Remdesivir-based therapy improved the recovery of patients with COVID-19 in the multicenter, real-world SARSTer study



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Remdesivir-based therapy improved the recovery of patients with COVID-19 in the multicenter, real-world SARSTer study
Introduction
In December 2019, a new pathogen associated with an outbreak of respiratory tract infections was discovered in Wuhan, China. It was identified as a novel coronavirus termed severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2), closely related to the already known betacoronaviruses responsible for epidemics named with the acronyms SARS (severe acute respiratory syndrome) and MERS (Middle East respiratory syndrome). The outbreak of the disease cause by SARS‑CoV‑2, coronavirus disease 2019 (COVID‑19), was announced a global pandemic by the World Health Organization (WHO) in March 2020. The clinical spectrum of SARS‑CoV‑2 infection ranges from asymptomatic or mild, self‑limited respiratory tract disease to severe progressive pneumonia leading to acute respiratory distress syndrome and death due to multiorgan failure. At the beginning of the epidemic, only supportive care was available, but the rapid worldwide spread of COVID‑19 has raised a desperate need to invent an antiviral agent active against SARS‑CoV‑2. At first, the search for an effective therapy focused on drug repurposing and new ways of using approved agents with confirmed activity against other viruses. Among them, a compound of lopinavir and ritonavir was identified. Lopinavir, acting as an inhibitor of human immunodeficiency virus (HIV) protease, coadministered with ritonavir to increase its bioavailability, was demonstrated to have in vitro activity against both SARS‑CoVs and MERS‑CoVs.1-5 The positive impact of lopinavir / ritonavir on the clinical outcome and reduction of the viral load in nasopharyngeal swabs was documented in patients participating in an open‑label study performed during the outbreak of SARS in 2003.2,3 Three case reports and a single retrospective study focused on the use of lopinavir / ritonavir in patients with MERS, suggesting improved clinical outcomes.6,7 Hence, due to the structural similarity of all betacoronaviruses, the relevance of lopinavir / ritonavir use in the treatment of COVID‑19 was considered. To answer the question as to whether this antiviral agent works in SARS‑CoV‑2 infection, Cao et al8 performed an open‑label randomized clinical trial in Wuhan, China, the epicenter of the outbreak, to evaluate the efficacy of lopinavir / ritonavir in patients diagnosed with COVID‑19. Nevertheless, study results were disappointing and no superiority of lopinavir / ritonavir therapy in terms of clinical improvement, duration of hospitalization, or time period of viral RNA detectability as compared with the standard of care (SoC) was demonstrated. The only significant difference was observed in the median time to clinical improvement, calculated after exclusion of patients who died early; however, the authors regarded that difference as “modest.”8 No positive impact of lopinavir / ritonavir therapy was reported in critically ill patients with SARS‑CoV‑2–related pneumonia treated in the intensive care unit and also in patients with the mild‑to‑moderate form of COVID‑19 compared with the SoC treatment or adjuvant therapy.9-11
Since the process of discovery, testing, and registration of a new antiviral drug is long, costly, and has a vague chance of success, attention has been paid to investigational drugs with a potential activity against SARS‑CoV‑2. Remdesivir has been the most promising one among them, a prodrug of an adenosine nucleoside analogue, which terminates viral RNA synthesis by inhibition of RNA‑dependent RNA polymerase and has an established dosing and safety profile. Ebola virus disease was the primary clinical indication for remdesivir use. However, despite the encouraging results of the in vivo efficacy evaluation in an animal model, a phase III randomized clinical trial did not clearly confirm the relevance of remdesivir use in humans and, then, this investigational agent was shelved.12 There has been renewed interest in remdesivir use for SARS‑CoV and MERS‑CoV infection treatment, and its activity against the family of coronaviruses, which was confirmed in in vitro and animal models, has raised hope for its effective application in the treatment of COVID‑19.13 Since the inhibitory effect on the recently emerged novel coronavirus was demonstrated in vitro, clinical trials and compassionate use programs have been initiated, and the WHO announced the launch of a trial that would include a single group of patients treated with remdesivir.14-16 Finally, based on findings from phase III clinical trials, ACTT‑1 and SIMPLE‑severe, remdesivir received emergency use authorization for the treatment of COVID‑19, issued by the Food and Drug Administration (FDA) on May 1, 2020.17-19 The subsequent final approval by the FDA and licences in various countries worldwide as well as recommendation by numerous scientific infectious disease societies have made remdesivir the first approved antiviral agent for the treatment of COVID‑19. However, due to doubts raised by the results of the Solidarity study, it is of importance to support registration research with data from real‑world experience.20
The purpose of the current study was to evaluate the effectiveness and safety of remdesivir use in patients with COVID‑19 in real‑world settings. The lopinavir / ritonavir–based regimen was used as a comparator instead of the undefined and imperfect concept of the SoC usually applied in COVID‑19 studies.
