Long-term outcomes of 11 021 patients with chronic coronary syndromes and after coronary angiography: the PRESAGE registry
Key words: conservative treatment, coronary artery disease, long-term outcomes, revascularization



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Long-term outcomes of 11 021 patients with chronic coronary syndromes and after coronary angiography: the PRESAGE registry
Introduction: There is a paucity of real‑world registries concerning patients with chronic coronary syndromes (CCS).
Objectives: We aimed to assess the long‑term outcomes of patients with CCS and after coronary angiography performed in accordance with the treatment strategy.
Patients and methods: The analysis involved 11 021 patients treated in a single center between 2006 and 2016 who were enrolled into the ongoing PRESAGE registry. Based on the results of coronary angiography and the treatment strategy adopted, patients were classified into 4 groups: with nonsignificant lesions (n = 3637), undergoing percutaneous coronary intervention (n = 4678), undergoing coronary artery bypass grafting (CABG; n = 997), and receiving conservative treatment (notwithstanding significant lesions on an angiogram; n = 1709). All‑cause death, assessed in every study group at 1-, 3-, and 5‑year follow‑up, was regarded as the primary outcome measure.
Results: The mean (SD) age of the study patients was 64.6 (9.5) years, and women constituted 35% of the cohort. Patients treated conservatively were the oldest (mean [SD] age, 64.9 [9.3] years) in the group and showed the highest prevalence of previous myocardial infarction (50.5%), CABG (31.8%), diabetes (40.3%), chronic total occlusion (65.5%), and left ventricular ejection fraction below 35% (24.4%). Death from any cause in patients with nonsignificant lesions, undergoing percutaneous coronary intervention, undergoing CABG, and receiving conservative treatment occurred 5 years following the index hospitalization in 11.2%, 16.2%, 9.7%, and 21% of those patients, respectively.
Conclusions: The PRESAGE registry provides valuable information about the clinical characteristics and long‑term outcomes of patients with CCS. The population of CCS patients is heterogeneous, and long‑term prognosis is also varied. The poorest characteristics and outcomes were reported in patients with significant lesions and ineligible for revascularization procedures.
What's new?
In the PRESAGE registry, we observed the treatment outcomes of patients diagnosed with chronic coronary syndromes based on coronary angiography. The worst prognosis was noted in patients with chronic coronary syndromes, confirmed significant lesions, and those who did not receive revascularization. Therefore, our analysis confirmed the key role of coronary angiography in the management and treatment of patients with chronic coronary syndrome. This modality enabled us to assess the risk of cardiac events and to implement appropriate treatment including revascularization.
Introduction
Chronic coronary syndromes (CCS; previously: stable angina) represent a prevalent manifestation of coronary artery disease (CAD), with an incidence (depending on the adopted definition) of approximately 5% to 12% of the population over 45 years of age.1 The number of patients with CCS is likely to rise because of prolonged life expectancy, the growing incidence of diabetes, and the improved survival of patients with acute coronary syndrome (ACS).2-4 Although significant advances in the diagnostic workup as well as the pharmacological and invasive treatment of CAD have been implemented in clinical practice over past decades, the number of studies regarding the management of patients with CCS is scarce.5-12 Randomized controlled trials are usually performed in carefully selected populations, which are often not representative of patients encountered in daily practice in terms of clinical characteristics, management, and treatment.7-11 International registries representing heterogeneous populations often recruit ambulatory patients from various countries and selected centers.6-11
Therefore, considering a large number of patients with CAD in our center and the possibility to provide complete data on diagnostic workup and therapeutic management, we decided to launch a large observational study of patients with CCS: the Prospective Registry of Stable Angina Management and Treatment (PRESAGE; ClinicalTrials.gov identifier, NCT03781492). The aim of our study was to assess the long‑term outcomes of patients with CCS who underwent coronary angiography, stratified using the treatment strategy.
Patients and methods
Registry design
The PRESAGE registry is a single‑center, prospective, observational study recruiting consecutive patients who underwent coronary angiography and were discharged from the 3rd Department of Cardiology, Silesian Centre for Heart Diseases in Zabrze, Poland, with the diagnosis of CCS.13 The hospital is a highly specialized cardiology center with cardiac surgery facilities. To obtain complete long‑term data, only patients from the Silesia province, inhabited by 4.5 million residents, were selected for analysis. The diagnosis of CCS was based on clinical manifestations, coronary angiography results, and the current guidelines of the European Society of Cardiology (ESC).14-16 The ESC recommendations for the management and treatment of CCS changed during the study period (ESC Guidelines 1997,14 2006,15 and 201316). Patients with vasospastic and / or microvascular angina were also included in the registry. Diagnostic and therapeutic strategies, including pharmacological and interventional treatment, were implemented in accordance with the current recommendations of the ESC.14-16 Patients presenting several times in our center were assessed as a single patient (data from the first hospitalization were included). Missing data were not imputed.
