Prevalent medication-related harm identified in patients admitted to a geriatric ward: cross-sectional and survival based contributors
Key words: elderly, iatrogenic geriatric syndromes, medication-related harm, survival



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Prevalent medication-related harm identified in patients admitted to a geriatric ward: cross-sectional and survival based contributors
Introduction: Medication‑related harm (MRH) has been recognized as a global public health issue.
Objectives: This study aimed to assess the prevalence and causes of MRH in geriatric patients. Another objective of the study was to recognize how MRH and drugs prescribed after geriatric interventions affect survival.
Patients and methods: It was a cross‑sectional study of 301 geriatric patients admitted to the hospital for any cause, combined with a 2‑year survival analysis. Altogether, 71 drug items were included. Medication‑related harm was defined based on clinical reasoning. Logistic regression models were applied to identify the explanatory variables for each type of MRH. The Cox proportional hazards model was used to determine the association of MRH and postdischarge medications with patient survival.
Results: Medication‑related harms were identified in 35.2% of the study patients. Those included, among others, hypotension (19.3%), hypoglycemia (13.3%), parkinsonism (4.3%), and benzodiazepine addiction (5.7%). Logistic regression, applied to estimate the impact of drugs before admission on MRH of any type, demonstrated an independent negative effect of typical neuroleptics, antidiabetic medication, benzodiazepines, and supplements, except vitamin D. After geriatric interventions, 4 drug classes showed a positive association with survival: thiazides (hazard ratio [HR], 0.45; 95% CI, 0.22–0.93), selective serotonin reuptake inhibitors (SSRIs; HR, 0.51; 95% CI, 0.34–0.75), paracetamol (HR, 0.54; 95% CI, 0.33–0.88), and angiotensin‑converting enzyme inhibitors (ACEIs; HR, 0.59; 95% CI, 0.4–0.89).
Conclusions: Geriatric‑based deprescribing and drug optimization mitigate the negative impacts of MRH on patient survival and may decrease the rehospitalization rate and healthcare costs. Thiazides, ACEIs, SSRIs, and paracetamol, if indicated, were associated with better survival in geriatric patients.
What's new?
This study shows the most prevalent medication‑related harm (MRH) types in geriatric inpatients from cross‑sectional and prospective perspectives. Drug‑related hypotension, hypoglycemia, parkinsonism, and benzodiazepine addiction represented the most common and overlapping MRHs. Drug‑induced parkinsonism was strongly related to the use of typical neuroleptics. Furthermore, only this type of MRH was associated with a lower survival rate despite the discontinuation of antidopaminergic drugs during hospital stay. The article highlights the complexity of MRH contributors that cover the qualitative (inappropriate treatment) and / or quantitative (overtreatment) issues, as well as the third player—patients’ conditions and susceptibility to MRH. Based on the Cox proportional hazards model, the study identified medications that showed a positive (angiotensin‑converting enzyme inhibitors, thiazides including indapamide, selective serotonin reuptake inhibitors, and paracetamol) or negative association (spironolactone or eplerenone) with an over 2‑year survival of patients after geriatric interventions. However, these associations may also be surrogates of disease severity that affects the survival of geriatric patients.