Patients and methods
The study population consisted of patients selected from 1496 individuals included in the SARSTer national database. This ongoing project, supported by the Polish Association of Epidemiologists and Infectiologists, is a national real‑world experience study on the treatment of patients with COVID‑19. Patients whose data were collected in the SARSTer database were treated in 30 Polish centers between March 1 and August 31, 2020. The decision about the treatment regimen was taken entirely by the treating physician with respect to the current knowledge and recommendations of the Polish Association of Epidemiologists and Infectiologists.21,22 The present analysis included 333 adult patients who received therapy with the 2 antiviral drugs, remdesivir or lopinavir / ritonavir, administered for the treatment of COVID‑19. Remdesivir was administered intravenously at a loading dose of 200 mg once a day and later at a maintenance dose of 100 mg for 5 to 10 days. Lopinavir / ritonavir was administered orally at a dose of 400/100 mg every 12 hours for up to 28 days. Lopinavir / ritonavir was used mostly at the beginning of the pandemic and, owing to the later documented lack of effectiveness, was considered as a comparator for remdesivir in this study. The SARSTer study was approved by the Ethical Committee of Medical University of Bialystok, Poland. If necessary, local bioethics committees approved the experimental use of repurposed drugs (lopinavir / ritonavir) in patients with COVID‑19.
Data were retrospectively entered and submitted online by a web‑based platform operated by the Tiba sp. z o.o. company. Parameters recorded at baseline included age, sex, body mass index (BMI), comorbidities and concomitant medication use, clinical status on admission, additional medication dedicated to COVID‑19 treatment, and adverse events. Baseline clinical status on hospital admission was classified as asymptomatic, stable symptomatic with oxygen saturation (SpO2) >95%, unstable symptomatic with SpO2 at 91% to 95%, unstable symptomatic with SpO2 ≤90% or acute respiratory distress syndrome.
Clinical improvement, expressed using the ordinal scale based on the WHO recommendations modified to fit the specificity of the national healthcare system, was regarded as the primary endpoint of treatment effectiveness. Improvement was defined as a 2‑point decrease from baseline at 7, 14, 21, and 28 days of hospitalization. The ordinal scale included the following: 1. nonhospitalized, no activity restrictions; 2. nonhospitalized, no activity restrictions, and / or requiring oxygen supplementation at home; 3. hospitalized, not requiring oxygen supplementation or medical care; 4. hospitalized, not requiring oxygen supplementation but requiring medical care; 5. hospitalized, requiring normal oxygen supplementation; 6. hospitalized, on noninvasive ventilation with high‑flow oxygen therapy equipment; 7. hospitalized, using invasive mechanical ventilation or extracorporeal membrane oxygenation; 8. death.
The secondary endpoints of effectiveness included: mortality rate, rate of the need for constant oxygen therapy, duration of oxygen therapy, rate of the need for mechanical ventilation, total hospitalization time, and rate of positive real‑time polymerase chain reaction (PCR) testing for SARS‑CoV‑2 after 30 days of hospitalization.
Statistical analysis
Study results were expressed as mean (SD) or number (percentage). A P value less than 0.05 was considered significant. The significance of differences was calculated by the χ2 or Fisher exact tests for nominal variables and by the Mann–Whitney test and the Kruskal‑Wallis analysis of variance for continuous variables. Univariable comparisons were calculated using the GraphPad Prism 5.1 software (GraphPad Software, Inc., La Jolla, California, United States). Forward stepwise logistic regression models with the Bayesian information criterion as a model selection criterion were constructed with an equal to or higher than 2‑point decrease on the ordinal scale between baseline and hospitalization day 21 as the dependent variable. Among independent variables tested, there were age, sex, BMI, diabetes, coronary artery disease, baseline classification and baseline score based on the ordinal scale, as well as therapy with remdesivir, lopinavir / ritonavir, tocilizumab, dexamethasone, chloroquine / hydroxychloroquine, heparin, convalescent plasma, and azithromycin. Only the main effects and first‑order interaction terms without predictor rescaling were considered in the model building procedure. Logistic regression models were calculated with the use of the R and MATLAB software (MathWorks, Natick, Massachusetts, Unites States).