The study was approved by the institutional review board and conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. Due to the retrospective design of the study, no additional patient consent was required.
Data collection
The PRESAGE registry included patients hospitalized between January 2006 and December 2016. Complete patient demographics, clinical characteristics, as well as diagnostic and therapeutic data were obtained by reviewing the hospital records. The analysis involved the occurrence of in‑hospital events including nonfatal myocardial infarction (MI), major bleeding, contrast‑induced nephropathy, and death. A subsequent analysis was based only on the data from the first hospitalization due to CCS. Follow‑up data were available for all enrolled patients and were acquired from the Polish National Health Fund (Narodowy Fundusz Zdrowia).
Definitions
Hypertension was defined as persistent systolic blood pressure of at least 140 mm Hg or systolic blood pressure of at least 90 mm Hg, or treatment with hypotensive drugs due to the known diagnosis of hypertension. Diabetes was diagnosed if the patient had a fasting plasma glucose level exceeding 125 mg/dl (7 mmol/l) at 2 examinations, a random plasma glucose level higher than 200 mg/dl (11.1 mmol/l), or a history of diabetes including treatment with diet, oral medications, or insulin. Hypercholesterolemia was defined as a baseline cholesterol level higher than 200 mg/dl (5.2 mmol/l) and / or a low‑density lipoprotein cholesterol level above 130 mg/dl (3.4 mmol/l), or previously diagnosed and treated hypercholesterolemia. Obesity was diagnosed if the body mass index was greater than or equal to 30 kg/m2. Peripheral artery disease was defined as at least one of the following: a history of or current intermittent claudication, angioplasty of lower extremity arteries, stenting or peripheral artery bypass grafting, previous amputation affecting the lower extremity, and atherosclerosis within the main arteries (aorta, renal arteries, carotid arteries, and others), confirmed by imaging. A positive family history of premature CAD was recognized if CAD was revealed in a first‑degree relative below 50 years of age in men and below 60 years of age in women. Significant CAD was defined as an angiographically significant stenosis of the coronary arteries of at least 2 mm in diameter, as determined by visual assessment or fractional flow reserve ≤0.8. A stenosis ≥50% of the left main artery or the proximal segment of the left anterior descending artery and a stenosis ≥70% in other segments was recognized as angiographically significant. Nonsignificant CAD was defined as stenosis <50% in the left main artery or the proximal left anterior descending artery and stenosis <70% in other segments of the coronary arteries with a diameter of at least 2 mm, as determined by visual assessment or fractional flow reserve >0.8. Smooth coronary arteries were defined as the absence of any atherosclerotic lesions in the coronary vessels. Major bleeding was defined as a clinically evident hemorrhage: 1) with an ensuing drop in hemoglobin levels greater than 5 g/dl (3.1 mmol/l) or a decrease in hematocrit >15%; 2) resulting in hemodynamic disorders; or 3) requiring blood transfusion. Contrast‑induced nephropathy was defined as impaired renal function, based on a relative (≥25%) or absolute (≥44 µmol/l) increase in the serum creatinine level up to 3 days after the first or subsequent coronary angiography examination in the absence of an alternative explanation of renal dysfunction.
Death defined as death from any cause was regarded as the primary outcome measure. The secondary outcome measures included nonfatal MI, ACS‑driven revascularization, and stroke. Additionally, the total rate of adverse events during follow‑up was presented. Nonfatal MI was defined as an ischemic event that met the ESC / American College of Cardiology criteria for MI.17 Nonelective ACS‑driven revascularization was defined as an additional, unplanned percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) procedure, performed in an urgent manner because of acute ischemic symptoms.18
Study groups
Based on the results of coronary angiography and the treatment strategy, patients were classified into 4 groups: patients with nonsignificant lesions (n = 3637), patients undergoing PCI (n = 4678), patients undergoing CABG (n = 997), and patients receiving conservative treatment (notwithstanding significant lesions on an angiogram; n = 1709).
Patients with significant valvular and neoplastic diseases were excluded from the analysis. Based on coronary angiography results, the study patients were categorized as having nonsignificant or significant lesions of the coronary arteries. Patients with significant lesions were assigned to one of the groups receiving treatment: PCI, CABG, or conservative treatment. Finally, the study patients were classified into 4 groups: nonsignificant lesions, PCI, CABG, and conservative treatment (Figure 1). The groups were divided according to the initial treatment strategy (intention‑to‑treat). An attempt to introduce the coronary guidewire (effective or failed) qualified the patient to the PCI group.
