Exercise test in patients with asymptomatic aortic stenosis: clinically useful or not?
Key words: asymptomatic aortic stenosis, β-blockers, exercise test



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Exercise test in patients with asymptomatic aortic stenosis: clinically useful or not?
Introduction: Aortic valve replacement (AVR) is recommended for symptomatic patients with severe aortic stenosis (AS). In asymptomatic AS (AAS), exercise testing (ET) is recommended; however, it remains controversial.
Objectives: The aim of our study was to assess the importance of ET in patients with AAS.
Patients and methods: A total of 89 patients with AAS (53 men; mean [SD] age, 59.5 [11.7] years) underwent 244 symptom‑limited ETs.
Results: All ETs were clinically negative. During the median (interquartile range) follow‑up of 22 (12) months, 39 patients (22 men) developed symptoms (the AVR group). This group was compared with 50 asymptomatic non‑AVR patients. In the multivariable Cox analysis, the maximal heart rate during ET less than 85% of age- and sex‑adjusted maximal predicted heart rate (THR less than 85%) was related to AVR (P = 0.01). After adjusting for the use of β-blockers, this was not significant (P = 0.08). In the β-blocker subgroup, the THR less than 85% was significantly related to AVR in the univariable Cox analysis (hazard ratio, 2.2; 95% CI, 1.07–4.9; P = 0.03) and after adjusting for age (P = 0.047). This relationship was not observed in patients who did not receive β-blockers.
Conclusions: In patients with AAS, ET is safe; however, in our study group, the results were not crucial in making a decision to perform AVR. Patients treated with β-blockers who did not achieve 85% of predicted maximal heart rate had a higher probability of AVR. The influence of the use of β-blockers on the decision to perform AVR in this patient population warrants further revision.
What's new?
We assessed the clinical value of exercise test in patients with asymptomatic aortic stenosis. We found that in this population, exercise test is safe, but its value in the decision‑making process for valve replacement in our study group was low. We also propose a new clinical parameter that may be an equivalent of aortic stenosis symptoms—inability to achieve 85% of age‑adjusted maximal heart rate during exercise, especially in patients treated with β-blockers. Those who were treated with β-blockers and did not achieve 85% of predicted maximal heart rate had a higher probability of aortic valve replacement. The influence of treatment with β-blockers on the decision to replace the aortic valve in this small group of patients warrants further revision.
Introduction
Aortic stenosis (AS) is one of the most common heart valve diseases in developed countries. Studies investigating the natural history of AS in adults show that as stenosis increases, compensatory mechanisms fail and symptoms, that is, dyspnea, angina, syncope, and arrhythmias develop.1-4 Once the symptoms develop, the prognosis worsens.5,6 Aortic valve replacement (AVR), either surgical or with the use of a transcatheter, is recommended by current guidelines for symptomatic patients with severe AS.3,4 In asymptomatic patients with AS (AAS) and preserved left ventricular (LV) function defined as ejection fraction (EF) above 50%, the benefit of prophylactic AVR is still unproven and the optimal timing of the intervention remains controversial.3-12 International guidelines recommend exercise testing (ET) to unmask pseudo‑asymptomatic patients and those without self‑reported symptoms. In the past, ET was contraindicated in patients with severe AS due to risk of life‑threatening complications.3,4 Nowadays, ET is still absolutely contraindicated in patients with symptomatic severe AS. As studies over the past 15 years have shown, in patients with AAS, ET supervised by an experienced cardiologist is safe, and based on the guidelines of the European Society of Cardiology and the American College of Cardiology / the American Heart Association, it can be prognostically useful.13-17 In practice, the use of ET in patients with AAS is controversial and varies among practicing clinicians.15,16,18
The aim of our study was to assess the safety and tolerability of ET in patients with severe AAS and to answer the question if standard ET is still of important clinical value in this group of patients.
