Atypical course of anaplastic large cell lymphoma with positive anaplastic lymphoma kinase



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Atypical course of anaplastic large cell lymphoma with positive anaplastic lymphoma kinase
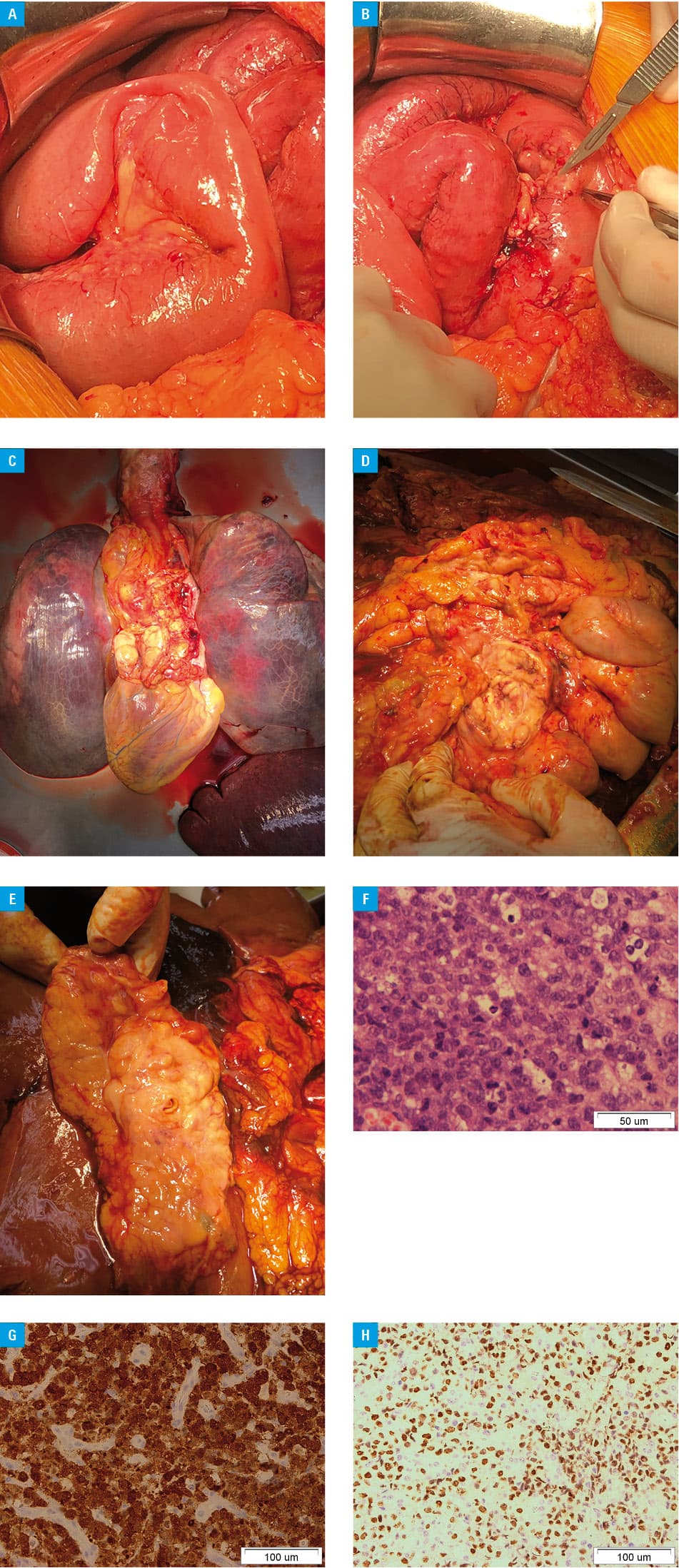
A 29‑year‑old man was admitted to hospital due to severe weakness, ascites, loss of appetite, bile vomiting, stool retention, insomnia, and excessive sweating that had been increasing for 3 weeks. Five months earlier, the patient had already been hospitalized for suspected lymphoma manifested by fever and occasional cough, with no symptoms of infection; however, he had refused further diagnostic workup and left the hospital at his own request. Currently, his condition rapidly deteriorated. On admission, the patient was in poor clinical condition with symptomatic ileus. Laboratory tests revealed mild anemia (hemoglobin level, 13 g/dl), leukocytosis (white blood cell count, 13.4 × 103/µl), hypoproteinemia (total protein level, 5.2 g/dl), hypercreatininemia (creatinine level, 1.79 mg/dl), and elevated serum levels of C‑reactive protein (77 mg/l; reference range, <10 mg/l) and procalcitonin (1.53 ng/ml; reference range, <0.05 ng/ml). Computed tomography showed extensive infiltration in the abdominal fat tissue, ascites, lymphadenopathy, thickening of the small intestine walls, and hydrothorax. Due to the worsening clinical condition, urgent laparotomy was performed. Disseminated tumorous infiltration of the peritoneal cavity, involving the mesenterium, transverse mesocolon, small intestine, and retroperitoneal space was recognized (Figure 1A and 1B). Dissection of the retroperitoneal space and decompression of the intestine was impossible due to the disease dissemination. Despite intensive treatment, the patient died 1 hour after surgery due to septic shock. In autopsy, disseminated lymphoma infiltration in the whole thoracic and abdominal cavities was noted (Figure 1C–1E). Histological findings showed anaplastic large cell lymphoma with positive anaplastic lymphoma kinase (ALK+ ALCL); the Ki‑67 index was 100%. Immunohistochemical examination revealed positive staining for CD2, CD30, epithelial membrane antigen, multiple myeloma oncogene 1, activin receptor–like kinase 1, and c‑myc protein as well as negative staining for CD4, CD3, CD23, CD10, CD20, creatine kinase, bcl‑2 and bcl‑6 protein, and cyclin D1 (Figure 1F–1H).
The first description of ALK+ ALCL was published by Stein et al1 in 1982, and it defined this malignancy as a peripheral T‑cell lymphoma usually consisting of large neoplastic cells with abundant cytoplasm and pleomorphic, often horseshoe‑shaped nuclei, with a translocation involving the ALK gene, and expression of ALK protein and CD30.1,2 Anaplastic large cell lymphoma is a chemo‑sensitive disease with overall survival of 70% to 90%.3 It represents approximately 3% of large cell non‑Hodgkin lymphomas.2 Anaplastic lymphoma kinase–positive ALCL most commonly occurs in the second and third decades of life (male / female ratio, 6.5). The majority (50%–70%) of patients present with stage III–IV disease with peripheral (mediastinal and / or abdominal) lymphadenopathy, systemic B symptoms (54%–75%), and extranodal involvement (60%), such as that of skin (8%–21%), soft tissues (17%–21%), lungs (6%–13%), liver (3%–17%), and spleen (8%–21%), as well as bone marrow (up to 16%).3 Intestinal location of ALCL is very rare. Only a few case reports have been published worldwide.4
In the presented case, the course of ALCL was fatal due to massive dissemination and ileus caused by intra‑abdominal location. Systemic therapy was not possible due to the patient’s clinical condition. Despite the relatively good prognosis of ALK+ ALCL (5‑year failure‑free survival is 60% and 5‑year overall survival is 70%), in this case, premature discontinuation of the diagnostic workup resulted in lethal complications.5 This case suggests that early diagnosis, before the development of fatal complications, might improve prognosis in ALK+ ALCL.
- Stein H, Mason DY, Gerdes J, et al. The expression of the Hodgkin’s disease associated antigen Ki‑1 in reactive and neoplastic lymphoid tissue: evidence that Reed‑Sternberg cells and histiocytic malignancies are derived from activated lymphoid cells. Blood. 1985; 66: 848‑858. | Crossref
- Ferreri AJ, Govi S, Pileri SA, Savage KJ. Anaplastic large cell lymphoma, ALK‑positive. Crit Rev Oncol Hematol. 2012; 83: 293‑302. | Crossref
- Tsuyama N, Sakamoto K, Sakata S, et al. Anaplastic large cell lymphoma: pathology, genetics, and clinical aspects. J Clin Exp Hematop. 2017; 57: 120‑142. | Crossref
- Cao Q, Liu F, Li S, et al. Primary rare anaplastic large cell lymphoma, ALK positive in small intestine: case report and review of the literature. Diagn Pathol. 2016; 11: 83‑91. | Crossref
- Savage KJ, Harris NL, Vose JM, et al. ALK- anaplastic large‑cell lymphoma is clinically and immunophenotypically different from both ALK+ ALCL and peripheral T‑cell lymphoma, not otherwise specified: report from the International Peripheral T‑Cell Lymphoma Project. Blood. 2008; 111: 5496‑5504. | Crossref
ARTICLE INFORMATION