Metastatic cervical lymph nodes from incidental thyroid cancer mimicking lymphomatous involvement on 18F-FDG PET/CT images



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Metastatic cervical lymph nodes from incidental thyroid cancer mimicking lymphomatous involvement on 18F-FDG PET/CT images
A 57‑year‑old man presented with splenic diffuse large B‑cell lymphoma (DLBCL) confirmed by needle aspiration biopsy in a local hospital. Fluorodeoxyglucose labeled with fluorine‑18 (18F‑FDG) positron emission tomography (PET) coregistered with computed tomography (CT) imaging was then performed for staging. It revealed splenomegaly with multiple hypermetabolic splenic masses involving splenic hilar lymph nodes (maximum standardized uptake value [SUVmax], 18.3; Figure 1A and 1B). Additionally, 3 focal thyroid lesions with an SUVmax of 20.3 and extensively enlarged cervical lymph nodes with an even higher SUVmax of 45.1 were also identified (Figure 1A and 1C). The FDG PET/CT findings in the thyroid were highly suggestive of multifocal thyroid cancer. However, it was difficult to confirm whether cervical lymphadenopathies were metastases from thyroid cancer or if they were involved by DLBCL. Ultrasound‑guided fine‑needle aspiration biopsies (UG‑FNABs) of the thyroid and bilateral cervical lymphadenopathies were then scheduled. Cytological examinations revealed papillary carcinoma, category VI of the Bethesda System for Reporting Thyroid Cytopathology (Figure 1D). Furthermore, thyroglobulin concentration in the washout fluid was greater than 500 ng/ml and the cells were positive for an activating mutation of the BRAF gene resulting in a valine‑to–glutamic acid substitution at amino acid 600 (BRAFV600E mutation; Figure 1E). Based on the above results, the diagnosis of papillary thyroid cancer with bilateral cervical lymph node metastases was clearly established. Therefore, splenic lymphoma was identified as primary splenic lymphoma (PSL) stage IISEA according to the Ann Arbor staging system. It was suggested to initiate chemotherapy for PSL and postpone treatment of thyroid cancer. After 4 cycles of R‑CHOP (rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisolone) regimen chemotherapy, interim PET/CT revealed complete remission of PSL. Intriguingly, there was no significant change in cervical abnormalities (Figure 1F).
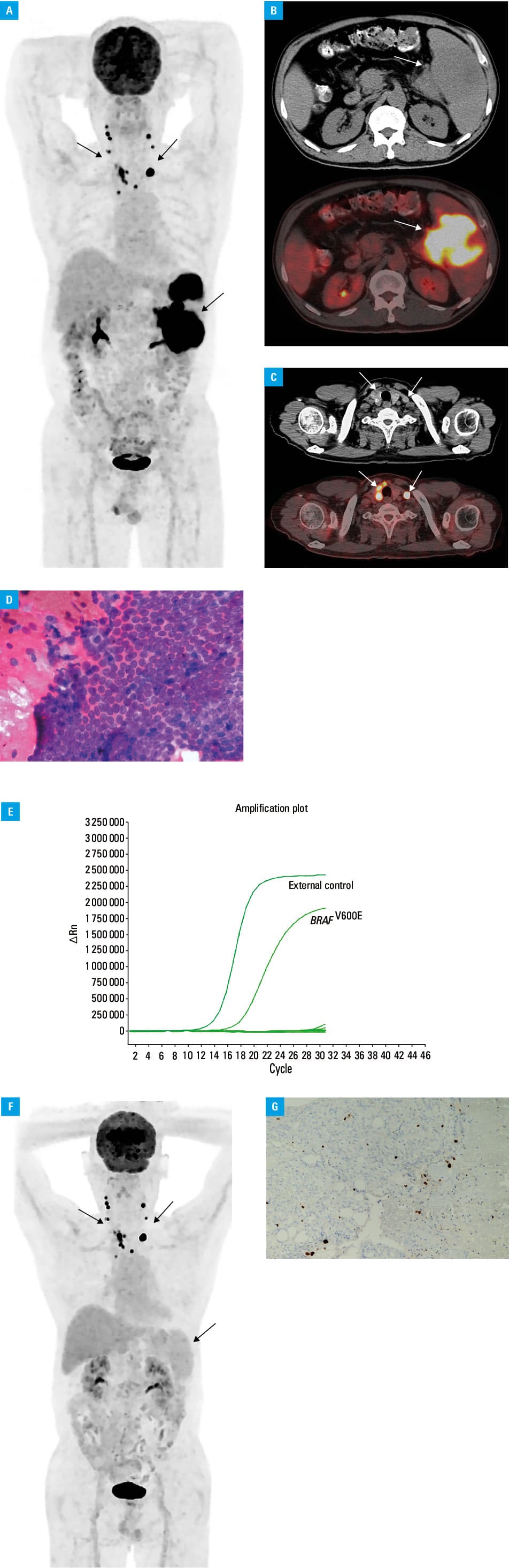
After the completion of all courses of chemotherapy, the patient underwent total thyroidectomy with radical dissection of central (level VI and VII) and bilateral (level II–V) lymph nodes. The results of histological examination validated the findings of the previous FNABs (pT3b, N1b, M0, stage II according to the 8th Edition Cancer Staging Form of the American Joint Committee on Cancer), and the Ki67 immunostaining