Intravenous leiomyomatosis as an unusual cause of the misdiagnosis of deep vein thrombosis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Intravenous leiomyomatosis as an unusual cause of the misdiagnosis of deep vein thrombosis
Intravenous leiomyomatosis (IVL) is a form of uterine leiomyoma that permeates into the venous system and grows along the vessel wall. Although histologically benign, biologically, it has malignant properties due to a potential to cause intracardiac extension, which may lead to heart failure and death. Intravenous leiomyomatosis was first described by Birch‑Hirschfeld in 1896 in Germany. Since then, around 300 cases of IVL have been reported in the medical literature.
Benign metastasizing leiomyoma is another rare condition that manifests as metastasizing uterine leiomyoma, most often to the lung. Coexisting conditions in a single patient are extremely rare and, therefore, about 60 cases have been reported in the literature so far.1-3 Here, we present the case of a patient with IVL extending to the right heart and metastasizing to the lung as well as with leiomyoma of the left ovary, treated with surgery and hormonal therapy.
A 50‑year‑old woman with a history of papillary thyroid cancer treated 7 years earlier was admitted to the hospital because of heavy menstrual bleeding and anemia. Pelvic ultrasonography was performed and showed massive uterine fibroids. Hysterectomy was carried out and the patient was rehospitalized for right flank pain and hematuria a week after the surgery. Hydronephrosis was diagnosed based on computed tomography (CT) findings (Figure 1A). Additionally, the CT scan demonstrated intravenous masses in the inferior vena cava (IVC), with channels of proper blood flow, which prompted the diagnosis of deep vein thrombosis (DVT) (Figure 1B). Additional diagnostic workup involving thoracic and pelvic areas was implemented. The examinations showed intravenous masses extending from the right atrium of the heart to the common iliac veins (Figure 1C and 1D).
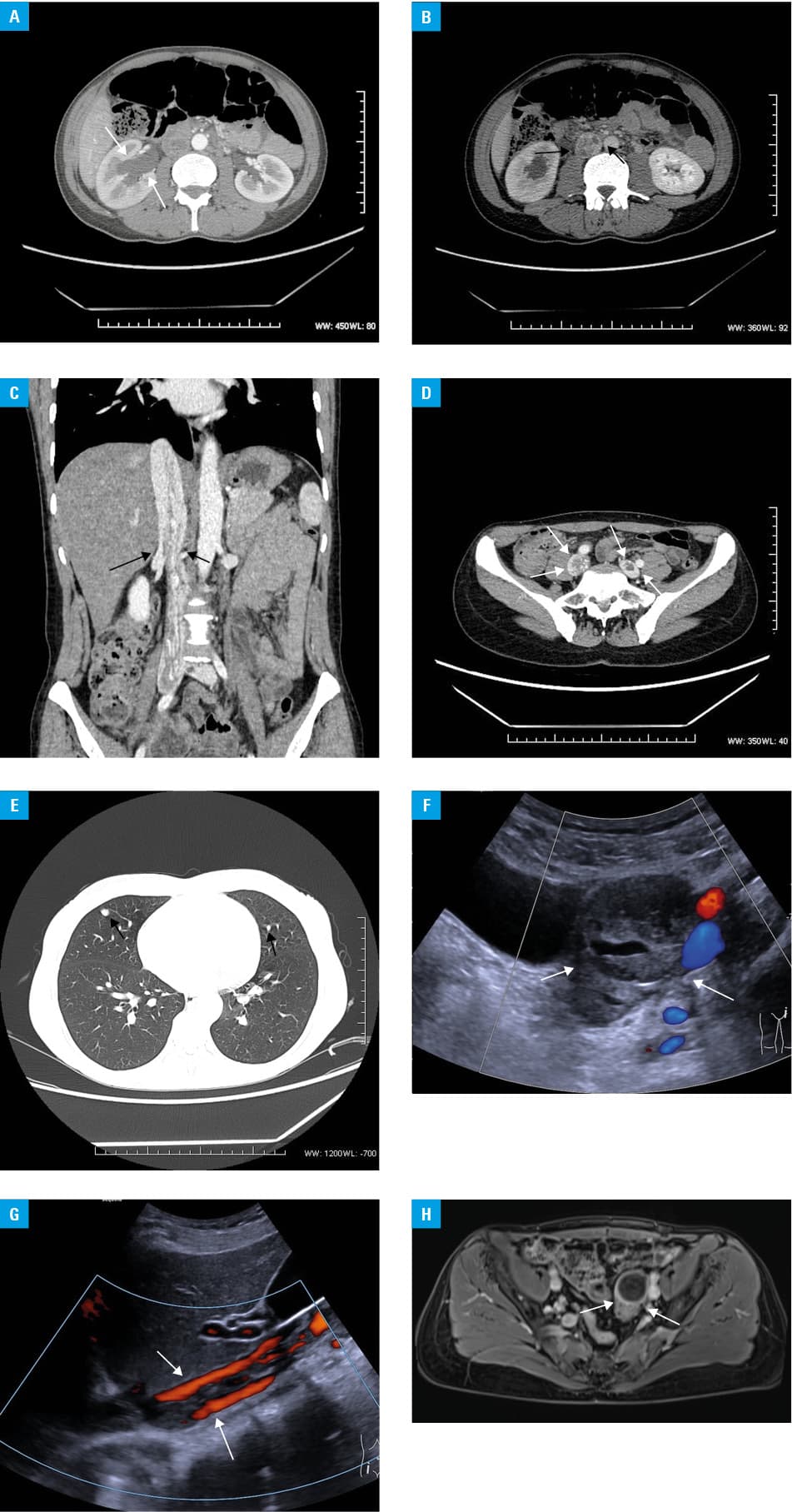
Anticoagulation therapy was initiated, although the patient did not show any clinical symptoms of DVT and her D‑dimer levels were low (302 μg/l). Moreover, chest CT revealed a few nodules of up to 13 mm in diameter in the right and left lungs, regarded as metastases of unknown origin (Figure 1E).
