. As there is no specific ICD code for it, we were not able to distinguish this type of AF.
Conclusions
In our study, AF was associated with the absence of significant coronary lesions on angiography and less frequent need for revascularization, reflecting difficulties with qualifying AF patients for invasive CCS diagnostic workup. Multiple factors might be the reason for these findings, namely, AF symptoms may mimic CCS symptoms, ST‑segment depression during AF pootly predicts obstructive CCS, stress tests are rarely proceeded in patients with AF, and rapid rhythm makes CT scan difficult to interpret. Our findings suggest the need for a more efficacious noninvasive diagnostic approach for patients with AF and suspected CCS.
- Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace. 2016; 18: 1609‑1678. | Crossref
- Potpara TS, Mujovic N, Lip GYH. Meeting the unmet needs to improve management and outcomes of patients with atrial fibrillation: fitting global solutions to local settings. Pol Arch Intern Med. 2019; 129: 574‑576. | Crossref
- Michniewicz E, Mlodawska E, Lopatowska P, et al. Patients with atrial fibrillation and coronary artery disease – double trouble. Adv Med Sci. 2018; 63: 30‑35. | Crossref
- Bednarski J, Balsam P, Tymińska A, et al. District versus academic hospitals: differences in the clinical characteristics of patients with atrial fibrillation without valvular heart disease treated with oral anticoagulants. Pol Arch Intern Med. 2018; 128: 274‑279. | Crossref
- Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020; 41: 407‑477.
ARTICLE INFORMATION