Results
Among 333 patients included in the study, 122 received remdesivir therapy, and 211 were treated with lopinavir / ritonavir. The study groups were balanced regarding sex, age, and BMI, but there was a predominance of male patients in both study arms (Table 1). Patients treated with remdesivir more frequently demonstrated a symptomatic unstable course of the disease with SpO2 ≤95% on admission to the hospital (69%) compared with those receiving lopinavir / ritonavir (57%), but the difference was nonsignificant. The prevalence of comorbidities was higher among patients treated with remdesivir, but the difference was significant only regarding ischemic heart disease (Table 1). During remdesivir treatment, additional medication used more frequently included dexamethasone, convalescent plasma, and low‑molecular‑weight heparin, whereas lopinavir / ritonavir was more frequently administered together with chloroquine and azithromycin (Table 1).
Characteristics | Remdesivir (n = 122) | Lopinavir /ritonavir (n = 211) | P value |
Data are presented as numer (percentage) of patients unless otherwise indicated.
Abreviations: ARDS, acute respiratory distress syndrome; BMI, body mass index; COVID‑19, coronavirus disease 2019; LMWH, low‑molecular‑weight heparin; SpO2, oxygen saturation | |||
Demographic data | |||
Female sex | 43 (35) | 85 (40) | 0.41 |
Male sex | 79 (65) | 126 (60) | |
Age, y, mean (SD) | 58.7 (14.5) | 56.1 (15.4) | 0.15 |
BMI, kg/m2, mean (SD) | 29.3 (4.5) | 28.2 (5.1) | 0.05 |
Baseline clinical status on hospital admission | |||
Asymptomatic | 1 (0.8) | 7 (3.3) | 0.27 |
Stable symptomatic, SpO2 >95% | 38 (31) | 83 (39) | 0.16 |
Unstable symptomatic, SpO2 at 91%–95% | 52 (43) | 70 (33) | 0.1 |
Unstable symptomatic, SpO2 ≤90% | 30 (25) | 49 (23) | 0.79 |
ARDS | 1 (0.8) | 2 (0.9) | 1.00 |
Comorbidities | |||
Hypertension | 65 (53) | 101 (48) | 0.36 |
Ischemic heart disease | 17 (14) | 13 (6) | 0.03 |
Other cardiovascular diseases | 14 (11) | 14 (7) | 0.15 |
Diabetes | 29 (24) | 38 (18) | 0.26 |
Chronic obstructive pulmonary disease | 4 (3) | 7 (3) | 1.00 |
Asthma | 4 (3) | 4 (2) | 0.47 |
Malignancy | 6 (5) | 10 (5) | 1.00 |
Additional medication dedicated to COVID‑19 treatment | |||
Chloroquine | 7 (5.7) | 153 (73) | <0.001 |
Hydrochloroquine | 2 (1.6) | 14 (6.6) | 0.06 |
Tocilizumab | 27 (22) | 34 (16) | 0.19 |
Convalescent plasma | 17 (14) | 13 (6.2) | 0.03 |
LMWH at prophylactic doses | 109 (89) | 137 (65) | <0.001 |
LMWH at therapeutic doses | 9 (7.4) | 13 (6.2) | 0.65 |
Dexamethasone | 31 (25) | 18 (8.5) | <0.001 |
Azithromycin | 10 (8) | 37 (18) | 0.02 |
As shown in Figure 1, the proportions of ordinal‑scale categories were balanced between the 2 treatment groups at baseline. The rate of patients discharged from the hospital was similar on days 7 and 14, but it increased in patients treated with remdesivir on days 21 and 28 (Figure 1). Differences in the ordinal‑scale score between particular timepoints and baseline values on admission to the hospital are shown in Figure 2. Clinical improvement measured using an ordinal scale demonstrated significantly higher rates after remdesivir treatment compared with lopinavir / ritonavir use on days 21 and 28, and the difference was 15% and 10%, respectively (Table 2). An additional analysis of clinical improvement based on the ordinal scale was carried out depending on the baseline oxygen saturation on hospital admission. The difference between the regimens increased along with worsening of oxygen saturation during the analysis on days 14, 21, and 28 (Table 2). A similar tendency was demonstrated depending on the baseline score based on the ordinal scale. As shown in Table 2, hospitalization time was significantly shorter in patients treated with remdesivir if they had baseline SpO2 ≤90%.
