Cushing syndrome and bone metastases as the manifestation of adrenocortical carcinoma



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Cushing syndrome and bone metastases as the manifestation of adrenocortical carcinoma
A 61‑year‑old woman was referred to an orthopedic clinic because of severe nontraumatic back pain. Computed tomography (CT) of the lumbosacral spine revealed vertebral body compression fractures in Th11 through L4, bone loss, and right adrenal tumor. Treatment with buprenorphine was initiated and the patient started using an orthopedic corset and a wheelchair. Additionally, the patient presented symptoms of Cushing syndrome (CS), that is, abdominal obesity with thin limbs, a round red face, thin skin, hypertension, diabetes requiring insulin therapy, without hirsutism.
Clinical symptoms and laboratory test results (increased cortisol levels without typical circadian rhythm at 26.1 μg/dl at 6 am and 29 μg/dl at 12 pm; decreased adrenocorticotropic hormone levels [<5 pg/ml]; and hypokalemia at 3.1 mmol/l [reference range, 3.8–5 mmol/l]) confirmed adrenocorticotropic hormone–independent CS. Abdominal CT detected a large right adrenal tumor, 60 × 47 × 51 mm in size, with heterogeneous contrast enhancement, delayed contrast washout, and vertebral body compression fractures (Figure 1A). Dual‑energy X‑ray absorptiometry of the lumbar spine and the femoral neck revealed low bone mass.
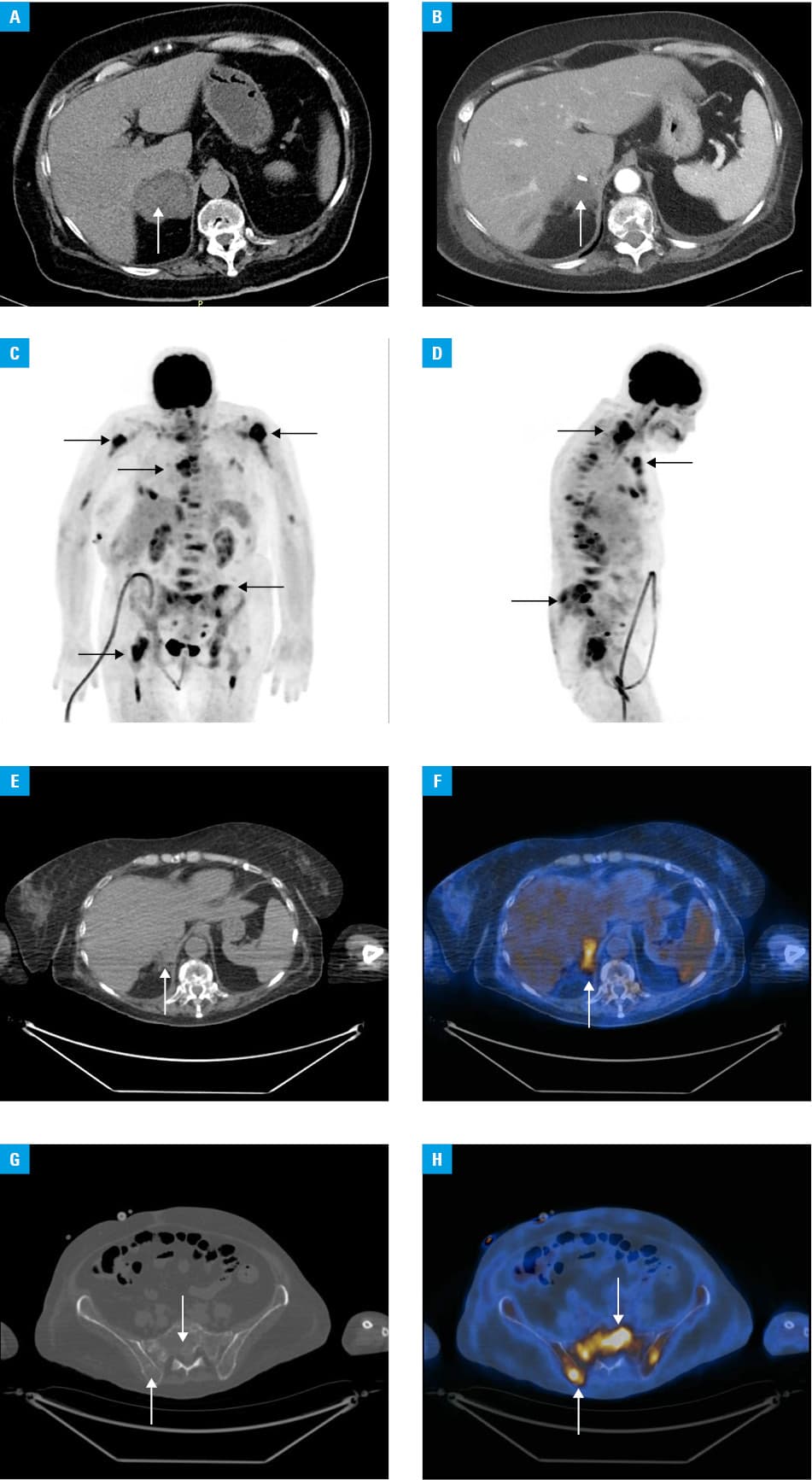
The patient was referred to the surgery department for adrenalectomy. The histological examination was remarkable for adenomatous hyperplasia of the adrenal cortex. Directly after surgery, clinically and hormonally persistent hypercortisolemia was observed. Thus, follow‑up abdominal and thoracic CT scans were performed. An irregular, hypodense lesion without contrast enhancement, 51 × 28 × 26 mm in size, at the postadrenalectomy site and osteolytic lesions in the thoracic vertebral body were visualized (Figure 1B). As the patient refused another surgery, metyrapone therapy was started and her condition improved. The third abdominal CT scan (performed after 4 weeks) presented the previously seen soft tissue lesion, with possible invasion of the surrounding tissues yet without any abnormalities in the lymph nodes, and multiple osteolytic lesions in bones. The second histological examination also did not confirm adrenocortical carcinoma (ACC) (Weiss score, 2/9). Due to inconclusive histological findings and the