Introduction
A growing number of octogenarians coupled with multimorbidity have led to polypharmacy and the risk of drug- or dosage‑related problems, even in the case of properly selected medicines.1-3 All types of medication‑related harm (MRH) have been recognized by the World Health Organization as a global public health issue.4,5 The significance of MRH is rising and has become one of the main causes of hospital admission,6-8 even after recent discharge.9,10 Special strategies and criteria for avoiding MRH have been developed and regularly updated to mitigate drug‑induced problems, polypharmacy, and age‑related alterations in drug handling.11-13 Nevertheless, a recent meta‑analysis found no statistically significant positive effect from any intervention in primary care settings on the hospitalization rate.14 Compliance with specific criteria does not always protect against MRH, especially in comorbid and older adults suffering from frailty or cognitive impairment.15 Medication‑related harm results from improper or hasty medical reasoning, insufficient geriatric skills, rare medication reconciliation, or reviews.16
Polypharmacy and drug‑related problems do coexist and overlap. Hence, appropriate deprescribing has a potential to reduce adverse drug reactions and costs as well as to improve patients’ quality of life.17,18 Iatrogenesis, like MRH, was added to the main pillars of Isaacs’ “geriatric giants.”4 However, how many faces does MRH have? An iatrogenic illness in frail older adults may appear unusual and can be masked by another diseases or disorders. Even “appropriate” medicines administered according to an inappropriate dosage can have unexpected negative effects in the frail elderly.4
Most studies have focused on risk factors for MRH in elderly people, including polypharmacy, inappropriate prescribing, as well as differences in pharmacokinetics and pharmacodynamics at old age. They have also looked at treatment provided by numerous physicians and a decreased capacity to handle medication or MRH following discharge from a hospital.19-21 Relatively little is known about the common types of MRH and their long‑term consequences. The questions addressed in this article include the following: What are the most prevalent faces of MRH in real‑life geriatrics? What contributors are involved? Medication‑related harm, such as, among others, drug‑induced hypoglycemia, hypotension, benzodiazepine addiction, and parkinsonism, overlap with each other and superimpose themselves on chronic conditions. Furthermore, this study aimed to show the associations between MRH and drugs prescribed at discharge during a survival period longer than 2 years.
Patients and methods
It was a cross‑sectional study of geriatric inpatients, combined with an analysis of an over 2‑year survival after geriatric hospital interventions. The study was complementary to the results of a previous work focused on the quantitative aspects of polypharmacy before and after hospital stay.18 A geriatric intervention included a thorough change in medication use (deprescribing and new prescribing) to adjust treatment to individual patient needs. Postdischarge drug recommendations were continued in a geriatric outpatient clinic where patients were referred after hospitalization.
All 301 consecutive patients (mean [SD] age, 82.3 [6.7] years) underwent a comprehensive geriatric assessment along with an extensive clinical examination and careful reasoning to establish the final diagnoses, including the analysis of possible MRH. Discharge dates ranged between January and June 2017. Death dates were obtained from the Polish Ministry of Digital Affairs on the censoring date of March 3, 2020. The median (interquartile range) survival was 34.7 (23.6–37.23) months (mean [SD], 29.4 [11.7] months).
Data on medication use before hospital stay and after discharge were also collected. Each medication was assigned to the relevant category out of 71 drug classes defined in Supplementary material, Table S1, both at admission (taken before hospitalization) and at hospital discharge (recommended to use after geriatric interventions). We did not record the medication dose. The rationale for medication use during hospital stay was revised based on the Beers,22 STOPP (Screening Tool of Older Persons’ potentially inappropriate Prescriptions), and START (Screening Tool to Alert doctors to the Right Treatment) criteria.12
Dependent variables
The following types of MRH were defined: 1) drug‑induced hypotension: low values of systolic (<90 mm Hg) or diastolic (<60 mm Hg) blood pressure (BP) or orthostatic hypotension, accompanied by dizziness, fainting, or neurological symptoms in patients receiving antihypertensive therapy; 2) drug‑induced hypoglycemia: documented episodes of low glycemia (<70 mg/dl) in patients on antidiabetic treatment; 3) benzodiazepine addiction with fall(s); 4) drug‑induced parkinsonism (stiffness, rigidity, shuffling gait, and other extrapyramidal signs) linked to the antidopaminergic activity of typical neuroleptics; 5) others: drug- or dosage‑related disorders (gastrointestinal bleeding or ulcers, anemia, cognitive impairment, heart failure exacerbation, drug‑induced hypertension, bradycardia, inanition, hypothyroidism following amiodarone therapy, and electrolyte disorders). The use of the study patients’ data was approved by an ethics committee and complied with the Declaration of Helsinki.
Inpatient characteristics as potential explanatory factors
The characteristics of the study patients included sociodemographic data, anthropometric data, and health‑related variables on admission including weakness, dizziness, fainting, pain, laboratory findings, mean arterial pressure (MAP) in supine and vertical positions calculated according to the following formula: diastolic BP + 1/3 (systolic BP – diastolic BP),23 orthostatic hypotension (a drop of 20 mm Hg or greater in systolic BP or of 10 mm Hg or greater in diastolic BP between measurements taken in supine and vertical positions within 1 to 3 minutes), and pulse pressure (PP) as a difference between systolic and diastolic BP in supine and vertical positions just after standing up.24 The change in the PP values between standing and supine positions was recorded. The functional level was assessed using the Barthel Index,25 the 15‑item Geriatric Depression Scale,26 and the Mini‑Mental State Examination.27 Additionally, a list of 21 diagnoses at discharge was established.