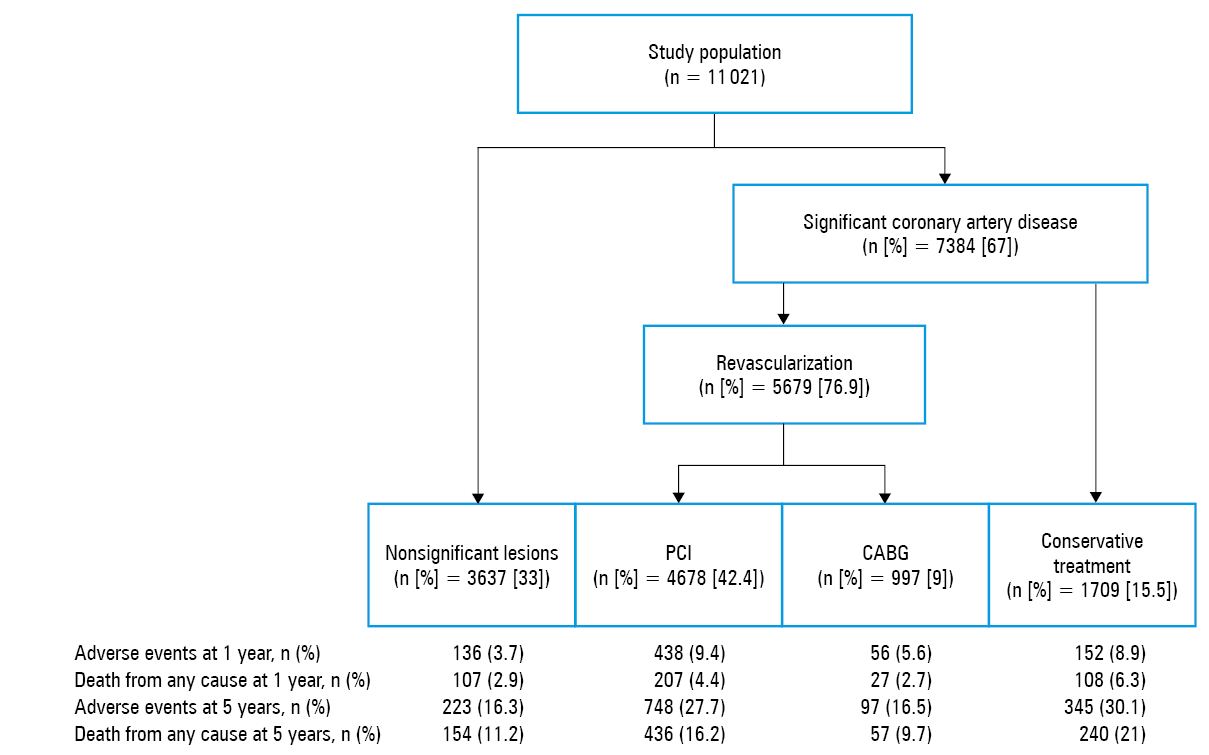
Abbreviations: CABG, coronary artery bypass grafting; PCI, percutaneous coronary intervention
Statistical analysis
The analysis included the descriptive statistics of baseline and angiographic characteristics, management, in‑hospital events, and the occurrence and predictors of adverse events at 1-, 3-, and 5‑year follow‑up. Continuous variables were expressed as mean (SD) for normally distributed variables or median (quartile 1 and 3) for nonnormally distributed variables. The normality of distribution was verified using the Shapiro–Wilk test. Categorical variables were presented as frequency. The 5‑year outcomes were summarized using the Kaplan–Meier method.
For all analyses, a 2‑tailed P value less than 0.05 was considered significant. The STATISTICA 13 software (StatSoft Inc., Tulsa, Oklahoma, United States) was used for all calculations.
Results
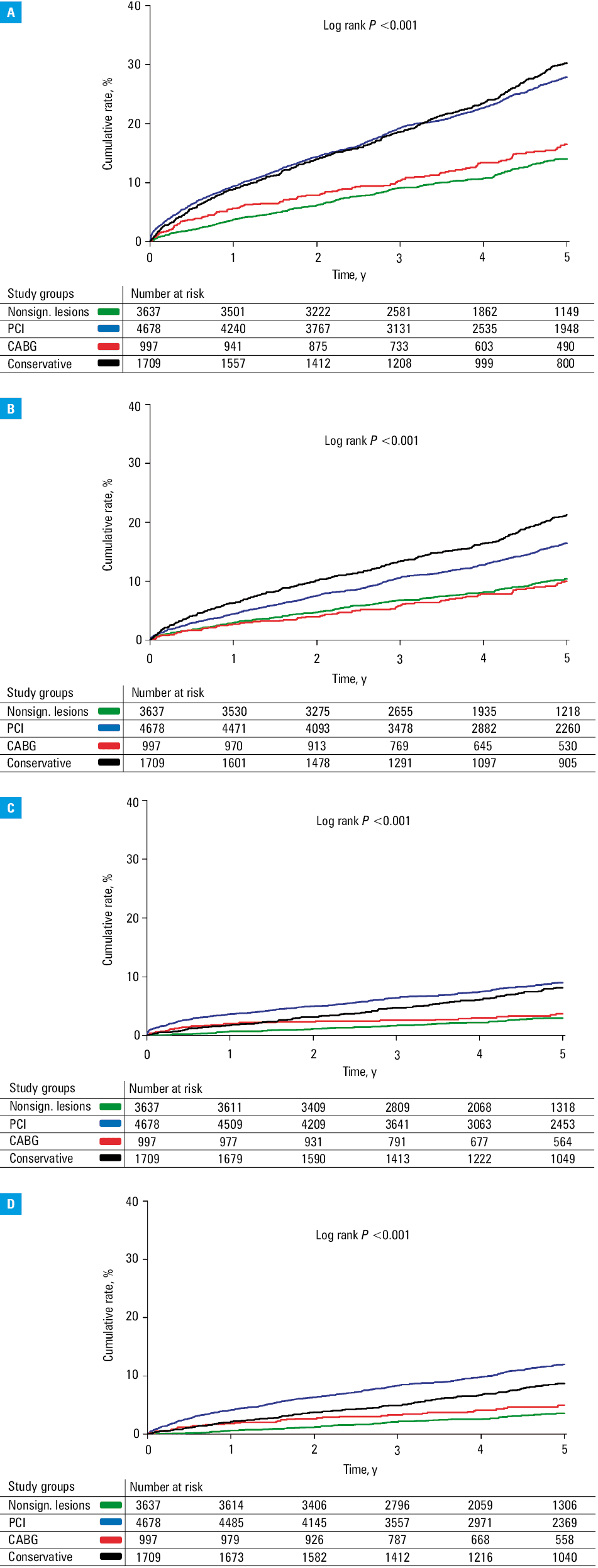
Between January 2006 and December 2016, 13 052 patients with confirmed CCS were enrolled into the PRESAGE registry. All patients were Caucasian. After the exclusion of those with significant valvular and neoplastic diseases, our study group included 11 021 patients. The nonsignificant lesion, PCI, CABG, and conservative treatment groups included 3637 (33%), 4678 (42.4%), 997 (9%), and 1709 (15.5%) patients, respectively. The baseline demographic, clinical, and angiographic characteristics of the study population are shown in Table 1. The mean (SD) age of the entire study cohort was 64.6 (9.4) years, and women constituted 35% of the subjects. Patients from the conservative treatment group were the oldest ones, with the highest prevalence of previous MI, CABG, diabetes, chronic total occlusion, and left ventricular ejection fraction below 35%. Pharmacotherapy recommended at discharge followed the ESC guidelines (Table 2). A total of 90% of the study patients received acetylsalicylic acid, and over 90% were treated with lipid‑lowering drugs (predominantly statins). Over 90% of the patients received β-blockers and nearly 90%—angiotensin‑converting enzyme inhibitors. In‑hospital and follow‑up data are presented in Table 3. The median (quartile 1 and 3)follow‑up was 1881 (1287–2907) days. The in‑hospital mortality rate in the entire study cohort was 0.4%, while the 5‑year all‑cause mortality rate was 15.3%. Five‑year mortality in nonsignificant lesion, PCI, CABG, and conservative treatment groups was 11.2%, 16.2%, 9.7%, and 21%, respectively. The Kaplan–Meier curves for all‑cause mortality, MI, ACS‑driven revascularization, and the total rates of adverse events are presented in Figure 2A–2D.
Variable | The PRESAGE registry | ||||||
Total population (n = 11 021) | Nonsignificant lesions (n = 3637) | Significant lesions | P value | ||||
PCI (n = 4678) | CABG (n = 997) | Conservative treatment (n = 1709) | |||||
Data are presented as percentage (number of patients affected / number of patients for whom data were available).