Positron emission tomography combined with CT did not show any lesions with greater 18F‑fluorodeoxyglucose uptake. After a month of pharmacological therapy, no recurrence of intravenous masses was observed. Right atrial and iliac vein masses were surgically removed. During sternotomy and laparotomy, the myomatous tissue was removed from the heart, iliac veins, and the IVC. The histological examination confirmed the diagnosis of IVL. Two months after the surgery, Doppler ultrasound showed new tumor tissue growing in the IVC (Figure 1F), and IVL of the IVC and iliac veins recurred a year after the procedure. Fortunately, the cardiac chambers remained normal. Moreover, contrast‑enhanced magnetic resonance imaging and ultrasound showed new lesions of similar morphology in the left ovary (Figure 1G and 1H). Currently, the patient receives antiestrogen therapy, as some studies have indicated hormonal influence on the clinical course of the disease.4 On physical examination, slight wheezes have been heard, but the patient shows no suspicious clinical features and remains under clinical surveillance.
To conclude, although IVL is a very rare entity, it could be underestimated due to its possible oligosymptomatic course.5 In order to avoid misdiagnosis (of DVT or metastases) and overtreatment, the disease should always be considered in middle‑aged women with a history of uterine fibroids and characteristic intravenous masses.
- Diakomanolis E, Elsheikh A, Sotiropoulou M, et al. Intravenous leiomyomatosis. Arch Gynecol Obstet. 2003; 267: 256‑257. | Crossref
- Jing D, Xiulan Z, Donghui G, et al. Intravenous leiomyomatosis of the uterus: a clinicopathologic study of 18 cases, with emphasis on early diagnosis and appropriate treatment strategies. Hum Pathol. 2011; 42: 1240‑1246. | Crossref
- Miller J, Shoni M, Siegert C, et al. Benign metastasizing leiomyomas to the lungs: an institutional case series and a review of the recent literature. Ann Thorac Surg. 2016; 101: 253‑258. | Crossref
- Bonder‑Adler B, Bartl M, Wagner G. Intravenous leiomyomatosis of the uterus with pulmonary metastases or a case with benign metastasizing leiomyoma? Anticancer Res. 2009; 29: 495‑496.
- Gunderson C, Parsons B, Penaroza S, et al. Intravenous leiomyomatosis disguised as a large deep vein thrombosis. J Radiol Case Rep. 2016; 10: 29‑35. | Crossref
ARTICLE INFORMATION