Statistical analysis
Data analyses were performed using Microsoft Excel and the Statistica software, version 12.0 (StatSoft Polska, Kraków, Poland). The formula for the Wilson score interval was applied when calculating 95% CIs for a proportion of MRH types. The χ2 test was used to assess the significance of differences among categorical variables. The nonparametric Mann–Whitney test was used to verify the significance of differences among continuous variables. Multivariable logistic regressions were applied to identify significant explanatory variables for the conditional probability regarding MRH of any type and each of the most prevalent types of MRH. The explanatory variables that turned out to be nonsignificant were omitted. All logistic regressions were controlled for age and multimorbidity expressed by the number of diseases out of 21 defined. The Cox proportional hazards model was applied to evaluate the association between MRH types and survival as well as between medication classes and survival. A P value less than 0.05 was considered significant.
Results
The mean (SD) age of 301 inpatients was 82.4 (6.7) years, and women constituted 2/3 of the study cohort. Detailed characteristics are presented in Table 1. Most of the patients were highly comorbid, disabled, and polymedicated. One or more MRH types were identified in 35.2% of the patients (Table 2). The most frequent MRH was hypotension (19.3%), followed by drug‑induced hypoglycemia (13.3%) and benzodiazepine addiction with fall(s) (5.7%). Drug‑induced parkinsonism was found in 13 cases (4.3%). In 5 patients (2%), amiodarone‑related hyper- or hypothyroidism were found. Harm following nonsteroidal anti‑inflammatory drug use (anemia, gastric ulceration, or heart failure) was noted in 8 patients (3%). Other MRH types (n = 11 [3.7%]) included drug‑induced bradycardia, electrolyte disorders, inanition, or myopathy following statin therapy. Altogether, 153 cases of various MRH types were identified in 106 patients.
Characteristics | N (%) | Mean (SD) | Median (IQR) |
a Missing cases: 11
b Missing cases: 62
c Missing cases: 14
Abbreviations: COPD, chronic obstructive pulmonary disease; IADL, instrumental activity of daily living; MMSE, Mini‑Mental State Examination; PP, pulse pressure | |||
Female sex | 204 (67.8) | – | – |
Age, y | – | 82.4 (6.7) | 84 (80–86) |
Death | 107 (35.5) | – | – |
Survival, mo | – | 29.4 (11.7) | 34.7 (32.2–36.4) |
Education, y | – | 9.1 (4.1) | 9 (7–11) |
Residence place (urban) | 212 (70.4) | – | – |
Barthel Index (0–100) | – | 79.4 (25.4) | 90 (80–95) |
IADL (0–12) | – | 6.6 (3.9) | 7 (5–9) |
Geriatric Depression Scale (0–15)a | – | 6.1 (3.8) | 6 (4–8) |
MMSE (0–30)b | – | 20.6 (6.8) | 22 (18–25) |
PP in supine position, mm Hg | – | 63.3 (17.7) | 60 (54–70) |
PP in standing position, mm Hgc | – | 56.1 (18.2) | 55 (47–62) |
Ischemic heart disease | 194 (64.8) | – | – |
Hypertension | 198 (65.8) | – | – |
Atrial fibrillation | 76 (25.2) | – | – |
Heart failure | 72 (23.9) | – | – |
Cerebrovascular disease | 139 (64.1) | – | – |
Arthritis | 158 (52.5) | – | – |
Parkinson disease | 48 (15.9) | – | – |