Abbreviations: BMI, body mass index; CABG, coronary artery bypass grafting; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; FFR, fractional flow reserve; GFR, glomerular filtration rate; LVEF, left ventricular ejection fraction; MI, myocardial infarction; Q1, quartile 1; Q3, quartile 3; others, see Figure 1 | |||||||
Age, y, mean (SD) | 64.6 (9.5) | 64 (9.7) | 65 (9.5) | 64.2 (8.7) | 64.9 (9.3) | <0.001 | |
Female sex | 35
(3858/11 021) | 49.9 (1814/3637) | 29.3 (1369/4678) | 23.7 (236/997) | 25.7 (439/1709) | <0.001 | |
Prior MI | 37.3 (4016/10 757) | 18.5
(647/3506) | 48.3 (2218/4592) | 31.6 (308/974) | 50 (843/1685) | <0.001 | |
Prior PCI | 35.4 (3806/10 757) | 20.5
(720/3506) | 47.5 (2182/4592) | 24.2 (236/974) | 39.6 (668/1685) | <0.001 | |
Prior CABG | 11.9 (1284/10 773) | 1.5
(53/3506) | 14.8 (683/4601) | 1.1 (11/976) | 31.8 (537/1690) | <0.001 | |
Prior stroke | 5.7 (614/10 796) | 4.2 (148/3515) | 6.2 (284/4606) | 5.8 (57/985) | 7.4 (125/1690) | <0.001 | |
Peripheral artery disease | 14.9 (1597/10 722) | 8.9
(311/3491) | 16 (733/4574) | 19.2 (187/976) | 21.8 (366/1681) | <0.001 | |
Atrial fibrillation | 17.7 (1905/10 759) | 23.7
(836/3528) | 14.5 (665/4578) | 9.1 (89/975) | 18.8 (315/1678) | <0.001 | |
Arterial hypertension | 81.3 (8888/10 927) | 81
(2905/3586) | 81.5 (3784/4645) | 83.2 (827/994) | 80.6 (1372/1702) | 0.37 | |
Family history of premature CAD | 20.2 (2137/10 556) | 21.7
(753/3465) | 19.3 (872/4528) | 19.7 (177/899) | 20.1 (335/1664) | 0.053 | |
Diabetes | 35.3 (3800/10 766) | 28.2
(986/3501) | 38.5 (1772/4599) | 37 (363/982) | 40.3 (679/1684) | <0.001 | |
Hypercholesterolemia | 75.6 (8177/10 813) | 71.4 (2525/3537) | 78.1 (3592/4602) | 77.8 (767/986) | 76.6 (1293/1688) | <0.001 | |
History of smoking | 46.9 (5048/10 774) | 42.3 (1483/3510) | 48.5 (2229/4596) | 49 (481/981) | 50.7 (855/1687) | <0.001 | |
Current smoking status | 22.7 (2447/10 774) | 22.4
(786/3510) | 23.7 (1089/4596) | 23 (226/981) | 20.5 (346/1687) | 0.06 | |
COPD | 6.2 (665/10 688) | 6 (209/3484) | 6.2 (282/4557) | 4.9 (48/976) | 7.5 (126/1671) | 0.04 | |
Canadian Cardiovascular Society class on admission | Asymptomatic / I | 41.5 (4358/10 492) | 42.1 (1422/3377) | 40.6 (1827/4506) | 34.8 (337/968) | 47 (772/1641) | <0.001 |
II | 35.1 (3679/10 492) | 34.6 (1168/3377) | 35.3 (1591/4506) | 42.8 (414/968) | 30.8 (506/1641) | <0.001 | |
III class | 23.4 (2455/10 492) | 23.3
(787/3377) | 24.1 (1088/4506) | 22.4 (217/968) | 22.1 (363/1641) | 0.08 | |
LVEF <35% | 12.5
(1159/9269) | 11.5
(270/2748) | 11.5 (475/4134) | 4.9 (42/865) | 24.4 (372/1522) | <0.001 | |
BMI, kg/m2, median (Q1–Q3) | 28 (26–31) | 28 (26–32) | 28 (26–31) | 28 (26–31) | 28 (25–31) | 0.09 | |
GFR <60 ml/min/1.73 m2 | 16.1 (1768/10 990) | 14.2
(514/3622) | 17.6 (821/4669) | 11.3 (113/996) | 18.8 (320/1703) | <0.001 | |
FFR measurement | 3.6 (401/11 021) | 3.1 (111/3637) | 3.7 (173/4678) | 5.7 (57/997) | 3.5 (60/1709) | 0.001 | |
Multivessel CAD | 36.9 (4071/11 021) | 0
(0/3637) | 51.5 (2409/4678) | 93.7 (934/997) | 42.6 (728/1709) | <0.001 | |
Left main CAD | 6.1
(668/11 021) | 0
(0/3637) | 6.7 (314/4678) | 18.2 (181/997) | 10.1 (173/1709) | <0.001 | |
Chronic total occlusion | 27.9 (3077/11 021) | 0
(0/3637) | 31.1 (1454/4678) | 50.6 (504/997) | 65.5 (1119/1709) | <0.001 | |
Drug | The PRESAGE registry | |||||
Total population (n = 11 021) | Nonsignificant lesions (n = 3637) | Significant lesions | P value | |||
PCI (n = 4678) | CABG (n = 997) | Conservative treatment (n = 1709) | ||||
Data are presented as percentage (number of patients affected / number of patients for whom data were available).
