Numerous, disseminated, purplish skin nodules in a patient with chronic lymphocytic leukemia



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Numerous, disseminated, purplish skin nodules in a patient with chronic lymphocytic leukemia
A 65‑year‑old woman diagnosed with chronic lymphocytic leukemia and chronic hepatitis B virus infection was consulted in an outpatient dermatology department due to numerous, disseminated, purplish skin nodules that had appeared during treatment with ibrutinib (Figure 1A and 1B). The patient was previously empirically treated with doxycycline (100 mg twice daily for 11 days) with partial improvement, but, after cessation of drug use, the progression of symptoms was observed and elevated body temperature was noted. She was also taking lamivudine, acyclovir, allopurinol, ethamsylate, folic acid, and vitamin D3. Ibrutinib treatment was discontinued. Dermoscopically, the nodules presented a pattern of linear vessels with branches, white‑pinkish structureless areas, and a brownish peripheral structureless area (Figure 1C and 1D). At the time of consultation, blood tests showed a white blood cell count of 56.91 × 109/l (reference range, 4–10 × 109/l; 0.5% of monocytes, basophils, and eosinophils, 5.1% of segments, 72.8% of lymphocytes, and 20.5% of lymphoid cells), red blood cell count of 3.02 × 1012/l (reference range, 3.8–4.8 × 1012/l), mean corpuscular volume of 104.6 fl (reference range, 80–96 fl), mean corpuscular hemoglobin of 36.1 pg (reference range, 27–32 pg), hemoglobin level of 109 g/l (reference range, 120–150 g/l), and platelet count of 33 × 109/l (reference range, 150–410 × 109/l). Histological examination confirmed the diagnosis of bacillary angiomatosis (BA) (Figure 1E and 1F). Treatment with clarithromycin was recommended, but after 14 days of drug intake lesions became severely ulcerated and fever recurred (the Jarisch–Herxheimer reaction). After a consultation with an infectious disease specialist, doxycycline treatment (100 mg twice daily for 6 weeks) was introduced instead, leading to complete resolution of skin lesions and alleviation of the Jarisch–Herxheimer reaction symptoms.
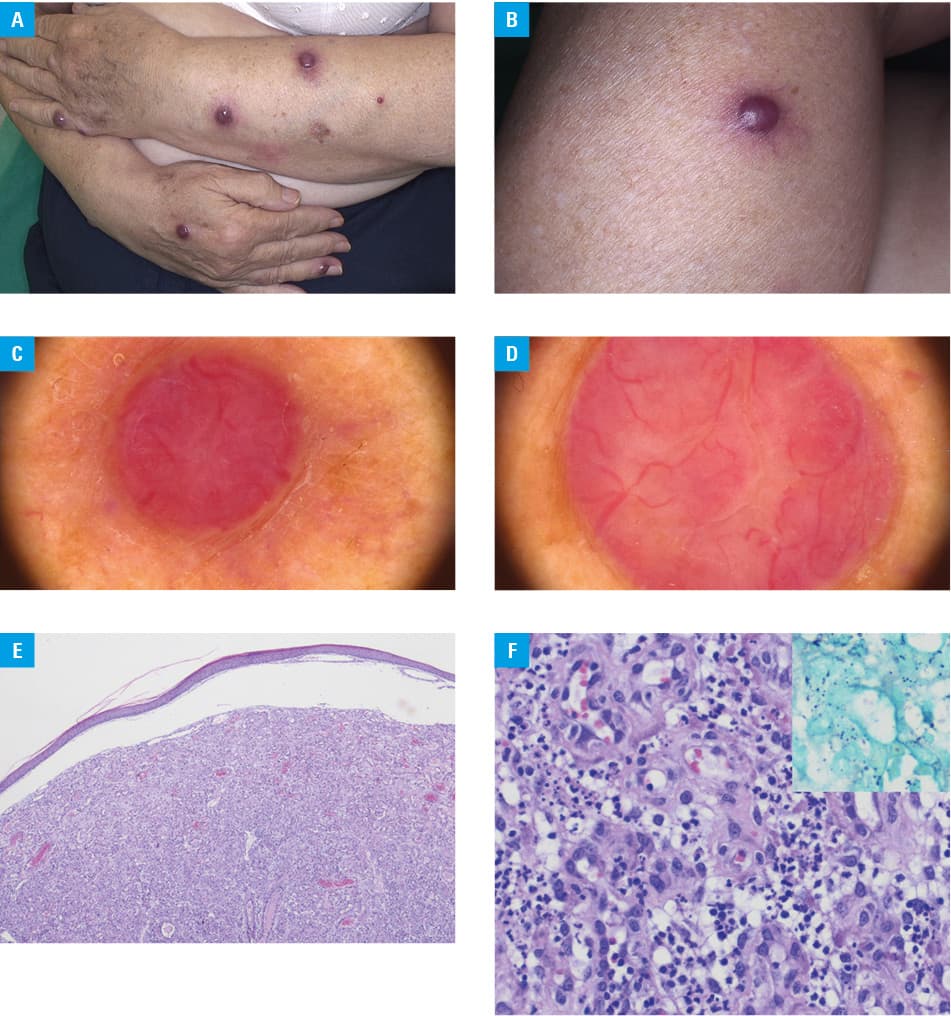