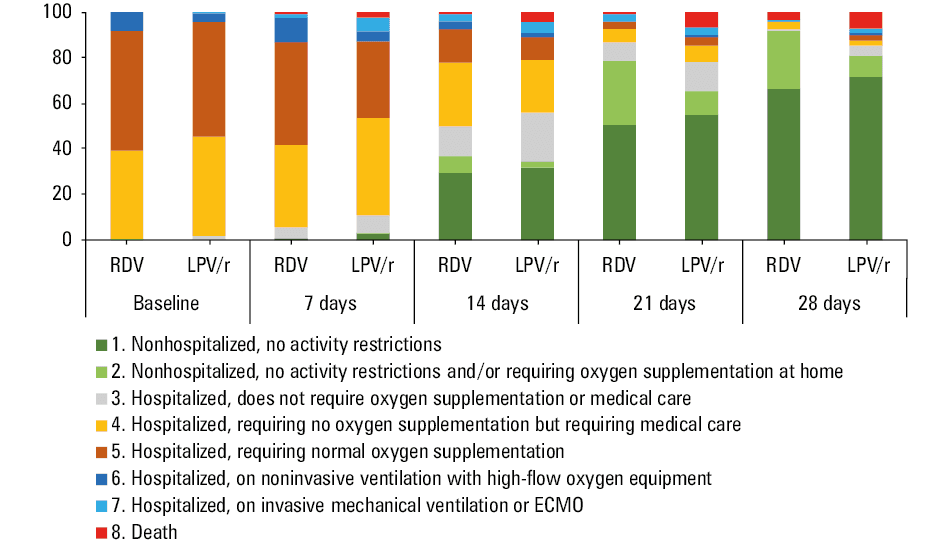
Abbreviations: ECMO, extracorporeal membrane oxygenation; LPV/r, lopinavir / ritonavir; RDV, remdesivir
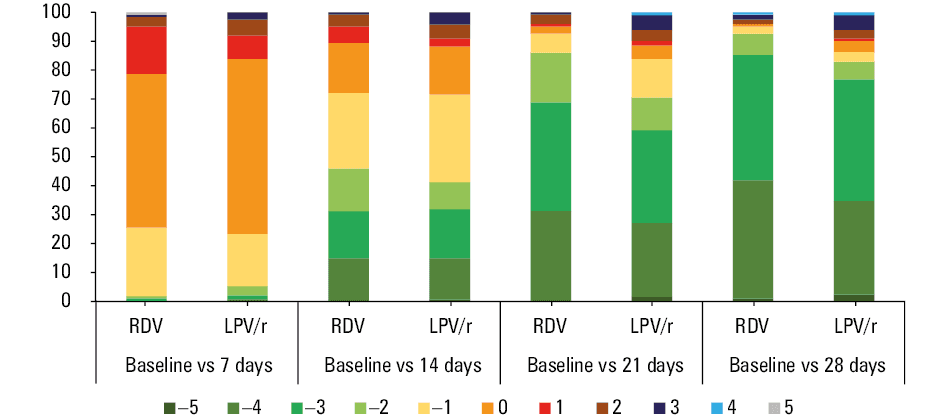
Abbreviations: see Figure 1
Endpoint | Follow‑up, days | Remdesivir (n = 122) | Lopinavir/ritonavir (n = 211) | OR (95% CI) | P value | ||
Data are presented as number of patients affected / total number of patients in whom data were available (percentage) unless otherwise indicated.
