The evolution from an “average” study patient to patient-specific characteristics to guide interventions in vascular medicine



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The evolution from an “average” study patient to patient-specific characteristics to guide interventions in vascular medicine
It’s about integrating individual clinical expertise and the best external evidence
Sackett DL, Rosenberg WM, Gray JA, et al. Evidence‑based medicine: what it is and what it isn’t. BMJ. 1996; 312: 71.
There is false optimism today that cardiovascular disease is no longer a major public health problem. Quite the opposite: despite the unquestionable progress in cardiovascular pharmacotherapy and prevention, the burden of cardiovascular disease is increasing.1 Over the next 20 years at least, ischemic heart disease and stroke will remain the top causes of death and premature death and will continue as the largest disease burden in Europe, with stroke as the number 1 cause for disability.1 Nowadays, strokes are, in their substantial proportion, preventable2 and educated efforts are urgently needed to reduce this proportion.1 The implementation of existing knowledge is essential to reduce the number of strokes, but it is not sufficient.1 Approaches for early disease detection need to be paired with further insights into disease mechanisms, taking advantage of novel technologies, including new biomarkers, imaging and “big” data in risk stratification.1,3 It becomes fundamental today to understand individual variations in disease pathology and the risk of symptom occurrence.3 Safe and more efficacious treatments, regarding both pharmacotherapy and devices, need to be applied on a patient‑specific basis—to precisely target and modify the disease‑related risks.1
Stroke is one of the most dreaded events in life. Over 80% of strokes occur without any clinical warning. A substantial proportion of stroke survivors are left with major mental and physical disability. The consequences are detrimental not only for the patient but also for the families, the healthcare system, and society. Large‑scale efforts are needed to maximize preventive rather than reactive treatment strategies. Atherosclerotic carotid disease is responsible for a much greater proportion of strokes than just those presenting with tandem occlusion of the intra- and extracranial vessels (approximately 20%). It is also the underlying cause for hemodynamic strokes due to a high‑grade carotid stenosis. In addition, showers of emboli from a “hot” carotid plaque can cause severe strokes, even in the absence of large vessel occlusion.
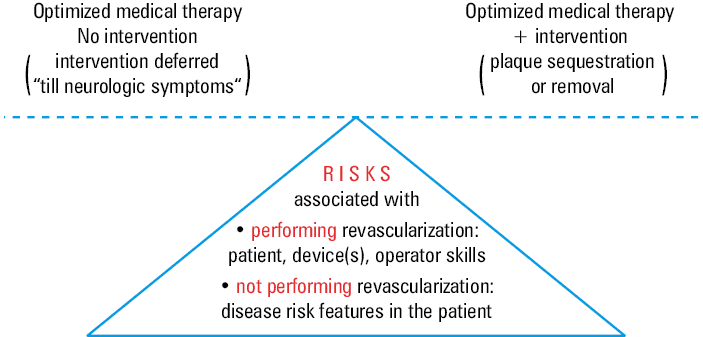
After detection of a clinically “asymptomatic” carotid stenosis (that may in reality not be truly asymptomatic, as symptoms may not be apparent during clinical examinations while cerebral imaging may show signs of ipsilateral ischemic damage), clinicians have to answer the 2 fundamental questions: 1) what is the risk of the particular carotid lesion to cause stroke, distal emboli, or underperfusion? and 2) what is the balance of risks and benefits of an intervention in the context of the individual patient, taking into account clinical, physiological, imaging, and lesion characteristics (Figure 1).
Ideally, indicators that would put the individual at a greater risk for an impending stroke should be identified before the stroke disaster occurs. The treatment should be preventive rather than reactive and should be safe and long‑term effective.2,4
It is clear today that optimized medical therapy, although it may reduce or delay stroke risk, does not sufficiently prevent strokes in relation to carotid stenosis.2,4 Pharmacologic treatment may modify stroke‑prone “vulnerable” plaques and the “vulnerable blood” parameters insufficiently to abolish the increased stroke risk.5,6 Patients who develop symptoms or signs of cerebral damage whilst already on optimized medical therapy continue to join contemporary all‑comer carotid revascularization studies.2,4 Such patients should be revascularized before rather than in reaction to their irreversible cerebral neuronal loss and associated cognitive decline.
Evidence‑based medicine (EBM) points randomized clinical trials (RCTs) as the gold standard for demonstrating (or refuting) the benefits of a particular intervention. Yet, RCTs have important limitations of which 4 are particularly relevant today: 1) the null hypothesis (which presumes that there is no difference between treatments); 2) probability (with a 5% threshold being generally used to evaluate the null hypothesis); 3) generalizability (in clinical practice, the tested intervention is likely to be used in a far more heterogeneous population than the RCT population); and 4) resource implications (these are often prohibitively high limiting precise disease classifications with imaging, histological, clinical, and cognitive assessment data as well as an increasingly prohibitively high cost of conducting an RCT).7
The null hypothesis may be no longer relevant if there have been previous studies showing that a particular treatment has benefits in certain lesion types or patient cohorts. This, indeed, has been the case with several recent RCTs in cardiovascular medicine, ie, regarding the fate of the thrombus extraction strategy in acute thrombotic coronary artery occlusions (patients with proximal thrombotic lesions were typically treated outside randomization).
Randomizing patients who are a likely to benefit from an intervention is not ethical, because randomization requires uncertainty of the treatment effect. These patients typically receive intervention outside the RCT,8 and thus in many instances only those who are unlikely to benefit from the intervention get randomized.8 Indeed, today’s cardiovascular RCTs increasingly suffer from an “entry” bias that, in turn, substantially affects generalization of results. Real‑life all‑comer studies and registries have greater relevance to clinical practice at large. All‑comer registries are (in contrast to RCTs) naturally heterogeneous. They are thus more likely to identify the individual characteristics of those who are at a greater risk of developing clinical consequences of the pathology (if left untreated) or identify the responders to treatment.
So, EBM today is not just about RCTs. Interestingly, already at its roots, EBM defined itself as being “about integrating individual clinical expertise and the best external evidence” rather than being a “cookbook” clinical medicine. The “average” RCT patient may not exist in clinical practice or may be as rare as the tip of the Gaussian distribution. Today, more a precise disease classification and greater understanding of individual variations in disease pathology drive the development of targeted therapeutics.3 There is increasing understanding in vascular medicine that patient and disease characteristics matter—both in the clinical risks in relation to the disease and in response to treatment. Interventions presumed to be “futile” on the basis of an “average patient” response in studies with a substantial selection bias—or in studies that have enrolled unnaturally homogenous populations—may actually work very well for other patients with the disease.
Today, there is increasing evidence that the carotid plaque (along with the “vulnerable blood” properties) itself plays an important, mechanistic part in transforming a lesion from asymptomatic to symptomatic.5,6,9,10 Individual patient, lesion and disease characteristics form the very basis of contemporary clinical decision‑making in atherosclerotic carotid stenosis (Figure 1), consistent with the EBM original principle of integrating individual clinical expertise and the best external evidence.
In this issue of Polish Archives of Internal Medicine (Pol Arch Intern Med), a multispecialty team of stroke neurologists, angiologists, and vascular surgeons share with us their identification of clinical and imaging factors associated with the symptomatic status of carotid artery stenosis.11 This work, although it may lack the precision of plaque characteristics used in some other recent studies,5,6,9,12 is focused on very practical aspects of decision making.11 It thus adds importantly to the currently “hot” topic of answering the unmet need for risk stratification in clinically asymptomatic carotid artery stenosis,5,6,9,10,12 bearing in mind that what is not (for some individuals—not yet) manifested clinically may be already manifested on cerebral imaging.
