Squamous cell carcinoma of the prostate with concomitant hypercalcemia and normal serum prostate-specific antigen levels



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Squamous cell carcinoma of the prostate with concomitant hypercalcemia and normal serum prostate-specific antigen levels
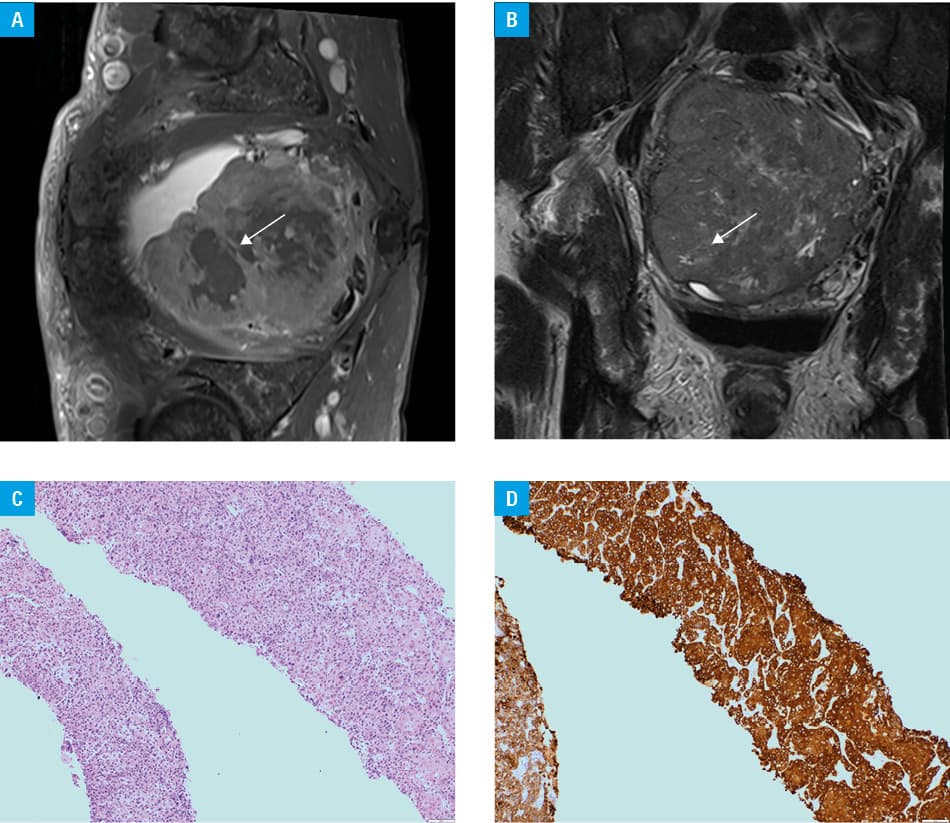
In April 2020, a 73‑year‑old man was referred to the hospital because of urinary tract infection accompanied by marked leukocytosis (31.5 × 103/μl) and thrombocytosis (505 × 103/μl). Laboratory workup revealed parathormone‑independent hypercalcemia, which subsided after a single dose of pamidronate. Computed tomography of the abdomen and pelvis showed a markedly enlarged prostate gland (93 × 98 × 103 mm) without enlarged lymph nodes in the pelvis or signs of bone destruction. The prostate‑specific antigen (PSA) level was within the reference range (0.93 ng/ml). The myelogram and histological examination of trephine biopsy were unremarkable. Fluorodeoxyglucose positron emission tomography–computed tomography (FDG‑PET/CT) indicated an active metabolic process, primarily proliferative, in the prostate (standardized uptake value, 40) with the involvement of the pelvic lymph nodes. Magnetic resonance imaging (MRI) of the pelvic cavity performed after 8 weeks (Figure 1A and 1B) showed a huge tumor arising from the prostate, infiltrating the bladder, and compressing the rectum, with numerous bone metastases metabolically inactive on FDG‑PET/CT. The diagnosis of squamous cell carcinoma (SCC) of the prostate was established based on ultrasound‑guided prostate biopsy (Figure 1C and 1D). After disqualification from cystoprostatectomy due to poor prognosis of the disseminated disease, the patient was started on palliative intensity‑modulated radiation therapy (IMRT) for the treatment of the tumor and metastatic pelvic lymph nodes (5 × 4 Gy). It presented good early tolerance and relieved lower urinary tract symptoms (LUTS). Lung metastases were diagnosed in the following 4 months. A poor clinical condition precluded the use of chemotherapy and the patient received hospice care for 6 months since the time of the diagnosis.
Squamous cell carcinoma of the prostate is a rare, aggressive cancer, frequently diagnosed in the stage of the metastatic disease, with a median overall survival of 12 months.1,2 Its clinical presentation based on 22 cases described in the literature includes LUTS, acute urinary retention, urinary tract infection, hematuria, and bone pain related to metastases. Sites of metastases (reported in 56% of cases) include bones, lungs, the liver, and lymph nodes.2 Squamous cell carcinoma of the prostate typically cannot be detected by PSA screening. Primary surgical intervention (prostatectomy, cystoprostatectomy with pelvic lymphadenectomy) may improve the outcome in patients with locoregional disease. There are limited data concerning radiation therapy, and chemotherapy in disseminated disease that has been implemented without long‑term response.2
The presented case shows an unusual clinical course of a patient with disseminated SCC of the prostate and hypercalcemia. Typically for SCC of the prostate, the lack of increased PSA levels made the differential diagnosis of prostate cancer and the exclusion of bladder cancer infiltrating the prostate much more difficult. As previously shown, the FDG uptake on PET/CT of the lesion was high.3,4 However, bone metastases were not visualized on FDG‑PET/CT. Of note, MRI turned out to be much more useful for the detection of bone metastases. The late presentation of the patient and the aggressive course of cancer precluded radical treatment. Although IMRT effectively controlled the irradiated tumor, it could not manage the disseminated disease and improve the overall survival without chemotherapy. Despite the poor prognosis, IMRT improved the patient’s quality of life by relieving LUTS.
- Moskovitz B, Munichor M, Bolkier M, Livne PM. Squamous cell carcinoma of the prostate. Urol Int. 1993; 51: 181‑183. | Crossref
- Malik RD, Dakwar G, Hardee ME, et al. Squamous cell carcinoma of the prostate. Rev Urol. 2011; 13: 56‐60.
- Dong A, Zuo C, Lu J, Wang Y. Squamous cell carcinoma of the prostate with strong FDG uptake on PET/CT. Clin Nucl Med. 2014; 39: 650‑652.
- Kara Gedik G, Yavas G, Akand M, et al. Fluorodeoxyglucose positron emission tomography/computed tomography imaging of a patient with squamous cell carcinoma of prostate. Case Rep Med. 2014; 2014: 860570. | Crossref
ARTICLE INFORMATION