Depression | 200 (66.4) | – | – |
Dementia | 125 (41.5) | – | – |
Delirium | 67 (22.6) | – | – |
Anemia | 123 (40.9) | – | – |
Diabetes | 116 (38.5) | – | – |
Infection | 92 (30.5) | – | – |
Liver disease | 74 (24.6) | – | – |
Chronic kidney disease | 50 (16.6) | – | – |
Ulcer | 65 (21.6) | – | – |
Thyroid disorder | 28 (9.3) | – | – |
Cancer | 29 (9.6) | – | – |
Benign prostatic hyperplasia | 37 (12.3) | – | – |
Connective tissue disease | 12 (4.0) | – | – |
COPD | 20 (6.6) | – | – |
Diseases out of 21 defined, n | – | 6.6 (2.3) | 6 (6–8) |
Medications on admission, n | – | 7.5 (3.4) | 7 (6–8) |
Medications at discharge, n | – | 6.2 (2.1) | 6 (5–7) |
Characteristics | N (%) | 95% CI | |
a In 106 patients affected by MRH
Abbreviations: MRH, medication‑related harm; NSAID, nonsteroidal anti‑inflammatory drug | |||
MRH of any type | 106 (35.2) | 30–40.8 | |
Drug‑induced hypotension | 58 (19.3) | 15.2–24.1 | |
Drug‑induced hypoglycemia | 40 (13.3) | 9.9–17.6 | |
Benzodiazepine addiction with fall(s) | 17 (5.7) | 3.6–8.9 | |
Drug‑induced parkinsonism | 13 (4.3) | 2.5–7.2 | |
NSAID‑related harm | 8 (3) | 1.4–5.2 | |
Amiodarone‑induced hyper- or hypothyroidism | 5 (1.7) | 0.7–3.8 | |
Harm induced by other drugs | 11 (3.7) | 2.1–6.4 | |
Number of coexisting MRH typesa | 1 | 65 (61.3) | 51.8–70 |
2 | 35 (33) | 24.8–42.4 | |
3 | 6 (5.7) | 2.6–11.8 | |
As shown in Table 3, regardless of the MRH type, patients affected by MRH more often complained of dizziness, syncope, fainting, or falls before admission to the hospital. They also suffered from significantly marked multimorbidity and polymedication. They had an almost 3‑fold higher value of PP change between the standing and supine body positions than patients unaffected by MRH. It resulted from a higher PP value in the supine position and a lower PP value after standing up as compared with the remaining patients.
Characteristics | Any MRH | P valuea | |
No (n = 106) | Yes (n = 195) | ||
a χ2 test or Mann–Whitney test as appropriate
b Missing cases: 62
c Missing cases: 11
d Missing cases: 14
| |||
Survival time, mo, median | 34.7 | 34.5 | 0.61 |
Age, y, mean (SD) | 82.4 (6.9) | 82.3 (6.3) | 0.86 |
Female sex, n (%) | 131 (67.2) | 73 (67.8) | 0.76 |
Living alone, n (%) | 57 (29.3) | 40 (37.7) | 0.13 |
Barthel Index (0–100), mean (SD) | 80.5 (25.5) | 77.4 (22.2) | 0.12 |
IADL (0–12), mean (SD) | 6.7 (3.9) | 6.4 (3.9) | 0.51 |
MMSE (0–30), mean (SD)b | 20.8 (7.1) | 20.3 (6.3) | 0.26 |
Geriatric Depression Scale (0–15), mean (SD)c | 5.6 (3.7) | 6.8 (3.8) | 0.03 |
Dizziness or vertigo on admission, n (%) | 79 (40.5) | 61 (57.6) | 0.004 |
Syncope or fainting before admission, n (%) | 18 (9.2) | 20 (18.9) | 0.01 |
Fall(s) during the preceding year, n (%) | 88 (45.1) | 79 (74.5) | <0.001 |
Orthostatic hypotension, n (%) | 42 (22.6) | 44 (43.6) | <0.001 |
MAP in supine position, mm Hg, mean (SD) | 88.2 (12.1) | 88.4 (11.1) | 0.47 |
MAP in standing position, mm Hg, mean (SD)d | 87.9 (12.9) | 85.1 (13.3) | 0.1 |
PP in supine position, mm Hg, mean (SD) | 62.0 (17.1) | 65.6 (18.8) | 0.1 |
PP in standing position, mm Hg, mean (SD)d | 57.7 (18.3) | 53.1 (17.6) | 0.03 |
PP change between standing and supine positions, mm Hg, mean (SD)d | –4.7 (14.5) | –12.9 (15.9) | <0.001 |
Diseases out of 21 defined, n, mean (SD) | 6.3 (2.3) | 7.1 (2.1) | 0.002 |
Ischemic heart disease, n (%) | 120 (61.5) | 74 (69.5) | 0.15 |
Hypertension, n (%) | 121 (62.1) | 77 (72.6) | 0.06 |
Atrial fibrillation, n (%) | 46 (23.6) | 30 (28.3) | 0.37 |
Heart failure, n (%) | 50 (25.6) | 22 (20.8) | 0.34 |
Cerebrovascular disease, n (%) | 121 (62.1) | 72 (67.9) | 0.31 |
Arthritis, n (%) | 105 (53.9) | 53 (50) | 0.52 |
Parkinson disease, n (%) | 26 (13.3) | 22 (20.7) | 0.09 |
Depression, n (%) | 122 (62.5) | 78 (73.6) | 0.05 |
Dementia, n (%) | 78 (40) | 47 (44.3) | 0.46 |
Delirium, n (%) | 40 (20.5) | 27 (25.5) | 0.32 |
Anemia, n (%) | 78 (40) | 45 (42.5) | 0.67 |
Diabetes, n (%) | 51 (26.2) | 65 (61.3) | <0.001 |
Infection, n (%) | 65 (33.3) | 27 (26) | 0.19 |
Liver disease, n (%) | 47 (24.1) | 27 (25.5) | 0.79 |
Chronic kidney disease, n (%) | 28 (14.4) | 22 (20.8) | 0.15 |
Ulcer, n (%) | 41 (21) | 24 (22.6) | 0.74 |
Thyroid disorder, n (%) | 20 (10.3) | 8 (7.6) | 0.45 |
Cancer, n (%) | 19 (9.7) | 10 (9.4) | 0.93 |
Benign prostatic hyperplasia, n (%) | 24 (37.5) | 13 (39.4) | 0.85 |
Connective tissue disease, n (%) | 9 (4.6) | 3 (2.9) | 0.44 |
COPD, n (%) | 14 (7.2) | 6 (5.7) | 0.61 |
Medications on admission, n, mean (SD) | 6.9 (3.3) | 8.7 (3.1) | <0.001 |
Medication‑related harm of any type
Multivariable logistic regression, applied to estimate the impact of drugs taken before admission on the occurrence of MRH of any type, documented the negative effect of typical neuroleptics (eg, haloperidol, promazine, sulpiride, and tiapride) (odds ratio [OR], 12; 95% CI, 3–47.4), antidiabetic medications (ie, sulfonylureas, metformin, or insulin) (OR, 7.7; 95% CI, 4–15), benzodiazepines (OR, 5.3; 95% CI, 2.3–12.3), supplements except vitamin D (OR, 2.1; 95% CI, 1.1–4), and the lower value of PP after standing up from a supine position (Table 4, model A).
Medications before admission; patient in‑hospital characteristics | Model A (medication‑related harm of any type) | Model B (drug‑induced hypotension) | Model C (drug‑induced hypoglycemia) | Model D (benzodiazepine addiction) | ||||||||||
OR | 95% CI | P value | OR | 95% CI | P value | OR | 95% CI | P value | OR | 95% CI | P value | |||
Abbreviations: see Table 1 | ||||||||||||||
Benzodiazepine use | 5.3 | 2.3–12.3 | <0.001 | 2.9 | 1.3–6.6 | 0.008 | – | – | – | – | – | – | ||
β-Blocker use | – | – | – | – | – | – | 2.5 | 1–6 | 0.045 | – | – | – | ||
Tramadol use | – | – | – | – | – | – | – | – | – | 4.6 | 1.5–13.9 | 0.006 | ||
Typical neuroleptics use | 12 | 3–47.4 | <0.001 | – | – | – | – | – | – | – | – | – | ||
Antidiabetic drug use | 7.7 | 4–15 | 0.001 | – | – | – | – | – | – | – | – | – | ||
Supplement use (except vitamin D) | 2.1 | 1.1–4 | 0.02 | 2.5 | 1.4–4.8 | 0.007 | – | – | – | – | – | – | ||
Drugs before hospital admission, n | – | – | – | – | – | – | – | – | – | 1.2 | 1–1.4 | 0.035 | ||
Diabetes | – | – | – | 3.3 | 1.7–6.6 | <0.001 | – | – | – | – | – | – | ||
PP in standing position, mm Hg | 0.97 | 0.96–0.99 | 0.006 | 0.97 | 0.94–0.98 | 0.001 | 1 | 0.98–1.02 | 0.62 | 0.95 | 0.92–0.99 | 0.01 | ||