demonstrated a low proliferative index of only 2% for the primary tumor (Figure 1G) and metastatic lymph nodes. Four weeks after surgery, the patient underwent radioactive iodine‑131 therapy (5.55 GBq) with stimulated‑serum thyroglobulin level of 5.6 ng/ml (TSH >100 IU/ml and antithyroglobulin antibody negative). Whole body scintigraphy performed after therapy showed radioiodine uptake only in the postsurgical remnant. Six months later, diagnostic whole body scintigraphy was negative under thyrotropin stimulation with stimulated‑serum thyroglobulin level of less than 1 ng/ml, and neck ultrasonography revealed no abnormalities. Until the time of manuscript submission, the patient was in good condition.
An FDG‑avid thyroid incidentaloma discovered during a PET/CT examination performed due to unrelated thyroid disease is known as the “PAIN” phenomenon.1 The incidence of this phenomenon varies from 1% to 4.3%,2 and thyroid cancer represents approximately 35% of such cases, with papillary carcinoma as the most frequent histological type.3 Kaliszewski et al2 reported that cytology results were significant predictors of cancer in patients with the “PAIN” phenomenon, and recommended surgical treatment in patients with cytology assigned to category III or higher of the Bethesda system, due to significant risk of thyroid malignancy. As far as we know, this is the first report of such extremely intense FDG uptake in metastatic lymph nodes from incidental papillary carcinoma mimicking DLBCL involvement. This case exemplifies that accelerated glucose metabolism in thyroid cancer is not always dependent on poor differentiation and / or rapid proliferation, but may be due to genetic alterations, such as BRAFV600E mutation.4,5 It also highlights that cytological examination of FNAB specimens is necessary for recognizing the “PAIN” phenomenon and preventing wrong staging of the synchronous malignancy.
- Katz SC, Shaha A. PET‑associated incidental neoplasms of the thyroid. J Am Coll Surg. 2008; 207: 259‑264. | Crossref
- Kaliszewski K, Diakowska D, Zietek M, et al. Thyroid incidentaloma as a “PAIN” phenomenon – does it always require surgery? Medicine (Baltimore). 2018; 97: e13339. | Crossref
- Pattison DA, Bozin M, Gorelik A, et al. (18)F‑FDG‑avid thyroid incidentalomas: the importance of contextual interpretation. J Nucl Med. 2018; 59: 749‑755. | Crossref
- Barollo S, Pennelli G, Vianello F, et al. BRAF in primary and recurrent papillary thyroid cancers: the relationship with (131)I and 2-[(18)F]fluoro‑2‑deoxy‑D‑glucose uptake ability. Eur J Endocrinol. 2010; 163: 659‑663. | Crossref
- Nagarajah J, Ho AL, Tuttle RM, et al. Correlation of BRAFV600E mutation and glucose metabolism in thyroid cancer patients: an (1)(8)F‑FDG PET study. J Nucl Med. 2015; 56: 662‑667. | Crossref
ARTICLE INFORMATION