Patients and methods
We prospectively included 120 consecutive patients from the Outpatient Valve Disease Department with a diagnosis of severe AAS. Severe AS was defined as the aortic valve area of 1 cm2 or less, mean transvalvular pressure gradient of 40 mm Hg or greater, and EF of more than 50%. The inclusion criterion was the absence of symptoms—major: dyspnea, angina pectoris, syncope, and minor: dizziness, weakness, fatigue, exercise intolerance. Exclusion criteria were as follows: predominant aortic regurgitation or more than mild mitral / tricuspid regurgitation / stenosis, history of coronary artery disease (myocardial infarction, coronary artery bypass graft, percutaneous coronary intervention), a comorbid disease associated with symptoms that could interfere with clinical evaluation and preclude ET (ie, uncontrolled hypertension, disabilities). Hypertension was defined as a previous diagnosis established by a physician (with medications) or systolic blood pressure values of 140 mm Hg or greater or systolic blood pressure values of 90 mm Hg or greater during 2 visits.18 Diabetes was defined as a previous diagnosis established by a physician (with medications) or fasting blood glucose level of 7 mmol/l or greater in 2 or more blood samples.18
Finally, absence of symptoms was confirmed in 96 patients. After a detailed examination and history taking, 24 patients were classified as symptomatic. One patient was excluded from the study after the first test and 6 patients refused to participate in the study and did not consent to AVR, if necessary. A total of 89 patients who diagnosed as true AAS agreed to participate in the study. The group included 36 women and 53 men. The mean (SD) age was 59.5 (11.7) years (range, 25–77 years).
All patients were informed about the procedures, benefits, and risks involved in participating in the study. Informed consent was obtained from each patient and the study protocol conformed to the 1975 ethical guidelines of the Declaration of Helsinki as reflected by the a priori approval of the institution’s bioethical committee.
Patients were followed every 6 months (symptom assessment; echocardiography, and ET in asymptomatic patients). The follow‑up was stopped at predefined time (December 31, 2017) and the maximal follow‑up was defined as 36 months.
Transthoracic echocardiography
The standardized examination included transthoracic echocardiograms. The severity of AS, LV wall thicknesses, chamber dimensions, and EF were measured according to the current European and United States guidelines.
Exercise testing
A symptom‑limited ET was performed using an electrical bicycle monitored by a cardiologist, according to the recommendations.19 Every minute, patients were asked about their exhaustion (we used the modified 0–10 Borg scale). The initial workload was 50 W with a gradual increase of 50 W every 3 minutes. The ET was conducted until the patient exhaustion (ie, score 7 on the modified Borg scale). Target heart rate (THR) was calculated as 220 – age. The submaximal heart rate corresponded to 85% of this value.
The test was stopped in case of: patient’s request to finish the test, significant breathlessness and / or chest pain, systolic blood pressure fall greater than 20 mm Hg, significant increase of ventricular ectopy (couplets, ventricular tachycardia), supraventricular tachycardia, the onset of atrial flutter / fibrillation, systolic blood pressure of 250 mm Hg or greater, or diastolic blood pressure of 115 mm Hg or greater, significant ST‑segment depression (>4 mm) or ST‑segment elevation, or when the patient achieved 100% of THR.
To distinguish physiological and symptomatic breathlessness, we verified the presence of additional symptoms such as inability to speak, facial pallor, distress.
The ET was considered clinically positive if symptoms of AS occurred or if the patient stopped prematurely due to limiting breathlessness, dizziness, or systolic blood pressure drop greater than 20 mm Hg during exercise. The end point was defined as the decision to perform AVR.