Abbreviations: OR, odds ratio; PCR, polymerase chain reaction; others, see Table 1 | |||||||
Clinical improvement (≥2‑point decrease on the ordinal scale) | All patients | 7 | 2/122 (1.6) | 11/211 (5.2) | 0.3 (0.07–1.39) | 0.14 | |
14 | 56/122 (46) | 87/211 (41) | 1.21 (0.77–1.9) | 0.42 | |||
21 | 105/122 (86) | 149/211 (71) | 2.57 (1.42–4.65) | 0.001 | |||
28 | 113/122 (93) | 175/211 (81) | 2.58 (1.2–5.57) | 0.01 | |||
Depending on SpO2 | >95% | 7 | 1/38 (2.6) | 7/83 (8.4) | 0.29 (0.04–2.47) | 0.43 | |
14 | 17/38 (45) | 37/83 (45) | 1.01 (0.47–2.18) | 1.00 | |||
21 | 34/38 (89) | 68/83 (82) | 1.88 (0.58–6.09) | 0.42 | |||
28 | 37/38 (97) | 79/83 (95) | 1.87 (0.2–17.35) | 1.00 | |||
91%–95% | 7 | 0/52 | 2/70 (2.9) | 0.26 (0.01–5.55) | 0.51 | ||
14 | 28/52 (54) | 34/70 (49) | 1.23 (0.6–2.53) | 0.59 | |||
21 | 47/52 (90) | 54/70 (77) | 5.17 (1.1–24.22) | 0.09 | |||
28 | 50/52 (96) | 58/70 (83) | 5.17 (1.1–24.22) | 0.02 | |||
≤90% | 7 | 1/30 (3.3) | 2/49 (4.1) | 0.81 (0.07–9.34) | 1.00 | ||
14 | 10/30 (33) | 12/49 (24) | 1.54 (0.57–4.19) | 0.44 | |||
21 | 22/30 (73) | 23/49 (47) | 3.11 (1.16–8.32) | 0.03 | |||
28 | 24/30 (80) | 33/49 (67) | 1.94 (0.66–5.69) | 0.3 | |||
Depending on the baseline score on the ordinal scale | 3–4 | 7 | 1/48 (2.1) | 6/96 (6.3) | 0.32 (0.04–2.73) | 0.42 | |
14 | 22/48 (46) | 39/96 (41) | 1.23 (0.62–2.49) | 0.6 | |||
21 | 43/48 (90) | 70/96 (73) | 3.19 (1.14–8.95) | 0.03 | |||
28 | 46/48 (96) | 84/96 (88) | 3.28 (0.71–15.32) | 0.14 | |||
5 | 7 | 1/64 (1.6) | 4/106 (3.8) | 0.41 (0.04–3.7) | 0.65 | ||
14 | 28/64 (44) | 46/106 (43) | 1.01 (0.54–1.9) | 1.00 | |||
21 | 54/64 (84) | 74/106 (70) | 2.33 (1.06–5.16 | 0.04 | |||
28 | 58/64 (91) | 85/106 (80) | 2.39 (0.91–6.28) | 0.08 | |||
6–7 | 7 | 0/10 | 1/9 (11) | 0.27 (0.01–7.51) | 0.47 | ||
14 | 6/10 (60) | 2/9 (22) | 5.25 (0.7–39.48) | 0.17 | |||
21 | 8/10 (80) | 5/9 (56) | 3.2 (0.42–24.4) | 0.35 | |||
28 | 9/10 (90) | 6/9 (67) | 4.50 (0.37–54.16) | 0.3 | |||
Death | All patients | – | 5/122 (4.1) | 17/211 (8.1) | 0.49 (0.18–1.34) | 0.18 | |
SpO2 ≤95% | – | 4/82 (4.9) | 14/119 (11.8) | 0.39 (0.12–1.21) | 0.13 | ||
Need for continuous oxygen therapy | – | 54/122 (44) | 107/211 (51) | 0.77 (0.49–1.21) | 0.31 | ||
Duration of oxygen therapy, day, mean (SD) | – | 10.2 (6.6) | 12.1 (11.2) | – | 0.72 | ||
Need for mechanical ventilation | – | 7/122 (5.7) | 18/211 (8.5) | 0.65 (0.27–1.61) | 0.39 | ||
Hospitalization time, day, mean (SD)
(excluding patients who died) | All patients | – | 15.6 (6.6) | 18.1 (10.4) | – | 0.07 | |
Depending on SpO2 | >95% | – | 14.6 (4.7) | 15.7 (6.2) | – | 0.61 | |
91%–95% | 15.2 (6.7) | 16.6 (9) | – | 0.3 | |||
≤90% | 17.5 (8.2) | 25 (14.7) | – | 0.03 | |||
Depending on the baseline score on the ordinal scale | 3–4 | 14.3 (5.2) | 17 (9.2) | – | 0.12 | ||
5 | 16.2 (7.3) | 18.8 (11.4) | – | 0.26 | |||
6–7 | 17.9 (6.7) | 21.7 (8.7) | – | 0.52 | |||
Positive result of real‑time PCR testing after 30 days of hospitalization | 30 | 5/122 (4.1) | 19/211 (9) | 0.43 (0.16–1.19) | 0.12 | ||
Adverse events | Any adverse events | – | 24/122 (20) | 83/211 (39) | 0.38 (0.22–0.64) | <0.001 | |
Diarrhea | 0/122 | 53/211 (25) | 0.01 (0.001–0.2) | <0.001 | |||
Elevated aminotransferase levels | 12/122 (9.8) | 6/211 (2.8) | 3.73 (1.36–10.2) | 0.01 | |||
Nausea | 2/122 (1.6) | 18/211 (8.5) | 0.57 (0.11–2.87) | 0.01 | |||
Vomiting | 1/122 (0.8) | 13/211 (6.2) | 0.13 (0.02–0.97) | 0.01 | |||
QT interval prolongation | 0/122 | 11/211 (5.2) | 0.07 (0.004–1.22) | 0.008 | |||
In the logistic regression model of patients receiving remdesivir or lopinavir / ritonavir, only remdesivir use was independently associated with at least a 2‑point improvement on the ordinal scale between baseline and day 21, while older age and tocilizumab use were negative predictors of the patient’s response (Table 3). Interestingly, in patients at older age, tocilizumab improved the likelihood of response.
Characteristics | β Estimate | SE | T statistic | P value | OR (95% CI) |
χ2 statistic vs constant model, 45.5; P value, 3.1–9; and Bayesian information criterion, 310.29
Abbreviations: see Table 2 | |||||
Intercept | 4.1063 | 0.7743 | 5.3 | <0.001 | – |
Remdesivir (0/1) | 1.5014 | 0.3752 | 4 | <0.001 | 4.13 (2.06–8.27) |
Tocilizumab (0/1) | –4.9421 | 1.644 | –3.01 | 0.003 | 0.0071 (0.0003–0.17) |
Age (per year) | –5.1216–2 | 1.2446–2 | –4.12 | <0.001 | 0.94 (0.92–0.97) |
Tocilizumab vs age | 0.063616 | 0.02631 | 2.42 | 0.02 | 1.07 (1.01–1.12) |
Patients treated with lopinavir / ritonavir experienced more adverse events (39%) than those treated with remdesivir (20%). The most frequent adverse events in those receiving lopinavir / ritonavir included diarrhea (25%), nausea (8.5%), vomiting (6.2%), and QT interval prolongation (5.2%). Patients treated with remdesivir most frequently had elevated levels of aminotransferases (9.8%), and other adverse events occurred sporadically (Table 2).
Discussion
Since May 1, 2020, the FDA has approved remdesivir to be distributed and administered intravenously to treat COVID‑19 in patients with the severe course of the disease by granting emergency use authorization. It has become possible in view of the promising results of phase III clinical trials. Hence, the antiviral agent that failed to live up to expectations in the treatment of Ebola virus disease has become a hope for those infected with SARS‑CoV‑2. Approvals issued in other countries and regions worldwide in the wake of the decision of the United States federal agency has enabled the use of remdesivir in patients with low blood oxygen saturation or need for oxygen therapy or more intensive breathing support. However, giving access to a new potential therapy, the need for further research to evaluate the safety and effectiveness of remdesivir was highlighted.
Since June 2020, remdesivir has also been available in Poland. Therefore, we aimed to assess the efficacy and tolerability of remdesivir in real‑world experience. A lopinavir / ritonavir–based regimen was used as a comparator owing to its antiviral mode of action, as both agents act by inhibiting viral proteins. We used this regimen instead of the undefined and imperfect concept of “SoC,” which is usually applied in COVID‑19 studies and can be interpreted in different ways depending on the treating center and phase of the pandemic. As no benefit of lopinavir / ritonavir treatment compared with the SoC was reported by Cao et al8 in patients with COVID‑19–related pneumonia, in the current analysis, we assumed that the efficacy of lopinavir / ritonavir was at the level close to that of placebo. The majority of patients receiving remdesivir presented with unstable symptomatic clinical status with SpO2 ≤95% on hospital admission (68%). Using the ordinal scale widely applied in COVID‑19 trials, we confirmed that remdesivir therapy was associated with greater clinical improvement, defined as a 2‑point decrease in disease severity, by days 21 (86% vs 71%; P = 0.001) and 28 (93% vs 83%; P = 0.01) compared with the lopinavir / ritonavir arm. A significant difference on day 21 was observed regardless of the baseline score on admission to the hospital. The detailed analysis considering the baseline oxygen saturation demonstrated a significant difference among unstable patients, by day 21 for individuals with SpO2 ≤90%, and by day 28 for those with baseline SpO2 at 91% to 95%. The possible reason for no difference observed by days 7 and 14 could be an effect of a national regulation followed until August 31, 2020, which in practice ordered hospitalization of the majority of patients for at least 14 days irrespective of treatment used or clinical improvement observed.
