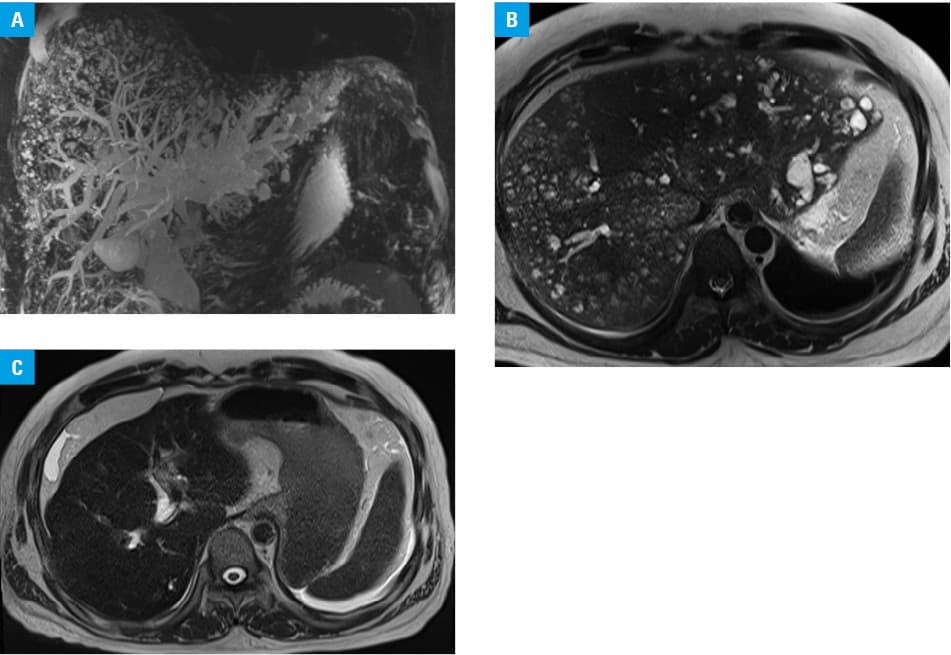
A previously healthy 33‑year‑old man presented to the emergency department due to fever, abdominal pain, and jaundice. He was immediately hospitalized based on a diagnosis of acute cholangitis and sepsis. Blood tests showed severe inflammation, high levels of hepatobiliary enzymes, and predominantly direct bilirubin. Magnetic resonance imaging after admission (Figure 1A and 1B) indicated dilated intrahepatic and extrahepatic bile ducts and multiple cystic lesions present diffusely throughout the liver. Based on clinical symptoms and blood biochemistry findings, acute gallstone cholangitis was considered. In particular, a high level of alkaline phosphatase (702 IU/l; reference range, 115–359 (IU/l) on biochemical findings seemed to suggest cholestasis caused by bile duct obstruction. Imaging findings (dilatation of intrahepatic and extra bile ducts, and calculi in the extrahepatic bile ducts) also suggested acute gallstone cholangitis. Immediately after admission, infusion of sulbactam / cefoperazone was started. Furthermore, we performed endoscopic retrograde cholangiography. Markedly dilated bile ducts with stones were revealed. No biliary stricture nor any communication between bile duct and cystic lesions was found on endoscopic retrograde cholangiopancreatography. Endoscopic stone removal was performed using a balloon catheter after sphincterotomy. After treatment, the cholangitis improved over time. The patient was discharged with improved symptoms. Magnetic resonance imaging conducted 3 months later revealed no evidence of intrahepatic or extrahepatic bile duct dilatation. Multiple cystic lesions in the liver all disappeared (Figure 1C). In a differential diagnostic workup, findings of multiple cystic lesions in the liver on magnetic resonance imaging suggested Caroli disease, with von Meyenburg complex as an underlying pathology.1,2 Caroli disease involves congenital cystic dilatation of the peripheral intrahepatic bile ducts. Diffuse lesions occur in bilateral liver lobes in many cases. Caroli disease is a rare autosomal recessive disorder that is known to be complicated by autosomal recessive polycystic kidney disease. Nevertheless, no renal lesion was found in this case. In contrast, von Meyenburg complex is characterized by bile duct hamartomas containing innumerable diffuse multiple cystic lesions. Both of those findings are similar to findings obtained in this patient, but they are not conditions that improve with bile duct drainage. Multiple liver abscesses were also differentiated. However, multiple cystic lesions disappeared immediately after stone removal. This clinical course was regarded as atypical for treatment of liver abscesses. In this case, peripheral bile ducts in the liver were considered to show cystic dilatation due to biliary obstruction. According to the classifications of intrahepatic cystic dilatation and related diseases, these findings were consistent with dilatation of the intrahepatic biliary ducts without the Meyenburg complex.3 To date, no case of acute cholangitis showing similar imaging has been reported in the literature. It is considered a very rare condition. In fact, it remains unclear why bile ducts exhibit such a peculiar morphology. However, the pathological findings in this case should be understood as a differential diagnosis of multiple intrahepatic cystic lesions.
- Ozlem Y, Yusuf B. Clinical characteristics of Caroli’s disease. World J Gastroenterol. 2007; 13: 1930‑1933. | Crossref
- Pech L, Favelier S, Falcoz MT, et al. Imaging of Von Meyenburg complexes. Diagn Interv Imaging. 2016; 97: 401‑409. | Crossref
- Longmire WP Jr, Mandiola SA, Gordon HE. Congenital cystic disease of the liver and biliary system. Ann Surg. 1971; 174: 711‑726. | Crossref
ARTICLE INFORMATION