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin II receptor blocker; others, see Table 1 | ||||||
Acetylsalicylic acid | 90.0 (8767/9754) | 78.1 (2249/2879) | 97.4 (4271/4384) | 93.7 (848/905) | 88.2 (1399/1586) | <0.001 |
P2Y12 receptor inhibitor | 49.7 (4847/9754) | 7.7 (222/2879) | 98 (4297/4384) | 13.5 (122/905) | 13 (206/1586) | <0.001 |
Oral anticoagulation | 16.6 (1621/9754) | 21.5 (619/2879) | 14.2 (623/4384) | 8.4 (76/905) | 19.1 (303/1586) | <0.001 |
Nitrate | 40.5 (3954/9754) | 31.2 (899/2879) | 39.9 (1750/4384) | 54 (489/905) | 51.5 (816/1586) | <0.001 |
β-Blocker | 93.3 (9103/9754) | 90.2 (2596/2879) | 94.9 (4160/4384) | 92.9 (841/905) | 95 (1506/1586) | <0.001 |
ACEI / ARB | 87.4 (8528/9754) | 82.9 (2387/2879) | 90 (3947/4384) | 87.2 (789/905) | 88.6 (1405/1586) | <0.001 |
Aldosterone antagonist | 33.8 (3234/9555) | 26.8 (758/2832) | 40.2 (1726/4294) | 19.6 (173/883) | 37.3 (577/1546) | <0.001 |
Statin | 89.2 (8598/9640) | 82.2 (2343/2850) | 92.8 (4017/4329) | 91.6 (820/895) | 90.5 (1418/1566) | <0.001 |
Diuretic | 48.5 (4734/9754) | 45.9 (1321/2879) | 48.5 (2126/4384) | 39.8 (360/905) | 58.4 (927/1586) | <0.001 |
Proton pump inhibitors | 46 (4490/9754) | 33 (949/2879) | 60.8 (2666/4384) | 33.6 (304/905) | 36 (571/1586) | <0.001 |
Variable | The PRESAGE registry | |||||
Total population (n = 11 021) | Nonsignificant lesions (n = 3637) | Significant lesions | P value | |||
PCI (n = 4678) | CABG (n = 997) | Conservative treatment (n = 1709) | ||||
Data are presented as percentage (number of patients affected / number of patients for whom data were available).
| ||||||
In‑hospital outcomes | ||||||
Death from any cause | 0.4 (47/11 021) | 0.4 (15/3637) | 0.4 (19/4678) | 0.3 (3/997) | 0.6 (10/1709) | 0.31 |
MI | 0.3 (28/11 021) | 0 (1/3637) | 0.6 (26/4678) | 0 (0/997) | 0.1 (1/1709) | <0.001 |
Target vessel revascularization | 0.1 (14/11 021) | 0 (0/3637) | 0.3 (14/4678) | 0 (0/997) | 0 (0/1709) | <0.001 |
Stroke | 0.1 (6/11 021) | 0 (0/3637) | 0.1 (4/4678) | 0.2 (2/997) | 0 (0/1709) | 0.032 |
Major bleeding | 0.6 (63/11 021) | 0.2 (8/3637) | 0.9 (42/4678) | 0.6 (6/997) | 0.4 (7/1709) | <0.001 |
Adverse events at 1‑year follow‑up | ||||||
Any | 7.1 (782/11 021) | 3.7 (136/3637) | 9.4 (438/4678) | 5.6 (56/997) | 8.9 (152/1709) | <0.001 |
Death from any cause | 4.1 (449/11 021) | 2.9 (107/3637) | 4.4 (207/4678) | 2.7 (27/997) | 6.3 (108/1709) | <0.001 |
MI | 2.2 (245/11 021) | 0.7 (26/3637) | 3.6 (169/4678) | 2 (20/997) | 1.8 (30/1709) | <0.001 |
ACS‑driven revascularization | 2.4 (270/11 021) | 0.5 (23/3637) | 4.1 (193/4678) | 1.8 (18/997) | 2.1 (36/1709) | <0.001 |
Stroke | 0.9 (97/11 021) | 0.6 (23/3637) | 1.0 (47/4678) | 0.9 (9/997) | 1.1 (18/1709) | 0.26 |
Adverse events at 3‑year follow‑up | ||||||
Any | 15.5 (1408/9061) | 9.9 (282/2863) | 19.6 (765/3896) | 9.8 (80/813) | 18.9 (281) | <0.001 |
Death from any cause | 9.6 (869/9061) | 7.3 (208/2863) | 10.7 (418/3896) | 5.4 (44/813) | 13.4 (199/1489) | <0.001 |
MI | 4.5 (407/9061) | 1.9 (54/2863) | 6.5 (255/3896) | 2.7 (22/813) | 5.1 (76/1489) | <0.001 |
ACS‑driven revascularization | 2.4 (219/9061) | 2.3 (67/2863) | 8.7 (339/3896) | 3.2 (26/813) | 5.2 (77/1489) | <0.001 |
Stroke | 5.6 (509/9061) | 1.9 (55/2863) | 2.7 (106/3896) | 2.1 (17/813) | 2.8 (41/1489) | 0.13 |
Adverse events at 5‑year follow‑up | ||||||
Any | 26.3 (1542/5800) | 16.3 (223/1372) | 27.7 (748/2696) | 16.5 (97/587) | 30.1 (345/1145) | <0.001 |
Death from any cause | 15.3 (887/5800) | 11.2 (154/1372) | 16.2 (436/2696) | 9.7 (57/587) | 21 (240/1145) | <0.001 |
MI | 7.2 (417/5800) | 3.9 (54/1372) | 9 (243/2696) | 4.1 (24/587) | 8.4 (96/1145) | <0.001 |
ACS‑driven revascularization | 4.1 (237/5800) | 4.8 (66/1372) | 12.1 (327/2696) | 4.9 (29/587) | 9.2 (105/1145) | <0.001 |
Stroke | 9.1 (527/5800) | 3.4 (47/1372) | 4.3 (117/2696) | 2.2 (13/587) | 5.2 (60/1145) | 0.011 |
Abbreviations: see Figure 1
Discussion
Registries of stable angina
