An oncogenic, somatic mutation of PIK3CA identified in 2 primary malignancies: clear cell renal cell carcinoma and prostate adenocarcinoma in the same patient



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
An oncogenic, somatic mutation of PIK3CA identified in 2 primary malignancies: clear cell renal cell carcinoma and prostate adenocarcinoma in the same patient
Introduction
Clear cell renal cell carcinoma (ccRCC) is the most lethal and prevalent histological subtype of renal cell carcinomas (RCC).1 The ccRCC morbidity is particularly high in Central European countries, with the peak in Czech Republic (28.9 cases per 100 000) and Poland (20 cases per 100 000), which remains an unexplained phenomenon.2 Currently, there is a demand to develop molecular strategies allowing preoperative diagnosis of ccRCC, detection of recurrences, and supporting therapeutic decision making. Novel ccRCC‑associated mutations and therapeutic targets can be potentially uncovered by targeted sequencing of gene regions that frequently harbor actionable / druggable mutations in various types of tumors.
In this study we sequenced the “hotspot” DNA regions in 50 known cancer genes in adult Polish patients with ccRCC (Slavic ethnic group) and matched controls with the purpose to uncover novel germline / somatic mutations associated with this disease. Unexpectedly, we have identified the first case of ccRCC with an highly oncogenic, rapamycin‑sensitive mutation of the PIK3CA gene (COSM754), and confirmed the presence of the same somatic variant in primary prostate adenocarcinoma diagnosed in the same patient during the follow‑up period.
Patients and methods
Ethics statement
This study was approved by the Institutional Ethics Committee of the Regional Specialized Hospital in Wrocław, Poland (no. KB/nr 9/rok 2016). All samples were collected at the Regional Specialized Hospital after obtaining written informed consent from study participants. The research was conducted in accordance with the Helsinki Declaration.
Patients
Blood samples were drawn from 23 healthy individuals (age range, 23–55 years; 11 men and 12 women), 13 disease controls (3 patients with oncocytoma, 2 with papillary carcinoma, 5 chromophobe renal cell carcinoma, and 3 with unclassified RCC; age range, 36–76 years), and 20 patients with ccRCC (age range, 48–89 years; 11 men and 9 women). Fresh renal tumor samples were obtained after partial or radical nephrectomy. This study also utilized 2 formalin‑fixed paraffin‑embedded (FFPE) prostate cancer samples, one from a patient with ccRCC whose renal tumor was positive for PIK3CA alteration (COSM754), and one from a patient with ccRCC whose kidney tumor was negative for PIK3CA alteration (a negative control for target sequencing).
Targeted sequencing of cancer‑associated genes and data analysis
The genomic DNA was purified from blood, and tumor specimens using PureLink genomic DNA mini kit (Thermo Fisher Scientific, Waltham, Massachusetts, United States). The quality of DNA was assessed on agarose gel stained with ethidium bromide, and the quantity of DNA was measured using the Qubit 2.0 fluorometer (Thermo Fisher Scientific). The mutational status of “hotspot” regions (encompassing 2856 COSMIC mutations) in 50 cancer‑related genes (ABL1, EGFR, GNAS, KRAS, PTPN11, AKT1, ERBB2, GNAQ, MET, RB1, ALK, ERBB4, HNF1A, MLH1, RET, APC, EZH2, HRAS, MPL, SMAD4, ATM, FBXW7, IDH1, NOTCH1, SMARCB1, BRAF, FGFR1, JAK2, NPM1, SMO, CDH1, FGFR2, JAK3, NRAS, SRC, CDKN2A, FGFR3, IDH2, PDGFRA, STK11, CSF1R, FLT3, KDR, PIK3CA, TP53, CTNNB1, GNA11, KIT, PTEN, VHL) was explored in the blood, and tumor‑derived DNA by targeted next‑generation sequencing. The amplicon libraries were prepared with the optimized Ion AmpliSeq Cancer Hotspot Panel v2 (Thermo Fisher Scientific) using 1 to 10 ng DNA. The sequencing was performed on an Ion Torrent PGM Sequencing platform (Thermo Fisher Scientific) using Ion 314 Chips (Thermo Fisher Scientific). The sequencing data were analyzed on the Ion Torrent Server using the variant caller and coverage analysis plugins. The depth of coverage ranged from 203‑fold to 2040‑fold (depending on the library), and the uniformity ranged from 99.2% to 100%. The cutoff for a variant to be considered true was ≥100 × coverage and ≥5% frequency (in case of cancer samples). The detected variants were filtered against COSMIC and dbSNP database to identify known and novel mutations. Functional significance of all variants was determined using the wAnnovar tool (http://wannovar.wglab.org).3 The predicted effect of the novel mutation was assessed using PolyPhen‑2.4 Comparative mutational analysis of the paired RCC blood / tumor samples was performed to distinguish germline variants from somatic mutations.