Statistical analysis
Statistical analysis was performed using SPSS, version 11.0 (IBM, Chicago, Illinois, United States). Values are given as mean (SD) for continuous variables and as percentages for categorical variables. The data were tested for normality by the Kolmogorov–Smirnov test. The groups were compared by the unpaired t test, the χ2 test, and the Mann–Whitney test. Correlates of the end point were identified by multivariable Cox regression models and presented as hazard ratio and 95% CIs. In multivariable analysis, we included the parameters that achieved P less than 0.1 in univariable analysis, not more than 4. In univariable analysis more than 4 variables had P less than 0.1. It is well known (and clearly seen in our results) that age was the strongest parameter related to AVR so it was used as reference. Variables such as hypertension, hyperlipidemia, and statin use were strongly related to age, which we verified in the first place. These variables became not significant in multivariable analysis after adjusting for age. Since peak velocity, peak aortic gradient, and mean aortic gradient are mathematically related to each other, we only included peak aortic gradient, which is most frequently used in literature. The results of ET, that is, exercise workload in metabolic equivalent tasks and heart rate, are strongly age dependent; however, since the percentage of THR and THR less than 85% are not, we included one of them.
Results
A history of hypertension was noted in 56 patients, 26 patients had dyslipidemia, and 13 were diabetic. The median (interquartile range) follow‑up was 22 (11–36) months. All patients finished and survived the follow‑up period. During this time, 39 out of 89 patients, 17 women and 22 men, developed symptoms (it was recorded during periodic visits before the next ET) and the decision to perform AVR (the AVR group) was made by the Heart Team.
The details of follow‑up are presented in Figure 1. We performed 244 tests (Table 1). No significant differences were observed between consecutive tests performed every 6 months.
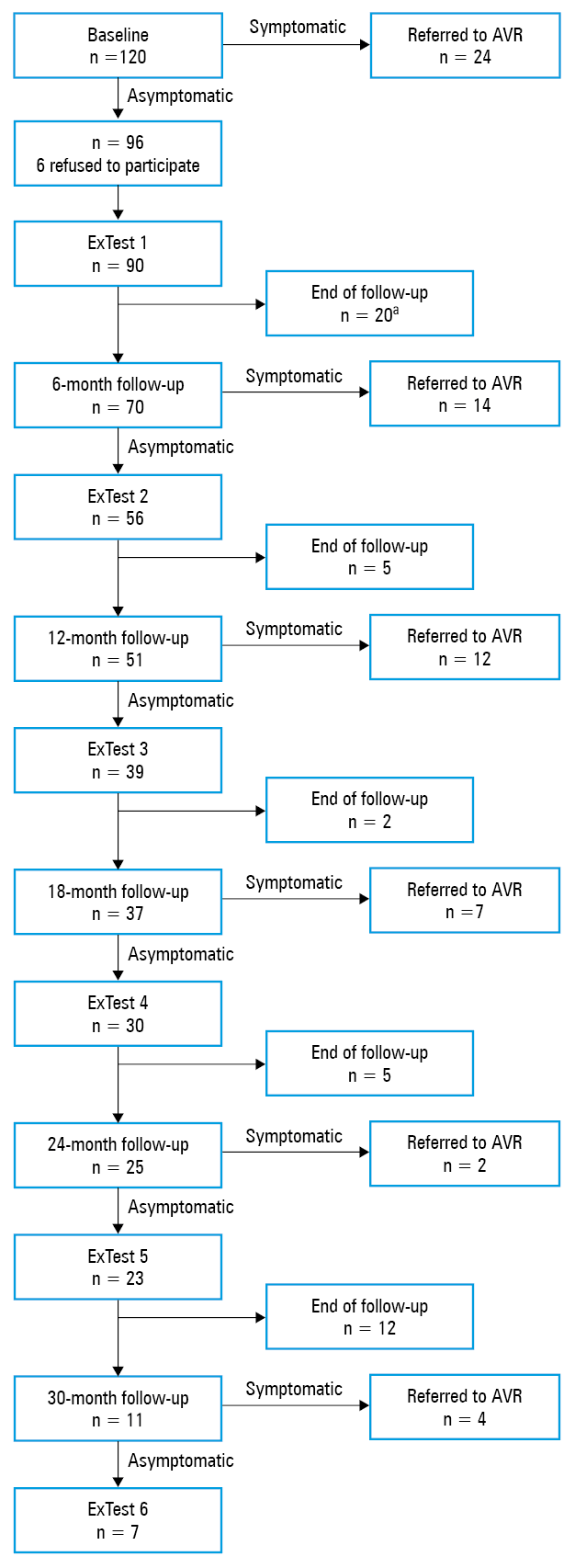
a One patient was excluded before the second test because he hid the symptoms during examination before the first exercise test. The test was asymptomatic.