Diseases (out of 21), n | 1.1 | 0.97–1.23 | 0.11 | 1 | 0.86–1.18 | 0.86 | 1.3 | 1.1–1.6 | <0.001 | 0.98 | 0.76–1.25 | 0.86 | ||
Age, y | 1 | 0.97–1.06 | 0.47 | 1 | 0.96–1.06 | 0.48 | 0.9 | 0.8–1 | 0.049 | 1.02 | 0.93–1.11 | 0.64 | ||
Drug‑induced hypotension
Drug‑induced hypotension was the most prevalent type of MRH and was found in almost every fifth patient receiving antihypertensive therapy. Drug‑induced hypotension was accompanied by drug‑induced hypoglycemia (33%), benzodiazepine addiction with fall(s) (21%), drug‑induced parkinsonism (5%), or other drug‑related problems (17%). Patients much more often complained of dizziness, fainting, and falls in the preceding year. In total, 77.2% of the patients presented with orthostatic hypotension. Multivariable logistic regression (Table 4, model B) showed the coexistence of diabetes, benzodiazepine use, supplement use, and a lower value of PP after standing up as factors independently contributing to the disorder.
Drug‑induced hypoglycemia
Drug‑induced hypoglycemia was identified in 13.3% of the study group and affected up to every third diabetic patient. The results of multivariable logistic regression revealed that multicomorbidity and β-blocker use contributed to this iatrogenic disorder (Table 4, model C), apart from antidiabetic treatment.
Benzodiazepine addiction
Benzodiazepine addiction was found in 5.7% of the study patients. Multivariable logistic regression showed 3 contributing factors: lower values of PP after standing up, a greater number of drugs taken before admission, and tramadol use (Table 4, model D).
Drug‑induced parkinsonism
Drug‑induced parkinsonism pertained to a relatively small number of patients affected by MRH (n = 13) and was identified mainly in those with significantly worse cognitive function and lower physical performance. Logistic regression explaining this disorder could not be properly estimated. Therefore, the only evident positive relationship was linked to the use of typical neuroleptics.
Impact of medication‑related harm on survival
Before discharge, medications used by patients were reconciled and adjusted to their individual needs, including withdrawal of potentially inappropriate drugs. Within a 2.4‑year follow‑up, 35.5% of the study patients died. After adjustment for age and multimorbidity, out of all defined MRH types, only drug‑induced parkinsonism was independently negatively associated with survival according to the Cox proportional hazards model (hazard ratio, 2.4; 95% CI, 1.25–4.61; P = 0.009).
Survival and medication use
Out of 71 drug items at discharge, 4 drug classes showed a positive association with survival, namely, selective serotonin reuptake inhibitors (SSRIs) (P = 0.001), thiazides including indapamide (P = 0.03), paracetamol (P = 0.01), and angiotensin‑converting enzyme inhibitors (ACEIs) (P = 0.01). The opposite, negative association was found in spironolactone or eplerenone users (P = 0.04). The remaining drugs—including statins, antidiabetics, vitamins and minerals, and even vitamin D—proved to be neutral for survival (Figure 1).