Sanger sequencing
The new NOTCH1 mutation and the highly oncogenic PIK3CA variant identified by high‑throughput sequencing were validated with Sanger sequencing. The polymerase chain reaction products were generated form paired ccRCC tumor, and blood DNA samples. The polymerase chain reactions were conducted using GoTaq Flexi kit (Promega, Madison, Wisconsin, United States). The primer sequences used to amplify PIK3CA were: (F) ACGCATTTCCACAGCTACAC, (R) AACAAAGGACTGTGAGCTGT, and the sequences of primers used to amplify NOTCH1 were: (F) ACTGCAAGGACCACTTCAGC, (R) AGACCACGTTGGTGTGCAG. The sequencing reactions were performed using forward primers. The electropherograms were visually inspected using Finch TV (Geospiza, Seattle, Washington, United States).
Results and discussion
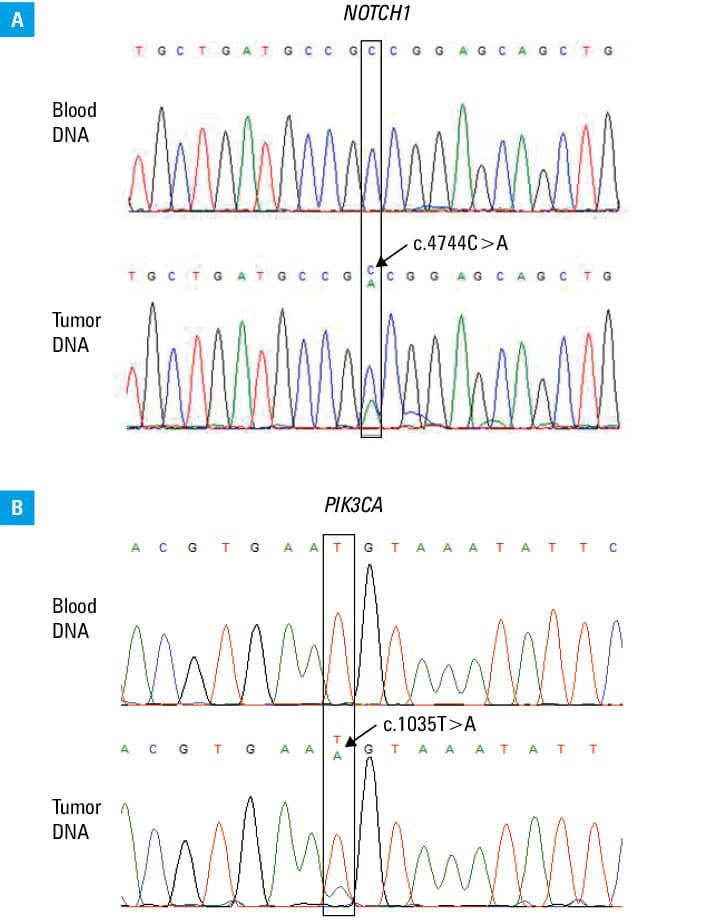
Comparative analysis of the genotype profiles between healthy subjects, ccRCC cases, and disease controls did not reveal any differences in the germline DNA. However, it allowed detection of ccRCC tumor–specific changes (known and novel) in 45% of cases (Supplementary material, Table S1). In total, 8 known, different VHL mutations have been discovered separately in 8 different patients (40%). A single patient with ccRCC who harbored pathogenic VHL alteration also carried a novel point mutation in the NOTCH1 gene (c.4744C>A; p.P1582S). The exonic NOTCH1 mutation, changing proline to threonine in the nonconserved region of the extracellular domain was predicted by PolyPhen‑2 to be deleterious (score 1).4 The mutation resides in the genomic region occupied by histone marks of active transcription, that is, H3K36me3 and H4K20me1 (Histone Modifications by ChIP‑seq from ENCODE/Broad Institute, GEO accession: GSE29611, PMID: 22955616), and may potentially alter the expression of the gene. According to the in silico analyses performed using the Mutation Tester tool,5 the p.P1582S variant alters the secondary structure of the NOTCH1 oncoprotein by causing a loss of an helix motif (1582aa‑1587aa), and also affects the extracellular topological domain spanning from amino acid residue 19 to 1735. The novel NOTCH1 gene mutation identified in ccRCC tumor was positively verified by Sanger sequencing (Figure 1A). The NOTCH1 alteration was identified in a 66‑year‑old female patient with T1 stage ccRCC tumor, limited to the kidney. Interestingly, our study also detected somatic, highly oncogenic PIK3CA mutation (c.1035T>A; p.N345K; COSM754) in a patients with ccRCC (74‑year‑old man; T3 stage ccRCC tumor limited to the kidney).6 The mutation was present in approximately 28% of sequencing reads encompassing the c.1035 position in the PIK3CA gene. The mutation has been successfully confirmed by low‑throughput sequencing (Figure 1B). The subject with COSM754 variant was the only representative of the ccRCC group, who developed another primary malignant neoplasm, that is, prostate adenocarcinoma during the follow‑up period (2.5 years post ccRCC resection). Because former studies showed that primary prostate adenocarcinoma develops in patients with RCC more frequently than expected (as synchronous or subsequent malignancy), we have sequenced the cancer‑associated genes in the prostate cancer (FFPE sample) in order to evaluate the genetic similarities between ccRCC and prostate cancer which occurred in the same man.7 Surprisingly, the COSM754 variant was detected in 10% of sequencing reads in prostate cancer sample. Possibly, the true allelic ratio of the mutant to the wild‑type allele was higher in the prostate cancer, as the DNA subjected to sequencing was derived from a tissue section that included both normal (in advantage) and transformed cells.