Abbreviations: AVR, aortic valve replacement; ExTest, exercise test
Parameter | Test 1 (n = 89) | Test 2 (n = 56) | Test 3 (n = 39) | Test 4 (n = 30) | Test 5 (n = 23) | Test 6 (n = 7) |
Data are presented as mean (SD) unless otherwise indicated.
Abbreviations: BP, blood pressure; ET, exercise test; HR, heart rate; HRR, heart rate recovery; MET, metabolic equivalent task; THR, target heart rate; others, see Figure 1 | ||||||
Time, min | 6.9 (2.2) | 6.9 (2.4) | 7 (2.1) | 7.1 (2) | 7.3 (2.1) | 7.5 (2) |
Exercise capacity, METs | 6.6 (1.6) | 6.4 (1.5) | 6.2 (1.1) | 6.6 (0.9) | 6.6 (1.4) | 6.7 (0.9) |
Pre‑ET HR, bpm | 75 (11) | 77 (15) | 76 (14) | 79 (13) | 76 (11) | 81 (13) |
Peak HR, bpm | 140 (17) | 143 (18) | 142 (13) | 144 (17) | 148 (15) | 152 (19) |
THR, % | 89 (8) | 89 (7) | 90 (7) | 89 (8) | 91 (6) | 90 (4) |
Patients with THR <85%, n (%) | 29 (32.6) | 10 (20) | 7 (17.9) | 8 (33.3) | 3 (15) | 1 (14.3) |
HRR, bpm | 42 (16) | 42 (11) | 43 (11) | 48 (23) | 45 (17) | 42 (9) |
Pre‑ET systolic BP, mm Hg | 129 (13) | 126 (15) | 128 (14) | 127 (17) | 130 (16) | 120 (15) |
Pre‑ET diastolic BP, mm Hg | 80 (11) | 81 (9) | 78 (17) | 82 (11) | 81 (10) | 77 (10) |
Peak systolic BP, mm Hg | 182 (24) | 187 (26) | 183 (21) | 181 (24) | 180 (22) | 179 (20) |
Peak diastolic BP, mm Hg | 96 (13) | 96 (13) | 100 (12) | 93 (24) | 95 (14) | 93 (12) |
All tests were finished because of patients fatigue (7/10 in the Borg scale) or achievement of 100% of THR and were clinically negative, without blood pressure fall or complex arrhythmias.
The AVR group was compared with 50 patients from the non‑AVR group (Table 2). Patients who remained asymptomatic were younger, had longer mean follow‑up time and less significant AS, less often had hypertension, and more often did not receive any medications.
Parameter | AVR (n = 39) | Non‑AVR (n = 50) | P value | |
Data are presented as number (percentage) of patients or mean (SD) unless otherwise indicated.