The field of carotid artery disease, in regard to risk / benefit stratification, is no exemption from other fields in vascular medicine. Recently, another multispecialty work published in Pol Arch Intern Med13 identified several predictors of favorable clinical responses to the “condemned” treatment of renal artery stenosis revascularization. Identification of those patients with better blood pressure control and improved renal function (or halted deterioration) as a result of renal artery revascularization may now enable targeting the intervention to those who are likely to benefit from it.13 This is opposite to a simplistic “no intervention for anybody” approach—because of the statistical lack of an “average” benefit that may well have been driven by largely recruiting patients with functionally insignificant stenoses and / or kidney failure already too advanced to be reversible
The recent publications in the Pol Arch Intern Med11,13 are examples of work in progress that, ideally, requires further, prospective validation. This, however, may not be so easy, because it is well known (and not surprising) that patients who possess a significant risk feature gravitate towards intervention rather than getting randomized or observed to validate a risk prediction model.8 It is the duty of a clinician to apply the best contemporary evidence available (Figure 1) rather than passively wait for “further,” “stronger” evidence—that may or may not arrive with the “magic” of a large‑scale RCT and that, in order to meet recruitment targets, may well enroll subjects who are, a priori, known not to require the intervention or benefit from it. The challenge of clinical decision making should also include the fact that the “value” of an intervention (and any other treatments) may be dependent on the endpoint.14 The latter should always be one that relates to the patients’ physical health in the context of quality of life.14,15
In conclusion, the heterogeneity of treatment effects is a direct reflection of patient and disease diversity, responsiveness to treatment, vulnerability to adverse effects, and definition of a study endpoint.3,7 It is increasingly understood that heterogeneity is a key obstacle in EBM’s attempts to summarize medical practice within the framework of “averages.”7 A “mean” (whether a baseline value or measurement of treatment response) may not represent the population. This is particularly relevant if the cohort, whilst sharing one common attribute, is heterogeneous in its characteristics, which remain in a mechanistic relation to the disease or treatment response. Advances in medical research pursued by clinician‑scientists, exemplified by a series of recent publications in Pol Arch Intern Med,11,13 may rescue the clinicians and, more importantly, many of their patients from the stalemate of wrongly understanding EBM as the medicine of averages.
Rather than treating RCT “average patients”—who all too often differ from real life—or other statistical averages, clinicians need to look at the individual patient and their specific risk profile. Implementing patient‑specific characteristics11,13 to guide interventions in vascular medicine remains fully within the framework of “integrating individual clinical expertise and the best external evidence.” Thus decision making that, in contemporary clinical practice, integrates patient and lesion characteristics continues to be evidence‑based.
- Pearson J, Sipido KR, Musialek P, van Gilst WH. The Cardiovascular Research community calls for action to address the growing burden of cardiovascular disease. Cardiovasc Res. 2019; 115: e96‑e98. | Crossref
- Musialek P, Roubin GS. Double‑layer carotid stents: from the clinical need, through a stent‑in‑stent strategy, to effective plaque isolation… The journey toward safe carotid revascularization using the endovascular route. J Endovasc Ther. 2019; 26: 572‑577. | Crossref
- Blaus A, Madabushi R, Pacanowski M, et al. Personalized cardiovascular medicine today: a Food and Drug Administration/Center for Drug Evaluation and Research perspective. Circulation. 2015; 132: 1425‑1432. | Crossref
- Mazurek A, Borratynska A, Malinowski KP, et al. MicroNET‑covered stents for embolic prevention in patients undergoing carotid revascularisation: Twelve‑month outcomes from the PARADIGM study. EuroIntervention. 2020; 16: e950‑e952. | Crossref
- Hosseini AA, Simpson RJ, Altaf N, et al. Magnetic resonance imaging plaque hemorrhage for risk stratification in carotid artery disease with moderate risk under current medical therapy. Stroke 2017; 48: 678‑685. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION