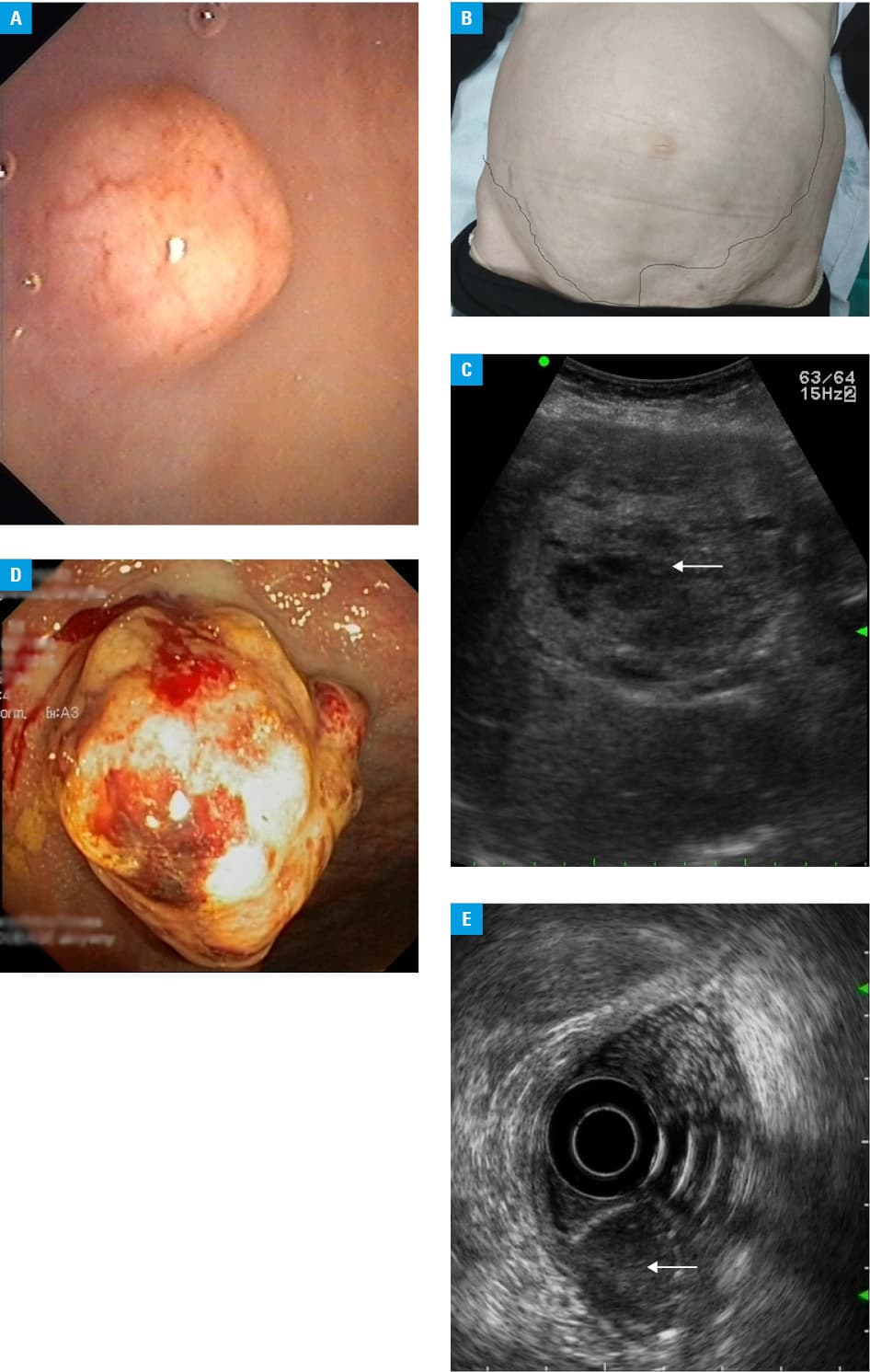
A 74‑year‑old woman was referred to the endoscopy unit for colonoscopy because of a change in bowel habits. The examination revealed a wide‑base polypoid lesion in the rectum, 10 mm in size, with the typical appearance of a neuroendocrine tumor (NET): yellowish, with normal intact covering mucosa (Figure 1A). Contrary to guidelines, a hot snare polypectomy was used to remove the lesion. The histopathological examination showed a well‑differentiated (G1) NET with a positive vertical margin. The patient did not make an appointment for follow‑up visits. After 53 months, she was referred to the department of gastroenterology with right hypochondriac pain, weight loss, and recurrent episodes of fresh blood in stool. The physical examination revealed abdominal distension with enormous liver enlargement (Figure 1B). Abdominal ultrasound (Figure 1C) and computed tomography scan showed numerous metastatic lesions in the liver, bones, and adrenal glands. The bulging, bleeding tumor of the rectum, invading the muscularis propria layer was shown on endosonography (Figure 1D and 1E). The biopsy confirmed the neuroendocrine origin of the tumor. Despite treatment with chemotherapy, the patient died after 6 months.