Hence, our findings supported results from clinical trials, including those based on which the decisions of authorization by the FDA and European Medicines Agency (EMA) were made.17-19 Patients with COVID‑19 without reduced oxygen saturation included in the SIMPLE‑moderate phase III trial and treated with remdesivir for 5 days were more likely to exhibit clinical improvement as compared with those receiving the SoC treatment alone, whereas no significant difference was documented for those randomized to the 10‑day regimen.23 Similar results were obtained for patients with the severe form of COVID‑19 defined as oxygen saturation <95% while breathing ambient air or receiving oxygen support, treated with remdesivir in the SIMPLE‑severe phase III trial. Clinical improvement was demonstrated in 65% and 54% of patients receiving remdesivir for 5 and 10 days, respectively.18 In both trials, the assessment was performed at a timepoint different from ours, on day 11 for moderate and 14 for severe disease.18,19,23 Notably, the comparison concerning patients with severe COVID‑19 was not randomized and performed within a single study yet between individuals on remdesivir therapy included in the SIMPLE‑severe phase III clinical trial and the concurrent retrospective real‑world cohort study on SoC only.19 Moreover, not all patients treated with remdesivir were included in the comparative analysis. After exclusion of Italian patients on remdesivir from the real‑world experience study owing to lack of comparative individuals receiving SoC, 74% of those treated with remdesivir fulfilled the criteria for clinical improvement as compared with 59% in the SoC cohort on day 14 (P <0.001).
This limitation was not shared by another phase III ACTT‑1 study designed as a double‑blind, randomized, and placebo‑controlled trial. The preliminary results of that study confirmed the superiority of remdesivir to placebo (normal saline solution) in shortening the time to recovery (11 versus 15 days). Patients were assessed daily using an ordinal scale, and the primary outcome measure was the first day on which the patient reached one of the 3 lowest levels on the scale meaning “not hospitalized with or without limitation of activities” and “hospitalized not requiring supplemental oxygen and ongoing medical care.”17 Also, data from the compassionate use program confirmed the benefit of remdesivir treatment in patients with severe COVID‑19, including those on invasive ventilation, and showed a 68% rate of clinical recovery.24 Unlike the abovementioned studies, no positive impact of remdesivir compared with placebo was reported in patients with the severe form of COVID‑19 with baseline oxygen saturation <95% who were included in a randomized, double‑blind, multicenter phase III clinical trial conducted in Wuhan, China.14 However, it should be noted that enrolment was prematurely terminated, as the epidemic in Wuhan was controlled and hence the study was underpowered.
The benefits of remdesivir use were not proven in the WHO‑planned Solidarity study.20 Despite the enormous number of patients included in that study, it did not influence the decisions of the FDA, EMA, and the most important scientific societies recommending the use of remdesivir. The primary drawback of the Solidarity study was the fact that patients were not categorized into those receiving oxygen at low or high flow. Patients were grouped by whether they did or did not need supplemental oxygen or if they were on ventilators. The difference may be of importance, because people who need less oxygen can be at an earlier stage of infection than those who need more oxygen. Meanwhile, as shown in the ACTT‑1 trial and in our study, the benefits of using remdesivir are achieved by patients who require low oxygen flow.17
The current analysis demonstrated the beneficial effect of remdesivir therapy as compared with lopinavir / ritonavir use in terms of secondary endpoints. Among them, a significant difference was found for the rate of lack of improvement within 28 days assessed on the ordinal scale. For the remaining parameters, including mortality rate, need for constant oxygen therapy and its duration, need for mechanical ventilation, rate of positive results of real‑time PCR testing for SARS‑CoV‑2 after 30 days, and hospitalization length, the positive impact of remdesivir without statistical significance was documented. Interestingly, the most striking and significant effect of remdesivir use on the length of hospitalization was observed in patients with baseline SpO2 ≤90% who needed hospital stay shorter by 7 days on average. Our findings on mortality are in line with the results achieved in the SIMPLE and ACTT‑1 clinical trials and an observational study of patients with cancer.17,19,23,25 Unfortunately, a detailed comparison regarding the remaining outcomes is impossible because of different endpoints and timepoints of assessment analyzed.17,19,23
The tolerability profile of remdesivir in the current analysis was in accordance with that seen in clinical trials, and transient aminotransferase elevations were the most frequently observed adverse event, reported in nearly 10% of patients. Lopinavir / ritonavir was frequently responsible for transient diarrhea, well known from experience in patients with HIV infection, which did not affect the clinical status of patients and duration of hospitalization.