Bacillary angiomatosis is a relatively rare disease caused by Bartonella henselae (B. henselae) or Bartonella quintana (B. quintana). Its most common manifestations include red‑purplish skin plaques or nodules, which may be associated with internal organ involvement.1 Transmission results from cat scratches or bites contaminated with infested cat flea feces (B. henselae) or from an infested human body louse that spreads the infection between people (B. quintana). Bacillary angiomatosis is usually observed in immunocompromised patients with human immunodeficiency virus or hepatitis B virus infection, in the course of leukemia or during chemotherapy, but it occasionally also affects immunocompetent individuals.1 Bacillary angiomatosis most commonly involves the skin, but almost every organ may be affected. A cutaneous BA lesion presents as a vascular, firm, and sometimes tender plaque or tumor. The lesions may differ in size and number and occur as a result of stimulation of proliferation and migration of endothelial cells caused by the bacteria.1 The differential diagnosis of BA includes a wide range of vascular tumors, eg, Kaposi sarcoma, pyogenic granuloma, angiosarcoma, angiokeratoma, and glomangioma, as well as cat‑scratch disease, verruga peruana, and angiolymphoid hyperplasia with eosinophilia.2-5 The dermoscopic presentation, interpreted in the clinical context, may be useful in the initial differentiation between these entities. To our knowledge, this is the first report on dermoscopic observations in BA. The observed linear vessels with branches correspond with vascular proliferations, while whitish structureless areas may correspond with amorphous aggregates that stain positively with the Warthin–Starry silver stain. A brownish peripheral structureless area may correspond with the bend of the epidermis due to the underlying vascular proliferation.
- Zarraga M, Rosen L, Herschthal D. Bacillary angiomatosis in an immunocompetent child: a case report and review of the literature. Am J Dermatopathol. 2011; 33: 513‑515. | Crossref
- Hu SC, Ke CL, Lee CH, et al. Dermoscopy of Kaposi’s sarcoma: areas exhibiting the multicoloured ‘rainbow pattern.’ J Eur Acad Dermatol Venereol. 2009; 23: 1128‑1132. | Crossref
- Zaballos P, Carulla M, Ozdemir F, et al. Dermoscopy of pyogenic granuloma: a morphological study. Br J Dermatol. 2010; 163: 1229‑1237. | Crossref
- Cozzani E, Chinazzo C, Ghigliotti G, et al. Cutaneous angiosarcoma: the role of dermoscopy to reduce the risk of a delayed diagnosis. Int J Dermatol. 2018; 57: 996‑997. | Crossref
- Rodríguez‑Lomba E, Avilés‑Izquierdo JA, Molina‑López I, et al. Dermoscopic features in 2 cases of angiolymphoid hyperplasia with eosinophilia. J Am Acad Dermatol. 2016; 75: e19‑e21. | Crossref
ARTICLE INFORMATION