Rectal NETs originate from the muscularis mucosa and grow towards the submucosa.1 Therefore, polypectomy with diathermic loop or forceps biopsy, routinely performed during colonoscopy in the case of epithelial polyps, rarely leads to radical treatment in rectal NETs.1 Most rectal NETs have a characteristic morphological image: they are nodules on a wide base with a smooth surface, yellow color, and with a hollow center or hyperemia.1 These features allow for making a proper diagnosis during colonoscopy and applying recommended treatment according to the tumor size, grade, and stage: endoscopic submucosal dissection, endoscopic mucosal resection, transanal endoscopic microsurgery, or surgical treatment.1 When radical treatment is applied, the prognosis for rectal G1 NETs of the diameter up to 10 mm is very good, with nearly 100% 5‑year survival rate, and these tumors do not even require follow‑up.1 Unfortunately, in spite of clear recommendations, which is apparent based on our patient’s history and other studies, majority of these lesions are resected with snare polypectomy2,3 which may lead to incomplete resection, and subsequently metastatic spread.2-5 Moreover, an important factor that led to the fatal outcome was the fact that the patient was lost to follow‑up. There are no clear and evidence‑based guidelines showing optimal management in case of nonradical resection of rectal NET; in such case, either a close follow‑up or a salvage therapy of the scar with endoscopic submucosal dissection or transanal endoscopic microsurgery should be applied.4 Therefore, considering the mistakes we see in our practice, we decided to present this case to underline the importance of complying with the guidelines and to show potential fatal consequences of ignoring the recommendations in rectal NETs.
- Starzynska T, Londzin‑Olesik M, Baldys‑Waligorska A, et al. Colorectal neuroendocrine neoplasms ‑ management guidelines (recommended by the Polish Network of Neuroendocrine Tumours). Endokrynol Pol. 2017; 68: 250‑260.
- Dąbkowski K, Białek A, Rusiniak‑Rossińska N, et al. Endoscopic treatment of rectal neuroendocrine tumors in a 12 year retrospective single center study. ESGE Days 2019; Prague2019. Endoscopy. 2019; 51: 137. | Crossref
- Fine C, Roquin G, Terrebonne E, et al. Endoscopic management of 345 small rectal neuroendocrine tumours: A national study from the French group of endocrine tumours (GTE). United European Gastroenterol J. 2019; 7: 1102‑1112. | Crossref
- Dąbkowski K, Szczepkowski M, Kos‑Kudła B, Starzynska T. Endoscopic management of rectal neuroendocrine tumours. How to avoid a mistake and what to do when one is made? Endokrynol Pol. 2020; 71: 343‑349. | Crossref
- Gleeson FC, Levy MJ, Dozois EJ, et al. Endoscopically identified well‑differentiated rectal carcinoid tumors: impact of tumor size on the natural history and outcomes. Gastrointest Endosc. 2014; 80: 144‑151. | Crossref
ARTICLE INFORMATION