Abbreviations: ACE, angiotensin converting enzyme; AVA, aortic valve area; EF, ejection fraction; IQR, interquartile range; IVSD, interventricular septum diameter; LVDD, left ventricular diastolic diameter; LVM, left ventricular mass; LVMI, left ventricular mass index; LVSD, left ventricular systolic diameter; PAG, peak aortic gradient; PWD, posterior wall diameter; Vmax, peak velocity; xAG, mean aortic gradient; others, see Figure 1 | ||||
Age, y | 65.2 (7.5) | 54.9 (12.5) | <0.001 | |
Sex | Male | 22 (56) | 31 (62) | 0.66 |
Female | 17 (44) | 19 (38) | ||
Hypertension | 30 (77) | 28 (56) | 0.046 | |
Diabetes | 6 (15) | 7 (14) | 0.99 | |
Hyperlipidemia | 21 (54) | 14 (28) | 0.02 | |
No treatment | 5 (13) | 20 (40) | 0.005 | |
β-Blockers | 28 (72) | 17 (34) | 0.001 | |
ACE inhibitors | 17 (44) | 19 (38) | 0.66 | |
Diuretics | 13 (33) | 10 (20) | 0.22 | |
Statins | 23 (59) | 19 (38) | 0.06 | |
Follow‑up, mo, median (IQR) | 17 (9–25) | 36 (13–36) | 0.001 | |
LVDD, mm | 43.7 (6.5) | 45.7 (6.9) | 0.17 | |
LVSD, mm | 27.2 (4.7) | 28.8 (4.6) | 0.12 | |
IVSD, mm | 14.7 (2.4) | 13.5 (2.6) | 0.03 | |
PWD, mm | 11.2 (2.3) | 10.9 (2.1) | 0.52 | |
LVM, g | 263 (95) | 257 (91) | 0.77 | |
LVMI, g/m2 | 138 (46) | 133 (40) | 0.56 | |
EF, % | 68 (4) | 68 (4) | 0.89 | |
AVA, cm2 | 0.8 (0.2) | 0.9 (0.2) | 0.11 | |
Vmax, m/sec | 4.8 (0.7) | 4.3 (0.2) | 0.02 | |
PAG, mm Hg | 88 (24) | 77 (20) | 0.02 | |
xAG, mm Hg | 52 (16) | 44 (15) | 0.03 | |
The comparison of the first tests performed in patients who underwent AVR with the non‑AVR group showed that the AVR group had lower exercise capacity in METs and lower heart rate during maximal effort compared with the non‑AVR group. This was mostly caused by the age differences. Patients in the AVR group more frequently became fatigued before they reached 85% of age‑adjusted THR (Table 3).
Parameter | AVR patients (n = 39) | Non‑AVR patients (n = 50) | P value |
Data are presented as mean (SD) unless otherwise indicated.
| |||
Exercise duration, min | 6.3 (2.2) | 7.3 (2.7) | 0.14 |
Exercise capacity, METs | 6.2 (1.5) | 6.9 (1.6) | 0.04 |
Pre‑ET HR, bpm | 73 (10) | 77 (11) | 0.05 |
Peak HR, bpm | 133 (14) | 145 (17) | 0.001 |
THR, % | 87 (8) | 90 (8) | 0.09 |
THR <85%, n (%) | 17 (43.5) | 12 (24) | 0.04 |
HRR bpm | 40 (10) | 44 (19) | 0.29 |
Pre‑ET systolic BP, mm Hg | 130 (13) | 128 (13) | 0.43 |
Pre‑ET diastolic BP, mm Hg | 78 (6) | 81 (14) | 0.29 |
Peak systolic BP, mm Hg | 181 (23) | 183 (24) | 0.59 |
Peak diastolic BP, mm Hg | 94 (13) | 97 (12) | 0.33 |
In the univariable Cox analysis, 85% of age‑adjusted THR was significant (Table 4). It might suggest a new clinical parameter, an equivalent of AS symptoms, that is, inability to achieve 85% of age‑adjusted THR during exercise. However, after adjustment for the use of β-blockers, this was not significant (P = 0.08).