rarity of bone metastases in ACC, 18F‑fluorodeoxyglucose positron emission tomography–CT (18FDG‑PET/CT) was performed to search for another malignancy. The 18FDG uptake was observed in the postoperative site lesion (maximum standardized uptake value, 3.1) and generalized osteolytic skeletal lesions (maximum standardized uptake value, 5.2) (Figure 1C–1H). It did not reveal any metastases to the lymph nodes, lungs, and liver or any other malignancy. Diagnostic workup findings were strongly suggestive of ACC with bone metastases, which was further confirmed by surgical adrenal biopsy. Due to the apparently metastatic disease, mitotane therapy was initiated. Unfortunately, despite treatment, the patient died soon.
Adrenocortical carcinoma is a very rare condition (0.7–2 per 1 000 000 per year). About 50% to 60% of patients have clinical hormone excess, predominantly CS.1 Bone loss in CS leads to fractures in approximately 30% to 76% of patients, especially at the vertebral site.2 In such cases, CT makes the recognition of bone metastases difficult. Adrenocortical carcinoma is usually metastatic at the time of diagnosis. The lung and liver are the most common metastatic sites.1 Bone metastases are noted in up to 14% of patients with advanced ACC.3,4 The bone is the single metastatic site in only 9% of those patients.3
Although CT and magnetic resonance imaging represent basic modalities to evaluate the stage of ACC and enable adequate treatment, 18FDG‑PET/CT can help to localize all metastases. Nevertheless, despite typical clinical and radiological features, obtaining the histological confirmation of ACC remains a challenge and leads to delay in chemotherapy initiation.
- Fassnacht M, Dekkers OM, Else T, et al. European Society of Endocrinology Clinical Practice Guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2018; 179: G1‑G46. | Crossref
- van der Eerden AW, den Heijer M, Oyen WJ, et al. Cushing’s syndrome and bone mineral density: lowest Z scores in young patients. Neth J Med. 2007; 65: 137‑141.
- Berruti A, Libè R, Laganà M, et al. Morbidity and mortality of bone metastases in advanced adrenocortical carcinoma: a multicenter retrospective study. Eur J Endocrinol. 2019; 180: 311‑320. | Crossref
- Libé R, Borget I, Ronchi CL, et al; ENSAT network. Prognostic factors in stage III‑IV adrenocortical carcinomas (ACC): an European Network for the Study of Adrenal Tumor (ENSAT) study. Ann Oncol. 2015; 26: 2119‑2125. | Crossref
ARTICLE INFORMATION