Novel ccRCC‑related mutations possessing diagnostic, prognostic, and predictive value can be potentially revealed by targeted sequencing of oncogenes and tumor suppressor genes known to carry clinically “meaningful” mutations in other types of cancers.
In this study, we have performed targeted, high‑throughput screening of “hotspot” regions in 50 genes commonly implicated in tumorigenesis with the aim to capture possible germline and somatic alterations associated with ccRCC tumors among Polish representatives. We have found that a significant number of ccRCC cancers (40%) from Polish patients harbored VHL mutations, which is a well‑known phenomenon. We also discovered a novel point mutation in the NOTCH1 protooncogene, which was in silico predicted to be deleterious. Most importantly, this study identified the first case of a patient with ccRCC and with somatic, highly oncogenic, rapamycin‑sensitive PIK3CA mutation (c.1035T>A; p.N345K; COSM754). The nonsynonymous COSM754 variant is a rare alteration that has been previously identified in several types of neoplasms, that is, breast, large intestine, central nervous system tumors, and prostate adenocarcinoma, but to our knowledge, it was never found in ccRCC.8-10 Surprisingly, we were able to detect this mutation in the primary prostate adenocarcinoma diagnosed in the same patient during the follow‑up period.
The PIK3CA oncogene encodes for p110α protein which is a catalytic subunit of class I phosphatidylinositol 3‑kinase (PI3K). PI3K is a crucial component of the signaling cascade PI3K / AKT / mTOR that plays a pivotal role in cell growth, proliferation, and survival. Constitutive activation of PI3K / AKT / mTOR, which is commonly induced by gain‑of‑function mutations in PI3K, leads to malignant transformation. Mutations of the PIK3CA gene and alterations of the PIK3CA pathway are frequent, both in ccRCC and prostate adenocarcinomas.11,12 As ccRCC and prostatic adenocarcinoma detected in the same patient did not share morphologic and immunohistochemical features, we have a hypothesis that these primary neoplasms evolved from clones of the same ancestral cell affected by the COSM754 mutation.
The main limitations of our study include small sample size and limited coverage of gene coding regions. Further population‑based sequencing studies are needed to verify the putative link between the mutational status of PIK3CA and synchronous / sequential occurrence of ccRCC and prostate cancer in the same patient.
- Moch H, Bonsib SM, Delahunt B, et al. Clear cell renal cell carcinoma. In: Moch H, Humphrey PA, Ulbright TM, Reuter VE, eds. World Health Organization (WHO) classification of tumours of the urinary system and male genital organs. Lyon: IARC Press; 2016: 120‑123.
- Protzel C, Maruschke M, Hakenberg OW. Epidemiology, aetiology, and pathogenesis of renal cell carcinoma. Eur Urol Suppl. 2017; 11: 52‑59. | Crossref
- Yang H, Wang K. Genomic variant annotation and prioritization with ANNOVAR and Wannovar. Nat Protoc. 2015; 10: 1556‑1566. | Crossref
- Adzhubei IA, Schmidt S, Peshkin L, et al. A method and server for predicting damaging missense mutations. Nat Methods. 2010; 7: 248‑249. | Crossref
- Schwarz JM, Cooper DN, Schuelke M, Seelow D. MutationTaster2: mutation prediction for the deep‑sequencing age. Nat Methods. 2014; 11: 361‑362. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION