Asystolic cardiac arrest with chest pain as initial features of eosinophilic granulomatosis with polyangiitis (Churg–Strauss syndrome)



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Asystolic cardiac arrest with chest pain as initial features of eosinophilic granulomatosis with polyangiitis (Churg–Strauss syndrome)
A 29‑year‑old man with late‑onset asthma, large nasal polyps, and a history of acute pancreatitis presented to the local hospital with new onset of retrosternal chest pain and concomitant dyspnea. His family history of cardiovascular diseases and sudden cardiac death (SCD) was noncontributory.
Electrocardiography revealed abnormal Q waves in leads II, III, and aVF without ST segment changes. Blood analysis showed an elevated level of troponin T (27 ng/l at the onset, with peak value of 276 ng/l; reference value, <14 ng/l) and N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) level of 152 pg/ml (reference value, <125 pg/ml). Coronary angiography only revealed slow‑flow in the unobstructed left anterior descending artery. Shortly after another episode of chest pain, the patient went into asystolic cardiac arrest (Figure 1A). After resuscitation, sinus rhythm with a heart rate of 100 bmp was restored. Electrocardiography demonstrated a transient ST‑segment elevation in anterior chest leads. Subsequent coronary angiography did not reveal any new findings (Figure 1B), and the patient was referred to our institute for potential implantation of a cardioverter‑defibrillator. Significant eosinophilia (1650/μl [reference range, 20–500/µl], 17.7% of peripheral white blood cell count) was not taken into account in the diagnostic work‑up.
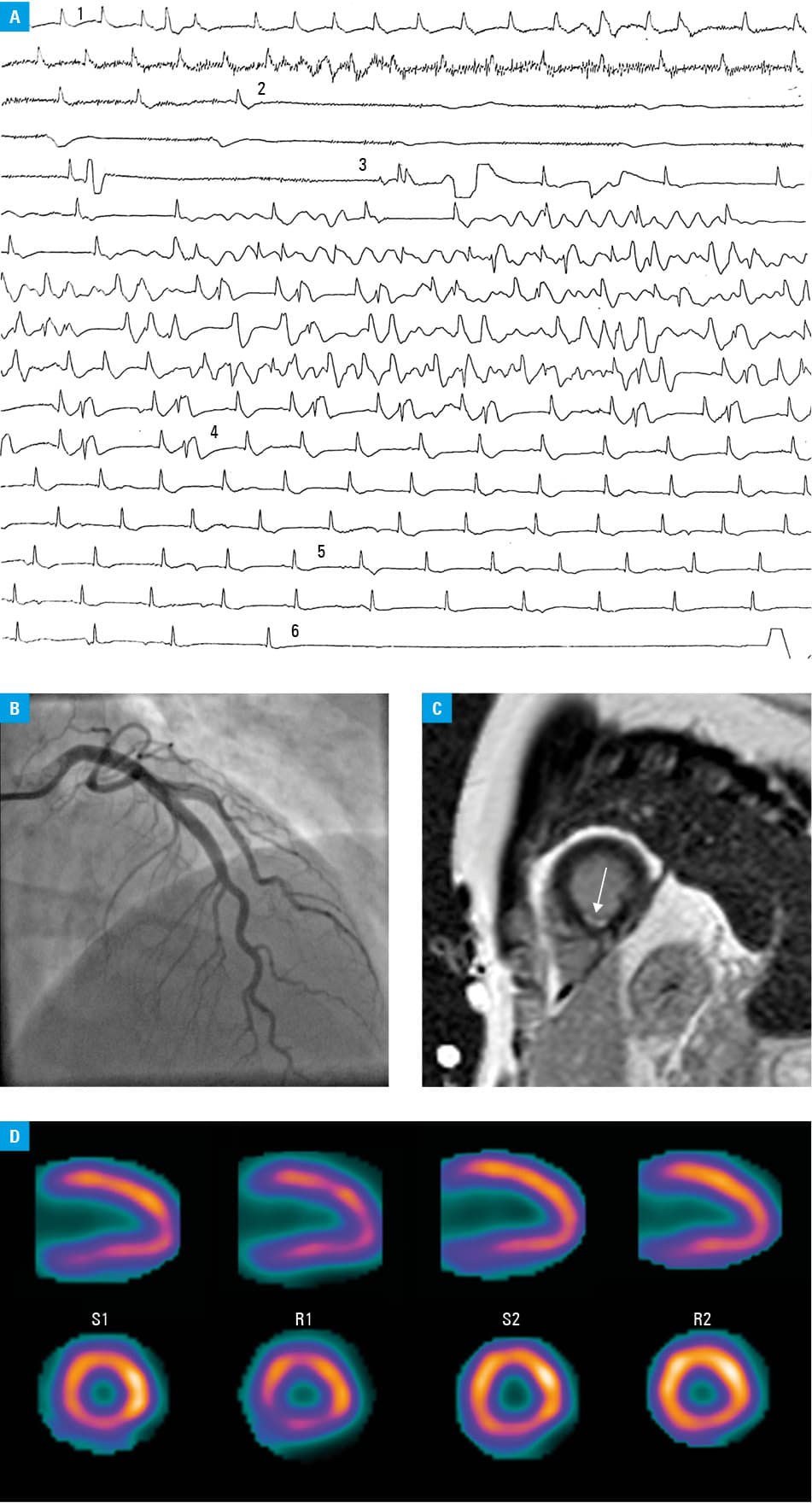
Since echocardiographic findings were insignificant, cardiac magnetic resonance imaging was performed, which showed a small focus of subendocardial delayed gadolinium enhancement in apical segments (Figure 1C). Stress perfusion cardiac scintigraphy demonstrated mild perfusion defect of the anterior, inferior, and infero‑septal walls with deterioration during the rest phase suggesting a pathology related to microvascular dysfunction (segments S1 and R1 on Figure 1D). In addition, antineutrophil cytoplasmic antibodies were negative.