Variable | Hazard ratio (95% CI) | P value |
Cox univariable analysis | ||
Age | 1.08 (1.04–1.1) | <0.001 |
PAG | 1.02 (1.009–1.037) | 0.002 |
β-Blockers | 2.8 (1.4–5.7) | 0.003 |
THR <85% | 2.27(1.2–4.3) | 0.01 |
Cox multivariable analysis | ||
Age | 1.07 (1.026–1.1) | 0.001 |
β-Blockers | 2.5 (1.23–5.1) | 0.01 |
PAG | 1.02 (1.003–1.036) | 0.02 |
The analysis of patients treated and not treated with β-blockers separately showed interesting results. Out of 45 patients treated with β-blockers, 28 became symptomatic, 16 (57%) of them did not reach 85% of THR. Out of the other 17 asymptomatic patients on β-blockers, only 5 (29%) did not achieve 85% of THR. In this β-blocker subgroup, THR of less than 85% was significantly related to AVR in the univariable Cox analysis (hazard ratio, 2.2; 95% CI, 1.07–4.9; P = 0.03). This parameter was still significant after adjusting for age (P = 0.047). This relationship was not observed in the group of 44 patients who did not receive β-blockers. A total of 11 patients out of 44 were finally qualified for AVR. Only one patient had a THR of less than 85%. Among the remaining 33 asymptomatic patients, 7 did not reach 85% of THR (Figure 2).
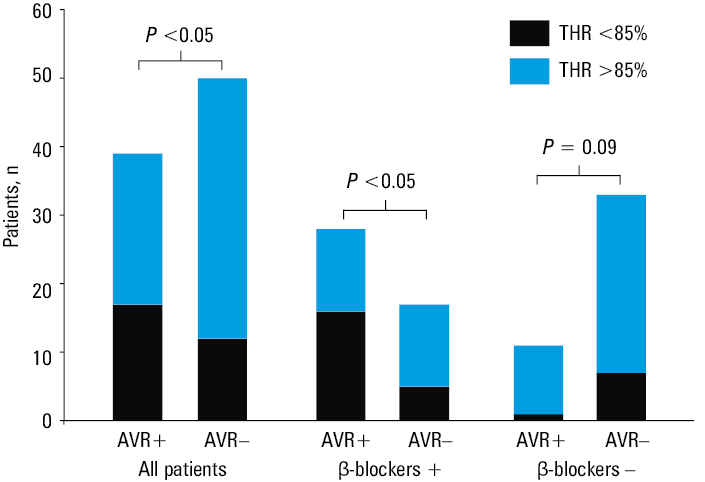
Abbreviations: see Figure 1
Discussion
Despite advances in the diagnosis of valvular heart disease, indications for valve replacement in patients with severe AAS remain controversial. Those supporting surgical treatment emphasize that even if patients with severe AS remain asymptomatic, they have a poor prognosis with a high event rate and early elective surgery should be recommended based on observational studies.8-12,20,21 It was reported that approximately half of the patients diagnosed with severe AS did not report symptoms at the initial evaluation.3,4,22 On the other hand, it is also known that 3% to 11% of patients die soon after the onset of symptoms before AVR can be performed.23 Traditional symptom‑limited ET should be helpful to determine whether patients who do not report symptoms are truly asymptomatic. In a retrospective analysis of prospectively collected data by Saeed et al,24 the mean (SD) event‑free survival at 1 year was 87% (3%) in patients who were asymptomatic on ET compared with 66% (4%) in those with revealed symptoms. Rafique et al25 in their meta‑analysis showed similar data. They found that asymptomatic patients with abnormal results on ET had a 8‑fold higher risk of cardiac events and 5.5‑fold higher risk of sudden death during follow‑up than those with normal results. In 2017, Redfors et al15 summarized 20 publications about stress testing in AAS. They presented a report with available data on stress testing in AS and its potential role in decision making for optimal timing of AVR. Only 7 out of 20 publications pertained to the treadmill stress test, and there were no cycloergometric tests. The rest were stress echocardiogram and cardiopulmonary testing. The most assessed group consisted of severe but also moderate AS. The abnormal stress test was observed in 15% to even 67% of patients. The authors summarized that a positive ET was the strongest predictor of symptoms at follow‑up. There was no explanation why the patients with a positive stress tests were not referred for surgery as recommended by the guidelines.
Our results are in contrast to those presented above. All of our tests were clinically negative. No symptoms were reported in 244 tests. Lack of a clinically positive ET in our group may be associated with a very careful selection of patients. The study group of 89 patients was selected from 120 patients defined as AAS. At baseline, all patients denied symptoms. After a very careful examination, 25 of them confirmed symptoms. Perhaps those patients would be symptomatic during ET if performed.
Lack of symptom reporting might be caused by various reasons. One of them is the self‑limitation of physical activity. Some patients believed that reduced exercise tolerance, shortness of breath, chest pain, and dizziness are related to age, smoking, changes in the spine, etc. Subsequently, they adapted by decreasing their level of activity to avoid symptoms. Patients may also not recognize significant symptoms, often underestimate their severity, and only report when they become extremely limiting.15 Data on the absence of symptoms are based on the information obtained from the patient, but it should also be confirmed by the family.
The ET is contraindicated in symptomatic patients, but it may happen that a patient is not telling the truth. This was the case of one of our patients, who denied the symptoms because he wanted to be under the supervision of the physician who led the program. Despite the symptomatic (stenocardia, dizziness) significant AS, the stress test was performed without any symptoms reported by the patient or complications. At the next visit, the patient refused the test and admitted being symptomatic. Despite clinical and echocardiographic progression, the patient refused surgery and died at home because of heart failure. He was excluded from the study; indeed, he did not fulfill the inclusion criteria to begin with.
Due to doubts related to symptoms in classic ET, new risk factors are searched for. Chambers et al13 described a new exercise measurement with additional important prognostic implication, an early rapid rise in heart rate defined as achieving at least 85% THR or at least 50% increase from baseline within the first 6 minutes. They concluded that rapid rise in heart rate is a compensatory mechanism to maintain cardiac output. This was associated with revealed symptoms later in the same test and predicted AVR. In the previous studies, the authors showed also that stroke volume failed at the start of exercise and before symptoms developed in patients with severe AS.24
Despite no symptoms during the test, we also attempted to determine differences in the results of ET between AVR and non‑AVR groups. Patients in the AVR group had lower exercise capacity in METs and lower heart rate during maximal effort compared with the non‑AVR group. This difference might be easily explained by age because AVR patients were older. On the other hand, the percent of maximal heart rate is age‑adjusted and we found that patients from the AVR group more frequently stopped exercise before they reached 85% of the predicted THR due to fatigue. The maximal heart rate below 85% of the age‑predicted heart rate was also presented as chronotropic incompetence and reported as an important prognostic factor.26 Perhaps in our patients, this could be regarded as an equivalent of AS symptoms. In the univariable Cox regression analysis, THR of less than 85% was related to higher probability of AVR. The significance persisted after adjustment for age. However, after adjustment for the use of β-blockers, this parameter was not significant (P = 0.08). Patients with AAS do not need pharmacological treatment.3,4 When they become symptomatic, they need surgery. The prevalence of hypertension in patients with AS was up to 50% in some studies—in our, younger group, it was about 30%.3,4,27 Hypertension was shown to accelerate the progression of AS and may increase the risk of disease. Hypertension, by increasing the systemic vascular load, had negative effect on hypertrophic remodeling in AS.27,28 However, severe AS has been considered a relative contraindication to antihypertensive treatment due to the risk of hypotension and hemodynamic collapse; nowadays, there is no doubt that hypertension should be treated with caution. Antihypertensive treatment with β-blockers is frequently avoided due to concerns related to the decrease in LV function. This is in line with recent clinical practice guidelines which do not mention β-blockers in the treatment of hypertension.3,4 On the other hand, recent studies have shown that β-blockers are safe and may even be beneficial.27,28
Our patients with hypertension or supraventricular arrhythmias received pharmacological treatment. We found that hypertension had no influence on survival / AVR, but β-blockers did. Moreover, patients treated with β-blockers who did not achieve 85% of the predicted maximal heart rate had a higher probability of AVR. This influence of β-blockers on AVR in this small group of patient warrants further investigation.
Although ET has been performed in AAS for over 15 years, there are still several issues that make the use of ET controversial. In the Euro Heart Survey on Valvular Heart Disease in asymptomatic patients with AS, ET was performed only in 5.7% of patients.18 This observation based on real clinical practice showed the present role of ET in this group of patients. Even in multicenter randomized controlled trials, EVOLVED and AVATAR, that compared early AVR to routine care in AAS, exercise test was not used as a part of the study protocol to eliminate pseudo‑asymptomatic patients.29,30 The definitions of the clinically abnormal exercise test in AAS also differ among reported studies.2,15,16,25,26 Up to 20% of patients with AS are unable to perform a exercise test due to poor mobility or impaired exercise capacity.21 Nowadays, AAS might be a different problem than it was observed 10 to 20 years ago; today, patients with AS are elderly, often with multiple comorbidities, and potentially more vulnerable to hemodynamic derangements associated with severe AS.18,23,25 Furthermore, the level of physical performance was highly varied in the analyzed group. Some patients participated in amateur sports (tennis, cycling, climbing). A large percentage of patients reported that they systematically attended the gym. But there were also patients who had a sedentary lifestyle. Compared to the general population, patients with AS had rather low fitness levels. This is the next indication to perform ET in AAS to establish also the safety of daily physical activities or occupational work.
Current guidelines recommend repeat clinical assessment and echocardiography every 6 to 12 months for severe AS but without information as to whether ET should be repeated at each follow‑up visit.3,4 Similarly to us, some authors highlighted the limited usefulness of the repeated ET (apart from verifying the absence of symptoms).16 At our institution, we perform exercise stress testing in asymptomatic patients with AS to confirm the absence of symptoms.
Although additional assessments such as the echocardiographic assessment of LV function, cardiopulmonary test, risk score (CURRENT‑AS), and biomarkers might improve diagnostics, their role in the management of AAS requires further investigation to justify a class I indication for surgery instead of classic ET.31-39
Limitations
The current cohort of AAS patients was highly selected since the National Institute of Cardiology is dedicated to more difficult cases; therefore, the study group may not represent the general population of patients with AAS. The low number of patients may bias the results.
We performed a cycloergometric exercise test that was not often previously reported in such studies, and our results may not be comparable with studies based on a treadmill stress test. We also did not perform ergospirometry with the measurement of respiratory exchange ratio to assess the exercise level objectively.
It was impossible to assess the exact time point at which the patients developed symptoms between follow‑up ETs. Despite being told to report the symptoms immediately, most of them waited until the scheduled visit. It was also difficult to indicate the most frequent symptom; sometimes it was dizziness, and in other cases, shortness of breath. Most participants complained of angina and more than one symptom. One patient had cardiac arrest with successful resuscitation by the family.
Conclusions
In patients with AAS, ET is safe, but in our study group, the results were not crucial in making the decision to perform AVR. Patients treated with β-blockers who did not achieve 85% of predicted maximal heart rate had a higher probability of AVR. Further research into the influence of β-blocker on the decision to perform AVR in this population is warranted.
- Bonow RO, Greenland P. Population‑wide trends in aortic stenosis incidence and outcomes. Circulation. 2015; 131: 969‑971. | Crossref
- Généreux P, Stone GW, O’Gara PT, et al. Natural history, diagnostic approaches, and therapeutic strategies for patients with asymptomatic severe aortic stenosis. J Am Coll Cardiol. 2016; 67: 2263‑2288. | Crossref
- Baumgartner H, Falk V, Bax JJ, et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017; 38: 2739‑2791. | Crossref
- Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology / American Heart Association Task Force on Practice Guidelines. Circulation. 2014; 129: e521‑e643. | Crossref
- Ross Jr R, Braunwald E. Aortic stenosis. Circulation. 1968; 37: 61‑67. | Crossref
ARTICLE INFORMATION