Strengths and limitations
We are aware of the limitations of our study. Among them, the impact of other therapeutic agents dedicated to COVID‑19 treatment should be pointed out. Baseline characteristics demonstrated the different distribution of patients with respect to concomitant drugs with a significantly higher rate of dexamethasone, convalescent plasma, and low‑molecular‑weight heparin use, and a lower rate of chloroquine and azithromycin use among patients treated with remdesivir. To eliminate this imbalance as a confounding factor, we performed analysis using logistic regression, which showed that, in patients receiving remdesivir or lopinavir / ritonavir, only the administration of remdesivir was independently associated with at least a 2‑point improvement on the ordinal scale on day 21. Importantly, in that model, we could not prove an additional independent beneficial effect of dexamethasone or convalescent plasma use on this endpoint, while the use of tocilizumab was beneficial only in older patients.
Other limitations of the current analysis are related to the real‑world evidence design of the study, including its observational character and retrospective electronic data collection burdened with possible data entry errors. Unfortunately, we could not increase the number of patients in the study because of the change in national regulations, which allowed the release of a patient from the hospital without real‑time PCR test negativization—this could significantly affect ordinal scale interpretation.
However, the major strength of the study lies in collection of data from a real‑world, heterogeneous population, thus being representative for routine practice, and a clearly defined comparator, unlike in some other studies that usually use an undefined concept of SoC. Interestingly, we observed that the addition of tocilizumab can improve the likelihood of clinical improvement, which supports our previous experience with this drug, but the possible use of the combined therapy with remdesivir and tocilizumab needs further research.26
Conclusions
Due to the complex pathogenesis and multiphasic clinical course of COVID‑19 with coagulation disorders, coinfections, multiorgan failure, and consequences of a “cytokine storm,” it is difficult to find the optimal management. An enormous number of repurposed drugs are still being tested for both antiviral, anti‑inflammatory, and cytokine storm control.27 Those studies also investigate the possibility of using remdesivir with other drugs, an example of which is baricitinib recently approved by the FDA for combination therapy with remdesivir.28
In conclusion, data collected in this retrospective, observational, real‑world study with antivirals as a leading therapy in 2 competing arms supported the use of remdesivir compared with lopinavir / ritonavir for the treatment of SARS‑CoV‑2 infection, particularly in patients with oxygen saturation ≤95%.
- Yamamoto N, Yang R, Yoshinaka Y, et al. HIV protease inhibitor nelfinavir inhibits replication of SARS‑associated coronavirus. Biochem Biophys Res Commun. 2004; 318: 719‑725. | Crossref
- Chen F, Chan KH, Jiang Y, et al. In vitro susceptibility of 10 clinical isolates of SARS coronavirus to selected antiviral compounds. J Clin Virol. 2004; 31: 69‑75. | Crossref
- Chu CM, Cheng VC, Hung IF, et al. Role of lopinavir/ritonavir in the treatment of SARS: initial virological and clinical findings. Thorax. 2004; 59: 252‑256. | Crossref
- deWilde AH, Jochmans D, Posthuma CC, et al. Screening of an FDA‑approved compound library identifies four small‑molecule inhibitors of Middle East respiratory syndrome coronavirus replication in cell culture. Antimicrob Agents Chemother. 2014; 58: 4875‑4884. | Crossref
- Chan JF, Yao Y, Yeung ML, et al. Treatment with lopinavir/ritonavir or interferon-β1b improves outcome of MERS‑CoV infection in a nonhuman primate model of common marmoset. J Infect Dis. 2015; 212: 1904‑1913. | Crossref
ARTICLE INFORMATION