Electrophysiology was performed for risk stratification of SCD, but no arrhythmias were induced. Based on the aforementioned findings and in accordance with the available criteria,1 eosinophilic granulomatosis with polyangiitis (EGPA) was diagnosed. Corticosteroid therapy was introduced, with 3 boluses of methyloprednisolone 500 mg every 2 days and oral prednisolone at the dose of 60 mg/d. Consequently, eosinophilia decreased to nearly 0% of peripheral white blood cell count with corresponding normalization of troponin T and NT‑proBNP levels. Given the reversible cause of cardiac arrest and excellent response to corticosteroids with uneventful recovery, the patient was not referred for implantation of a cardioverter‑defibrillator for secondary prevention of SCD. After 9 months of gradual reduction of prednisolone dosage, he was left on 7.5 mg daily. On fifth month, follow‑up scintigraphy showed significant improvement of perfusion in both rest and stress phases (segments R2 and S2 on Figure 1D). In 2‑year follow‑up, the patient remained asymptomatic.
Eosinophilic granulomatosis with polyangiitis, previously known as Churg–Strauss syndrome, is an autoimmune inflammatory disease of small and medium vessels. Cardiac involvement occurs in 60% of cases and is the main cause of mortality among patients with EGPA. It is more clinically overt in patients who are negative for antineutrophil cytoplasmic antibodies, as in the case of our patient, and usually involves myocarditis, pericarditis, coronary artery vasculitis, heart failure, and arrhythmias.2-5
Our case highlights that diagnosing EGPA can be challenging for physicians. Since all organs may be vulnerable to the effects of persistent eosinophilia alone, the differential diagnosis should include parasitic infections, atopic drug reactions, myeloproliferative disorders, and hypereosinophilic syndrome, which can be indistinguishable from EGPA in terms of clinical presentation and biomarker profile, especially in its early prodromal stage. Initially, eosinophilia might be misleadingly attributed to asthma and sinusitis, and consequently diagnosed separately from cardiac manifestation. However, the above‑mentioned findings of scintigraphy and the absence of atherosclerotic stenosis of large coronary arteries on cardiac magnetic resonance were highly suggestive of small‑vessel disease and thus allowed to link the significant eosinophilia and refractory late‑onset asthma with the acute, life‑threatening cardiac involvement.
Although arrhythmia as an initial feature of EGPA is rare, asystolic cardiac arrest has not been presented so far. In a patient with refractory asthma and a significant peripheral eosinophilia, EGPA should be considered, because only early initiation of corticosteroids can preserve cardiac function.
- Masi AT, Hunder GG, Lie JT, et al. The American College of Rheumatology 1990 criteria for the classification of Churg‑Strauss syndrome (allergic granulomatosis and angiitis). Arthritis Rheum. 1990; 33: 1094‑1100. | Crossref
- Fong C, Schmidt G, Cain N, et al. Churg‑Strauss syndrome, cardiac involvement and life threatening ventricular arrhythmias. Aust N Z J Med. 1992; 22: 167‑168. | Crossref
- Sharpley FA. Missing the beat: arrhythmia as a presenting feature of eosinophilic granulomatosis with polyangiitis. BMJ Case Rep. 2014; 2014: bcr2013203413. | Crossref
- McAleavey N, Millar A, Pendleton A. Cardiac involvement as the main presenting feature in eosinophilic granulomatosis with polyangiitis. BMJ Case Rep. 2013; 2013: bcr2013009394. | Crossref
- Sokołowska B, Szczeklik W, Włudarczyk A, et al. ANCA‑positive and ANCA‑negative phenotypes of eosinophilic granulomatosis with polyangiitis (EGPA): outcome and long‑term follow‑up of 50 patients from a single Polish centre. Clin Exp Rheumatol. 2014; 32: S41‑S47.
ARTICLE INFORMATION