Both inclusion criteria and baseline characteristics differ in registries concerning patients with CCS.5-11,13 Outpatients referred to a cardiologist because of de novo CCS were enrolled in the Euro Heart Survey (EHS) of Stable Angina. The analysis involved 3779 patients from 36 European countries, enrolled in 2002.6 The inclusion criteria in the CLARIFY (Prospective Observational Longitudinal Registry of Patients with Stable Coronary Artery Disease) study included previous MI, evidence of coronary stenosis >50%, confirmed symptomatic myocardial ischemia, or a prior revascularization procedure. The study involved 32 703 outpatients from 45 countries and 5 continents, recruited in the years 2009 and 2010.8 The CICD (Chronic Ischemic Cardiovascular Disease) pilot registry included 755 patients with non–ST‑segment elevation acute coronary syndrome, 1464 with chronic CAD, and 201 with peripheral artery disease treated in 10 European countries between 2013 and 2014.7 The REACH (Reduction of Atherothrombosis for Continued Health) study was an outpatient registry of 68 236 patients with either stable symptomatic vascular disease (CAD, cerebrovascular disease, or peripheral artery disease) or multiple atherosclerotic risk factors, enrolled in 44 countries in the years 2003 and 2004.9
Baseline characteristics
While the inclusion criteria in the abovementioned registries differed from those set in the PRESAGE study, some similarities and differences can be observed between the studies in terms of patient enrolment, clinical characteristics, management, and treatment. Most of these registries enrolled ambulatory patients.5,6,8,9 The mean age of our study patients was 64.6 years—similar to the CLARIFY registry (64.2 years) and the CICD pilot registry (66.6 years) but higher than in the EHS study (61 years).6,7,9,10 Similar to our study, the majority of individuals in all other reports were male—from 58% in the EHS study to 77.6% in the CLARIFY registry.6,8 Hypertension was the most frequent risk factor in the majority of CCS registries and was observed in 62% of the patients from the EHS study and in 82.6% of those from the CICD pilot registry.6,7 Dyslipidemia was the second most frequent risk factor observed in 58% of the EHS patients and in 75.5% of the REACH patients.6,9
In our study, the presence of chronic occlusion of the coronary arteries was most frequent in the CABG (50.6%) and conservative treatment (65.5%) groups. This is in line with the data from previous studies, in which the presence of anatomical restrictions accounted for the more frequent choice of a conservative treatment strategy or CABG.19,20 Of note, PCI is beneficial for patients with angina resistant to optimal medical therapy or with a large area of ischemia within the chronic total occlusion–supplied territory.21 Therefore, conducting complete revascularization in this population leads to measurable benefits at long‑term follow‑up.22
Uniqueness of the PRESAGE registry
The main difference, as well as the largest advantage of PRESAGE over other registries, was observed in terms of diagnostic workup. Every patient enrolled in our study had coronary angiography performed, and nearly 85% of individuals underwent echocardiography. Of note, our study patients were enrolled in the years 2006 to 2016, a period of time in which indications for echocardiographic examination were less evident. The evaluation of left ventricular (LV) function by echocardiography has been recommended by the ESC guidelines since 2013 in all patients with CCS in order to identify LV abnormalities, measure the ejection fraction, and evaluate the diastolic function.16 Among other registries, the highest percentage of echocardiography performance was reported in 70% of the patients from the CICD pilot study, enrolled in the years 2013 and 2014.7 The percentage of patients in whom computed tomography coronary angiography, dobutamine stress echocardiography, or myocardial perfusion scintigraphy were performed was marginal, so these tests were not included in the analysis.
The PRESAGE registry presents the modalities for diagnostic workup and treatment offered to consecutive patients with CCS treated in a highly specialized cardiovascular center, in which the majority of diagnostic and therapeutic options can be used.13 To the best of our knowledge, PRESAGE is the first and largest registry to assess the complete clinical, angiographic, and therapeutic data in an all‑comer CCS population in a tertiary cardiology center.
Compared with other registries,5-11 the rate of evidence‑based medication use was high in the PRESAGE population, which reflects adherence to the ESC guidelines and the heterogeneity of our population. Of note, 35.4% of our study patients had a history of PCI, 42.4% during the index hospitalization; therefore, the high percentage of patients treated with β-blockers, angiotensin‑converting enzyme inhibitors, statins, and dual antiplatelet therapy seems to be apparent.
Long‑term outcomes
Long‑term mortality and cardiac event rates in patients with CCS vary among registries, depending mainly on patient characteristics and enrolment criteria. In the ESC pilot registry, 2.6% of the patients died during the 6‑month follow‑up period.23 In the REACH registry, the total mortality rate was 2.8% per year in the subgroup of patients with established cerebrovascular disease.9 Parma et al24 compared the long‑term outcomes of the Polish and European populations enrolled in the CLARIFY registry. The 5‑year all‑cause death rate in the Polish and European patients was 8.5% and 7.9%, respectively. The 5‑year mortality in the entire population of the PRESAGE registry was 15.3%. Importantly, 47.3% of our patients underwent revascularization procedures prior to index hospitalization, 37.3% had previous MI, and coronary angiography detected multivessel CAD in 36.9% of the patients.
Our registry confirms the observation that the population of patients with CCS is heterogeneous with regard to clinical characteristics, management, and outcomes. The worst clinical characteristics and long‑term prognosis were observed in patients with significant lesions of the coronary arteries who were deemed ineligible for any revascularization procedures by the Heart Team. Nearly a quarter of them had LV ejection fraction below 35%, nearly 1/3 of them underwent CABG, and nearly 2/3 of them presented with the chronic total occlusion of the coronary artery. Due to the wide variability of patient clinical and angiographic characteristics and the resulting different management strategies, we consciously resigned from performing multivariable analysis.
In our view, this analysis may be burdened with a significant methodological error, as a patient with nonsignificant lesions was not considered for revascularization. Therefore, we cannot directly relate our results to those obtained in the COURAGE trial25 and relevant meta‑analyses26,27 showing that revascularization in patients with CCS is an adjunctive treatment to optimal medical therapy. Similar conclusions were drawn in the recently published randomized ISCHEMIA trial (2588 patients assigned to invasive diagnostic workup and revascularization, and the remaining 2591 patients, to the control group).28 After 5 years of follow‑up (median follow‑up, 3.2 years), there was no significant difference in the risk of the key primary outcome (a composite of death from cardiovascular causes, MI, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest) and key secondary outcome (death from cardiovascular causes or MI).
Patients without significant lesions visualized on coronary angiography required closer attention. This generally poorly defined subpopulation should not be neglected, particularly due to the fact that the 5‑year mortality rate in our study was 11.2%. Although the mortality rate in this group compared with patients after PCI or CABG seems to be relatively high, patients without significant lesions frequently had previous MI or PCI and were diabetic. Moreover, noncardiovascular deaths in patients with CCS are still an underestimated problem.
Our analysis confirmed the role of coronary angiography in the management and treatment of patients with CCS. A coronary angiogram enabled us to assess the risk of cardiac events and implement appropriate treatment including revascularization. It was associated with a low rate of periprocedural complications. Such management seems to comply with the ESC recommendations, in which indications for coronary angiography in patients with CCS have been broadened.29
Limitations
In addition to the typical limitations associated with the retrospective design, several limitations need to be considered in the present study. First, the rate of fractional flow reserve measurement was relatively low, mainly due to the study period during which this modality was not commonly available in Poland. Second, the SYNTAX score values were unavailable, which precluded the full assessment of CAD severity in the study groups. Third, data on the completeness of revascularization were unavailable.
Conclusions
The PRESAGE registry provides valuable information on the clinical characteristics and long‑term outcomes of patients with CCS. The population of CCS patients and their long‑term prognosis is heterogeneous, and the poorest characteristics and outcomes were observed in those with significant lesions and deemed ineligible for revascularization procedures.
- Hemingway H, McCallum A, Shipley M, et al. Incidence and prognostic implications of stable angina pectoris among women and men. JAMA. 2006; 295: 1404‑1411. | Crossref
- Tunstall‑Pedoe H, Kuulasmaa K, Mähönen M, et al. Contribution of trends in survival and coronary‑event rates to changes in coronary heart disease mortality: 10‑year results from 37 WHO MONICA project populations. Monitoring trends and determinants in cardiovascular disease. Lancet. 1999; 353: 1547‑1557. | Crossref
- Piwońska A, Piotrowski W, Piwoński J, et al. Cardiovascular health knowledge of the Polish population. Comparison of two national multi‑centre health surveys: WOBASZ and WOBASZ II. Kardiol Pol. 2017; 75: 711‑719. | Crossref
- Pikala M, Maniecka‑Bryła I. Fifteen‑year mortality trends due to cardiovascular diseases in Poland using standard expected years of life lost, 2000–2014. Kardiol Pol. 2017; 75: 1033‑1040. | Crossref
- Steg PG, Greenlaw N, Tendera M, et al; Prospective Observational Longitudinal Registry of Patients With Stable Coronary Artery Disease (CLARIFY) Investigators. Prevalence of anginal symptoms and myocardial ischemia and their effect on clinical outcomes in outpatients with stable coronary artery disease: data from the international observational CLARIFY Registry. JAMA Intern Med. 2014; 174: 1651‑1659. | Crossref
ARTICLE INFORMATION