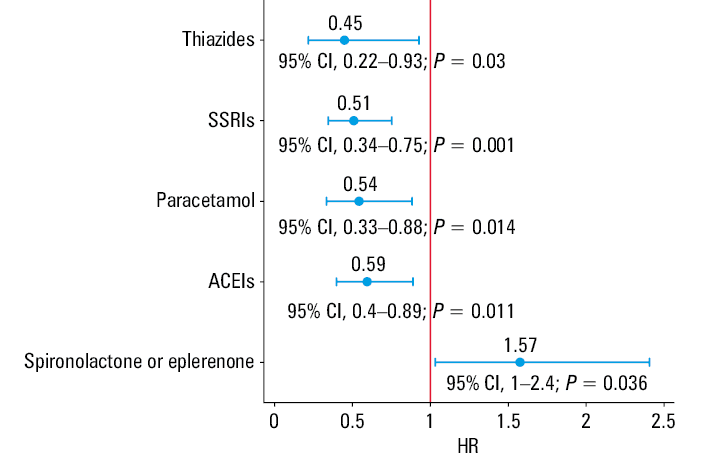
Abbreviations: ACEIs, angiotensin‑converting enzyme inhibitors; HR, hazard ratio; SSRIs, selective serotonin reuptake inhibitors
Discussion
Medication‑related harm is growing in importance among older adults, along with multimorbidity and polypharmacy.4,28 Age‑related impairments interplay with multifaceted health conditions and drug‑related outcomes, making clinical presentation blurred, ambiguous, and often wrongly diagnosed.29 A geriatric approach, looking beyond medicines, and deprescribing are the best ways to avoid MRH linked to inappropriate or redundant medication use.18
The rate of MRH noted in this study (35%) seems extremely high, though it is lower than 82% reported in an Ethiopian study,28 46.2% documented in a Brazilian study,30 and 39% in another study of hospitalized multimorbid older patients.31 Nevertheless, the incidence and prevalence of MRH in the elderly cannot be accurately determined owing to a huge diversity in the nomenclature and perception of the issue,32 as well as patients’ setting and age.33,34 It is estimated that 10% to 30% of older adults are admitted to the hospital because of MRH,7 although MRH is usually a hidden problem in a large proportion of patients, at least in the present study, being referred to the hospital for other reasons. After adjustment for age and multimorbidity, only typical neuroleptics, antidiabetics, benzodiazepines, and, interestingly, supplements (except vitamin D), as well as a higher value of PP change (after standing up) independently affected MRH of any origin. This finding allowed the researcher to assess the complexity of the MRH nature that covers at least 3 areas: qualitative (inappropriate medication such as typical neuroleptics), quantitative (overtreatment such as with antidiabetics),35 both related to prescribers, as well as the third player—patients’ conditions and MRH susceptibility. The present study showed an underestimated contribution of the latter. Loss of arterial pressure control even after minimal stress, such as upright standing from a supine position, provides evidence of neurovegetative failure that contributes to MRH. Although PP typically substantially falls after standing up,36 patients affected by MRH presented a 3‑fold higher value of PP change between standing and supine positions compared with the unaffected individuals. The harmfulness of supplement use seems to be an embarrassing issue, although other authors have also reported similar observations.37
Drug‑related hypotension affected every fifth patient on antihypertensive treatment. In community‑based samples, postural hypotension was present in 13% of the older people,38 which is over twice as much as in the current study. In both those studies, tranquillizers were shown to play a significant role here. In a British study of a younger population, hypotension was strongly associated with the number of antihypertensives taken, age, and comorbidities.39 This finding was not confirmed in the present study, in which failure of mechanisms controlling BP homeostasis constituted a problem beyond the use of any antihypertensive drug. Polypharmacy, including diuretics, was removed from the logistic model in favor of stronger contributors such as diabetes coexistence, benzodiazepine addiction, lower PP in a standing position, and the number of supplements taken (except vitamin D). This set of predictors suggests disease‑related neurovegetative or regulatory impairments of BP homeostasis at advanced old age rather than any effect of antihypertensive drugs. Nevertheless, drug‑induced hypotension was independently associated with mortality and hospital admission.40
Drug‑related hypoglycemia in older diabetic patients remains a major challenge.35,41 The present study confirmed previously reported results showing that advanced age, comorbidity, and β-blocker use independently act as risk factors for hypoglycemia.
Age‑related changes make older adults sensitive to the adverse effects of benzodiazepine‑related falls.42 Numerous benzodiazepine users also take other psychotropic drugs.43 In the current study, polypharmacy, weak opioids (tramadol), and worsened hemodynamic adaptation to a standing position (a lower PP value) were found to be independent contributors to addiction.
Although drug‑induced parkinsonism does not represent the most common type of MRH, it seems to be the most prevalent cause of secondary parkinsonism, which is practically irreversible and difficult to treat.44 The disorder is strongly related to the use of typical neuroleptics, especially in individuals with an inherited predisposition and pre‑existing extrapyramidal signs.44 We confirmed these findings in relation to drugs; furthermore, only this type of MRH caused shorter survival despite the discontinuation of antidopaminergic drugs during hospital stay.
Among all the drugs recommended at discharge, only spironolactone or eplerenone exerted a negative effect on survival, which may have been due to their use in end‑stage heart failure. According to the Cox model, positive effects on survival were found in users of SSRIs, paracetamol, thiazides (including indapamide), and ACEIs. The HYVET (Hypertension in the Very Elderly Trial) study carried out in a group of relatively healthy people with hypertension who were older than 80 years showed that a 2‑year active antihypertensive treatment with indapamide and perindopril was associated with a 30% reduction in the rate of fatal or nonfatal stroke, a 39% reduction in the rate of death of stroke, a 64% reduction in the rate of heart failure, and a 21% reduction in the rate of death from any cause.45 The results of the current study seem to support the findings of the HYVET clinical trial, even though a severely comorbid geriatric population was investigated here.
Of note, the associations based on the Cox proportional hazards model do not provide unequivocal evidence of causal relationships between the drug(s) and survival. The former could be a surrogate of the type and / or severity of disease that affects survival. Nevertheless, novel antidepressants, selected antihypertensives, weak analgesics, if indicated, seem to be a reasonable choice for treatable conditions in the frail older adults. These medicines, recommended by the Beers,22 STOPP, and START criteria,12 appear relatively safe for geriatric patients. Of note is the beneficial effect of SSRI use in the treatment of depression, which is common in geriatric patients. Reduced serotonergic signal transmission was found even in healthy aging.46 This class of drugs has also exerted a beneficial effect on survival in patients with cancer.47Strengths and limitations
The strength of this study lies in the holistic, standardized, and interdisciplinary geriatric approach, which considers the individual needs of patients, including medication use (before and after adjustment), during a geriatric intervention. Data from a previous study18 enabled the researcher to explore MRH in real‑life scenarios and confront the results within an over 2‑year survival period. However, it should be acknowledged that this work had several limitations. First, as the literature does not provide an unambiguous MRH typology, the researcher adopted her own classification of MRH types. Second, lack of a follow‑up study did not allow the researcher to determine whether drugs recommended at discharge were constantly taken and affected survival. Also, a limited sample size might have been insufficient to identify all potential factors for MRH and to conduct a more in‑depth statistical analysis on medication effectiveness.
Conclusions and implications
Medication‑related harm is an underappreciated iatrogenic syndrome in the geriatric population. Active search for MRH in every older patient at the beginning of the diagnostic process should be routine. Out of the dozen medications tested, 4 drug classes were found to significantly contribute to MRH of any origin, namely, typical neuroleptics, antidiabetics, benzodiazepines, and supplements. Drug‑related hypotension and / or hypoglycemia are the most common and overlapping MRHs, and tramadol use, polypharmacy, and age- and disease‑related BP neurovegatative impairment / dysregulation contributed to benzodiazepine‑related falls. Chronic use of typical neuroleptics was strongly associated with drug‑induced parkinsonism and a shorter survival rate, despite drug discontinuation. The beneficial relationships between survival and ACEIs, thiazides, paracetamol, and SSRIs revealed in this study are promising. Deprescribing and drug use optimization in geriatric patients can mitigate the negative effects of MRH on survival and, potentially, decrease the rate of rehospitalization and overall healthcare costs.
- Gnjidic D, Hilmer SN, Blyth FM, et al. Polypharmacy cutoff and outcomes: five or more medicines were used to identify community‑dwelling older men at risk of different adverse outcomes. J Clin Epidemiol. 2012; 65: 989‑995. | Crossref
- Cho S, Lau SWJ, Tandon V, et al. Geriatric drug evaluation: where are we now and where should we be in the future? Arch Intern Med. 2011; 171: 937‑940. | Crossref
- Tinetti ME, Bogardus ST Jr, Agostini JV. Potential pitfalls of disease‑specific guidelines for patients with multiple conditions. N Engl J Med. 2004; 351: 2870‑2874. | Crossref
- Stevenson JM, Davis JG, Martin FC. Medication‑related harm: a geriatric syndrome. Age Ageing. 2019; 49: 7‑11. | Crossref
- World Health Organization. Medication without harm. WHO global patient safety challenge (2017). https://apps.who.int/iris/bitstream/handle/10665/255263/WHO‑HIS‑SDS‑2017.6‑eng.pdf;jsessionid=BEAE9A48FB01C60F6940173B29CC5A9F?sequence=1. Accessed February 16, 2020.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION