Why albuminuria should be assessed more frequently in everyday clinical practice? A position statement



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Why albuminuria should be assessed more frequently in everyday clinical practice? A position statement
Introduction
Albuminuria is a well‑established marker of kidney damage and its clinical usefulness has been documented in numerous studies. The use of urinary albumin excretion in the management of hypertension is still insufficient in everyday practice, despite the fact that current European and Polish guidelines indicate the importance of albuminuria in the assessment of cardiovascular risk in this group of patients.1,2 This study presents the rationale for the need for more frequent assessment of albuminuria in everyday clinical practice.
Methods for assessing urinary albumin excretion
Albumin is a protein consisting of 585 amino acids organized in 3 globular domains. Its molecular weight is 66 472 Da. The protein has a free thiol group at cysteine 34, which determines its antioxidant capacity. Albumin molecules express no less than 5 epitopes recognized by different antibodies, which is important for immunoassays. Albumin has a high ability to bind many substances present in the plasma, including drugs, bilirubin, fatty acids, calcium, magnesium, hormones, and metals; it is also subject to glycation. Due to the above characteristics of the albumin molecule, a newly synthesized protein may significantly differ from the protein circulating in the plasma for many days (the half‑life of albumin is up to 20 days): such a molecule is then “loaded” with a number of substances, which may also affect the results of tests for albuminuria. Albumin that enters the urine undergoes additional modifications in the filtrate.3-10
The concept of albuminuria as an indicator of kidney damage and / or a biomarker of systemic diseases dates back to 1969, when elevated albumin levels were first demonstrated in the urine of patients with newly diagnosed diabetes.3 The importance of urine albumin detection in diagnosing and then monitoring kidney damage in diabetes was reinforced by a series of studies performed in the early 1980s; at that time, its role was also found in the prediction of progression of kidney damage and other complications in patients with diabetes.4
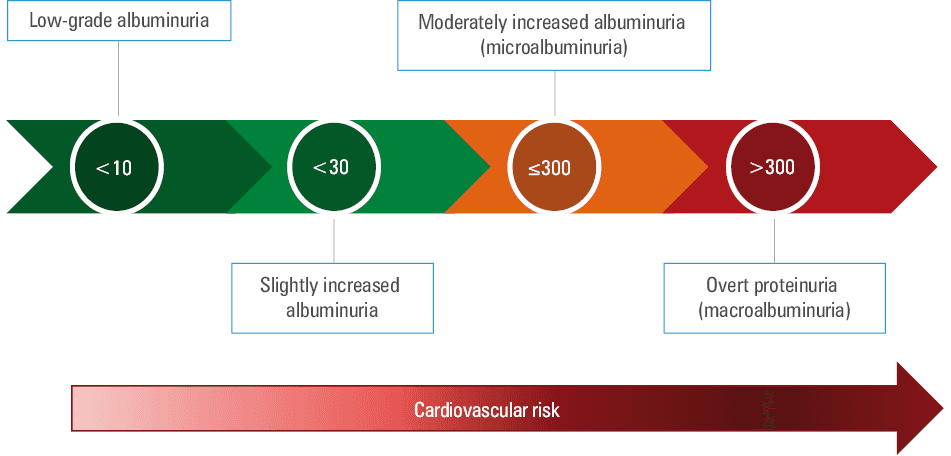
Contemporary reference ranges defining normoalbuminuria have been established based on early studies on albumin excretion and reflect the threshold of sensitivity of the methods used at that time. Most guidelines still consider albumin excretion below 30 mg/d as within the reference range.5-7 Considering technical difficulties with a reliable 24‑hour urine collection, albuminuria is currently defined as the urinary albumin‑to‑creatinine ratio (UACR) in the first morning portion of urine. Normoalbuminuria expressed in this way is below 30 mg/g or 3 mg/mmol creatinine. Some expert groups propose separate normal ranges for men (eg, UACR <17–25 mg/g creatinine) and women (eg, UACR <25–35 mg/g creatinine). Microalbuminuria was defined as urinary albumin excretion in the range of 30 to 300 mg/d (3–30 mg/mmol creatinine, 30–300 mg/g creatinine), and values exceeding the upper limit of this range were defined as macroalbuminuria or overt albuminuria.5-7
Due to the progress in the field of diagnostic methods and the improvement of their sensitivity, the current definitions of normo- and microalbuminuria have been questioned. Population studies using sensitive assays showed that the amount of albumin excreted by healthy individuals is 2.5 to 12 mg/g creatinine (with the distribution of albumin excretion shifted significantly to the left, ie, towards the lowest values). Moreover, a significant increase in cardiovascular risk is observed at as low as 2.5 mg/g creatinine (in fact, the relative risk curve rises most steeply in the range of 2.5 and 30 mg/g creatinine, ie, in the normoalbuminuria range, and then runs flatter).7 Therefore, it can be assumed that the concept of normoalbuminuria, and thus microalbuminuria, does not make sense, or it should be defined with much lower values, probably not exceeding 3–5 mg/g of creatinine. Alternatively, it has been proposed to use the term low‑grade albuminuria, that is, UACR below 10 mg/g creatinine, but without strictly defining the normal value (Figure 1).8 Albumin and creatinine are best determined in the first morning urine sample. Albumin is stable at 4 °C and 20 °C: a sample stored at room temperature should be examined within 8 hours, and if stored in a refrigerator, reliable results can be obtained even after a week. Longer storage requires freezing at –80 °C (when samples are stored at –20 °C, albumin fragmentation occurs). Creatinine in urine is stable for 7 days at room temperature, and also for a very long time after freezing the sample to –20 °C and –80 °C. The reliability of the test is affected by factors such as exercise or acute febrile illness in 24 hours prior to urination, as well as menstruation and urinary tract infection.3-10
The current methods for the determination of urinary albumin excretion are summarized in Table 1. It should be emphasized that over 90% of tests performed are immunoassays, and most of them are based on the turbidimetric method using polyclonal antibodies.9 This method is currently recommended by the National Kidney Disease Education Program / the International Federation of Clinical Chemistry and Laboratory Medicine Working Group on Standardization of Albumin in Urine.10 The sensitivity of urine albumin determination in the concentration range of less than 30 mg/l with the use of strip tests ranges from 79% to 97%.
a There are numerous various modalities for measuring urinary albumin, which reflects the methodological problems encountered by this seemingly simple test. This is primarily due to the lack of a laboratory standard: urine albumin is measured using a lyophilized standard for the determination of plasma proteins (there is no laboratory standard for urine albumin). In addition, albumin undergoes various types of modifications in the urine (including fragmentation into polypeptides that can be immunoreactive or immunononreactive, ie, “visible” or “invisible” for various immunological assays). Another factor determining whether or not albumin in urine will be detected by various techniques is the presence or absence of C‑terminal or N‑terminal fragments of the protein. On the other hand, high performance liquid chromatography can identify proteins other than albumin that have similar physicochemical properties. This means significant discrepancies between the results obtained with the various techniques listed in this Table (eg, for values <30 mg/l, the concentrations are 2- to 3‑fold higher with the high performance liquid chromatography as compared to the immunonephelometry).
b Recommended method
Abbreviations: ELISA, enzyme‑linked immunosorbent assay |
Immunological methods using mono- or polyclonal antibodies
|
Urine protein electrophoresis |
Methods using fluorescent reagents (eg, Albumin Blue 580) |
Methods using color reagents |
High performance liquid chromatography |
Liquid chromatography with mass spectrometry/with tandem mass spectrometry |
Strip tests (eg, Clinitec MA 9 Strip, Siemens; Micral‑Test Strip, Roche and others) |
The recent Kidney Disease: Improving Global Outcomes (KDIGO) guidelines for the diagnosis and treatment of chronic kidney disease emphasize the need to discontinue the use of the term “microalbuminuria” by both clinicians and laboratory diagnosticians. This expert group states that in healthy people, the urinary excretion of albumin does not exceed 10 mg/g of creatinine.7 Interestingly, in the document of the same KDIGO group on the treatment of hypertension in kidney diseases, the term microalbuminuria is used as valid, without a word of comment.3 A critical commentary or reflection on the way of defining normo- or microalbuminuria cannot be found in the latest European guidelines for the treatment of hypertension or in the Polish document devoted to this issue.1,2 However, there are no recommendations in any of the abovementioned documents regarding the method for determining urinary albumin excretion (although all of them indicate UACR as a useful tool for the diagnosis and monitoring of albuminuria).
Albuminuria as a marker of early kidney damage: is it justified to differentiate between normo-, micro-, and macroalbuminuria and why should it be done?
Albuminuria occurs in the early stages of kidney damage, that is, before the estimated glomerular filtration rate (eGFR) is below the reference range.11 Albuminuria is also recognized as a risk indicator for the progression of chronic kidney disease and a useful surrogate in clinical practice to assess the effectiveness of nephroprotective management. The usefulness of albuminuria in this respect has been demonstrated in population12 and observational13 studies, as well as in prospective clinical trials14 and meta‑analyses.15 Measurement of albuminuria in the general population is a valuable test for detecting people at risk of renal impairment, irrespective of the presence of other cardiovascular risk factors (eg, hypertension). Albuminuria has been shown to be of significant diagnostic and prognostic value in diabetic kidney disease (DKD) and in other nondiabetic kidney diseases (eg, IgA nephropathy). When assessing the importance of albuminuria in the diagnostic workup of early kidney damage as well as the risk of progression to advanced renal failure, one should take into account the daily and day‑to‑day variability of urinary albumin excretion, as well as the impact of many factors such as: body position, exercise, high‑protein or high‑sodium diet, or drinking large volumes of fluids.16 In addition, urinary albumin excretion can be influenced by many nonrenal factors, such as fever, inflammation, increase in blood pressure, severe hyperglycemia, or heart failure. Therefore, measuring albuminuria in several urine samples on different days significantly increases the accuracy of the diagnostic and prognostic assessment of this parameter.17
Albuminuria reflects functional and / or structural changes in the glomerular filtration membrane that allow increased transfer (leakage) of albumin into primary urine in amounts exceeding the reabsorption capacity of the proximal nephron tubules. Albuminuria can also be considered as an indicator of early damage (dysfunction) of the vascular endothelium (including the glomerular vessels), which leads to increased permeability of the vascular wall, also for albumin. The most common cause of increased permeability of the glomerular vascular wall is increased intraglomerular pressure (hyperperfusion), which directly leads to increased glomerular filtration (hyperfiltration) and the penetration of albumin into the tubular fluid.18
Hyperperfusion and hyperfiltration within the glomerulus are found, inter alia, in obese people and in patients at early stages of chronic diabetes or in those with non‑DKD. The reabsorption of albumin from the tubular fluid occurs by endocytosis, a process involving transport proteins such as megalin and cubulin. Albuminuria can also result from a defect in the reabsorption or metabolism of albumin in the proximal tubule, or both. Too high concentration of albumin in the tubular fluid and an enhanced reabsorption in the proximal tubule lead to tubulointerstitial injury as a result of the release of proinflammatory cytokines (eg, monocyte chemoattractant protein 3), factors that influence progression of fibrosis (fibrosis‑inducing cytokine, transforming growth factor β), compounds causing vascular damage such as oxygen free radicals or endothelin, and increased apoptosis.18 Increased metabolism of albumin as a result of higher reabsorption of this protein plays a role in the pathomechanism of the progression of chronic kidney injury. The greater the urinary albumin excretion, the greater the risk of end‑stage renal disease or premature death. However, as documented in many studies, this is not a threshold‑dependent relationship and therefore it is impossible to precisely define the magnitude of albuminuria from which its diagnostic and prognostic value is significant. It has been shown that urinary albumin excretion defined as high‑normal also increases the likelihood of future chronic kidney disease.19 Taking into account results of these studies, it was concluded that the term micro- or macroalbuminuria is not appropriate (the risk increases continuously) and therefore many authorities in the field of nephrology propose not to use such a gradation of urinary albumin excretion and use only the term “albuminuria” together with the value of this parameter. This certainly allows a more precise indication of the risk associated with albuminuria, and at the same time, there is no risk of misinterpretation of the terms micro- and macroalbuminuria.8
Albuminuria as a marker of cardiovascular risk
Classic research conducted in the 1980s and 1990s showed an association between increased urinary albumin excretion and the risk of developing nephropathy and cardiovascular events in populations of patients with type 1 and 2 diabetes as well as arterial hypertension.13 The nature of this relationship has also been determined. A study of hypertensive patients with left ventricular hypertrophy (LVH) showed an association between increased urinary albumin excretion and the risk of cardiovascular morbidity and mortality. The observed relationship was linear; no threshold values for the increase in the risk were found, and the relationship did not show any plateau.16
The relationship between albuminuria and cardiovascular risk has also been shown in studies of the general population. In the PREVEND (Prevention of Renal and Vascular End‑stage Disease) population‑based study, increased urinary albumin excretion was associated with a 10‑year cardiovascular mortality of 4.7%, which corresponded to a moderate absolute risk by the Systematic Coronary Risk Evaluation (SCORE) classification.20 The relationship between albuminuria and the risk of death was linear: a 2‑fold increase in albuminuria was associated with an increase in the risk of cardiovascular death by 29% and noncardiovascular death by 12%.20
The results of the above and other studies have been confirmed in large meta‑analyses. A meta‑analysis by the Chronic Kidney Disease Prognosis Consortium of over 630 000 people showed a continuous, linear relationship between albuminuria and cardiovascular risk. This relationship was observed both in the general population and in patients with arterial hypertension, those with diabetes or chronic kidney disease, as well as in those without these diseases.21
As the relationship between albuminuria and cardiovascular risk is continuous and linear, the optimal value of albuminuria with respect to cardiovascular risk cannot be determined. In a study by Chong et al,22 which included healthy young people, it was found that values greater than 6.2 mg/g in women and greater than 4.2 mg/g in men are associated with a higher risk of death. Optimal values were observed in less than 25% of patients with arterial hypertension, diabetes, over 70 years of age, and diagnosed with coronary artery disease, which indicates little usefulness of adopting very low cutoff thresholds for optimal albuminuria in clinical practice.22
It should also be emphasized that the relationship between albuminuria and cardiovascular risk is independent of eGFR. Moreover, eGFR is associated with cardiovascular risk only when it falls below 70 to 75 ml/min/1.73 m2, while in the case of albuminuria this relationship is linear, starting from the lowest values.21 It is worth noting that cystatin clearance is more closely related to cardiovascular risk than creatinine clearance. It has also been shown that, unlike creatinine‑based eGFR, the addition of albuminuria to risk estimation based on cystatin‑based eGFR does not increase the sensitivity of cardiovascular risk assessment.23
Albuminuria and other organ damage
Current guidelines for the management of patients with arterial hypertension include increased urinary albumin excretion—in addition to LVH and a slight degree of renal impairment—in subclinical organ complications of hypertension, which are more severe in coexistence with type 2 diabetes. It should be emphasized that in the light of the 2018 Guidelines of the European Society of Hypertension and the European Society of Cardiology, patients with subclinical organ complications are considered to be at increased total cardiovascular risk.1,2 The update of the guidelines discusses subclinical organ complications in hypertension in relation to the total cardiovascular risk in patients with hypertension and / or type 2 diabetes.
Relationships between albuminuria and cardiac morphology and function have been demonstrated. In a study by Wang et al,24 it was found that the incidence of LVH and left ventricular diastolic dysfunction increase along with the deterioration of renal function, assessed by UACR in a urine sample. It has been shown that in patients with UACR in the third tertile, the incidence of LVH increases by 80% and that left ventricular diastolic dysfunction is 60% more frequent than in patients with UACR in the first tertile. Moreover, it has been confirmed in a multivariate model that albuminuria is an independent predictor of LVH and diastolic dysfunction. Similar observations were provided by the study by Dekkers et al,25 who found a correlation between the indexed mass of the left ventricle and the albumin to creatinine ratio (β = 0.941; 95% CI, 0.2–1.67).
A close relationship between albuminuria and left ventricular muscle hypertrophy was confirmed by the results of the study performed by Rodilla et al,26 who showed a higher percentage of regression of LVH in patients with decreased albuminuria. The percentage of patients with LVH regression was much lower in the group where albuminuria did not decrease.
Albuminuria is also associated with another organ complication: arterial stiffness assessed by the pulse wave velocity measurement. Dekkers et al25 demonstrated a relationship between albuminuria and arterial stiffness. A 2019 study by Vasan et al27 showed correlations between microalbuminuria (log UACR) and central pulse pressure (β = 0.134; P <0.0001) as well as central mean arterial pressure (β = 0.071; P <0.0001) and carotid‑femoral pulse wave velocity (β = 0.144; P <0.0001).
Another evidence supporting the importance of the assessment of organ complications was provided by studies which showed that the occurrence of organ damage—LVH, albuminuria, increased arterial stiffness, and atherosclerotic plaques in the carotid arteries—was associated with a higher risk of cardiovascular events both in patients with a SCORE risk of less than 5% and those with a SCORE risk of 5% or greater.28,29 Thus, the assessment of these complications enables a more precise risk stratification than using the SCORE alone (Table 2).
Score, % | Cardiovascular risk, % | ||
Albuminuriaa (+) | Atherosclerotic plaqueb (+) | Atherosclerotic plaque (+) and albuminuria (+) | |
The incidence of cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, and hospitalization due to coronary artery disease was assessed in 2059 healthy patients aged 41, 51, 61 and 71 years, who were divided into subgroups according to traditionally assessed cardiovascular risk in long‑term follow‑up (median 12.6 years).28
a Albuminuria (+) was defined as UACR ≥90 percentile (men, 0.73 mg/mmol; women, 1.06 mg/mmol)
b Atherosclerotic plaque (+) was defined as the presence of atherosclerotic plaque confirmed on ultrasound of the carotid arteries | |||
1–5 | 12.7 | 14.1 | 25.5 |
5–10 | 13.6 | 16.7 | 38.8 |
Does a reduction in albuminuria translate into a reduction in cardiovascular risk?
As presented above, albuminuria is a significant risk factor for cardiovascular disease and early cardiovascular mortality in patients with / without diabetes or with / without hypertension.20,30,31 Albuminuria reflects a generalized increase in endothelial permeability or dysfunction, which contributes to the progression of chronic kidney disease and cardiovascular disease.32 The key mechanism is the loss of glycocalyx, a polysaccharide gel that covers the endothelial surface facing the lumen of the vessel and normally acts as a barrier to albumin loss.32 The degradation of glycocalyx in response to endothelial stimulation leads to albuminuria, and then to vascular inflammation, which is a pathological basis for the clinical association of albuminuria the progression of renal and cardiovascular diseases.32 In hypertension, renal abnormalities include arteriolopathy of small and medium‑sized vessels, which is characterized by internal intima hyperplasia, hyalinization, and smooth muscle hypertrophy (nephroangiosclerosis). This can be a manifestation of systemic endothelial dysfunction, which can lead to cardiac, cerebral, or renal vascular complications. In addition, these small- and medium‑sized vessels react inadequately to various vasodilators such as nitric oxide and acetylcholine. Similarly, in clinically healthy subjects with albuminuria, vasodilation stimulated by various substances is reduced in proportion to the size of albuminuria. Moreover, elevated levels of von Willebrand factor, a marker of endothelial dysfunction and a risk factor for thrombotic and cardiovascular complications, have been found in nondiabetic hypertensive patients with albuminuria.30-32
The Heart and Soul Study evaluated soluble endothelial cell‑selective adhesion molecule, a marker of endothelial dysfunction and a risk factor for worsening of renal function and albuminuria, and showed that elevated levels of soluble endothelial cell‑selective adhesion molecule were significantly and independently associated with a decrease in baseline eGFR below 60 ml/min/1.73 m2 and increased albuminuria (UACR ≥30 mg/g; P <0.0001).33 Soluble endothelial cell‑selective adhesion molecule was found to be associated with albuminuria and deterioration of renal function in both cross‑sectional and prospective studies, which confirms that endothelial dysfunction may potentially contribute to an increased risk of kidney disease and cardiovascular disease.33
It can be postulated that a reduction in albuminuria, a marker of endothelial and vascular dysfunction, will also be an indicator of a reduction in cardiovascular risk.
In the LIFE (Losartan Intervention For Endpoint Reduction in Hypertension) study, albuminuria was associated with the risk of the primary endpoint (cardiac death, myocardial infarction, or stroke regardless of the presence of concomitant diabetes).34 The authors of this study showed that changes in albuminuria correlate with changes in cardiovascular risk—a decrease in albuminuria was associated with a reduction in the risk of the primary endpoint.35
Viazzi et al36 conducted an interesting analysis which included 16 clinical trials involving a total of 48 580 patients. The studies were divided according to the presence of differences regarding albuminuria during follow‑up. It has been shown that in studies in which a difference in albuminuria was observed between the compared groups, there was also a difference in the frequency of cardiovascular events (risk reduction by 55% in favor of groups with lower albuminuria). In studies where no differences in albuminuria were found between the compared groups, no differences in the frequency of cardiovascular events were found either.
A separate analysis of the results of 6 clinical trials (36 325 patients) was performed, in which the frequency of cardiovascular events was assessed depending on the changes in albuminuria. It was shown that the risk of cardiovascular events was reduced by 51% in patients whose albuminuria decreased or remained stable compared with patients with increased albuminuria.36 The results of this meta‑analysis are consistent with the results of the previous meta‑analysis—both showed that a 10% and 30% reduction in albuminuria was associated with a reduction in the risk of cardiovascular events by 14% and 16%, respectively.36,37
Assessment of albuminuria in patients with diabetes
Diabetic kidney disease has become the leading cause of end‑stage renal disease over the past few decades.38,39 This microvascular complication of diabetes affects about 30% of people with type 1 diabetes and about 40% of people with type 2 diabetes.38 The observed prevalence of DKD reflects a significant increase in the incidence of diabetes, which has been considered as the noncommunicable epidemic of the 21st century. From a prognostic point of view, it is important that the incidence of DKD, regardless of the type of diabetes, is also associated with an increased cardiovascular risk, cardiovascular mortality and all‑cause mortality. Therefore, preventing the development and / or progression of DKD is crucial for reducing the risk of end‑stage renal disease requiring renal replacement therapy, but also, and perhaps above all, for reducing the risk of cardiovascular mortality, and thus significantly improving the quality of life in this special patient population.38,39
Traditionally, the natural history of DKD includes the hyperfiltration stage, transition from normoalbuminuria to microalbuminuria, overt proteinuria with gradual decline in glomerular filtration to the stage of terminal renal failure.40 Today, however, this complication is becoming more and more heterogeneous. Currently, it is believed that the typical DKD phenotype is changing, as there are more and more people with diabetes who have low eGFR but without concomitant albuminuria.41 In the available studies, the percentage of patients with type 2 diabetes and normoalbuminuria despite lowered eGFR values (eGFR <60 ml/min/1.73 m2) ranged from 16% to 33%.42,43 The above observations were also confirmed for patients with type 1 diabetes,44 and in some of the studies the percentage of patients with normoalbuminuria and reduced eGFR reached even 50% to 60%.45,46 The cause of the above phenomenon is believed to be better glycemic and blood pressure control and the widespread use of drugs blocking the renin‑angiotensin system (RAS).
In patients with diabetes, the urinary albumin excretion, serum creatinine, and eGFR should be determined to detect or assess the severity of DKD. Albuminuria and eGFR are independent predictors of cardiovascular and renal risk in diabetic patients.47,48 Diabetic kidney disease is asymptomatic for a long time, so performing screening tests is an extremely important aspect of managing diabetes.47,48 Screening tests should be repeated annually; in patients suffering from type 2 diabetes, it should be started immediately after the diagnosis of diabetes, and in patients with type 1 diabetes after 5 years from the diagnosis of diabetes.47,48
In order to assess the urinary albumin excretion, the UACR should be determined based on the results of quantitative tests in a single, preferably morning, urine sample. Two positive UACR results are the basis for the diagnosis of increased urinary albumin excretion (Table 3). The urinary albumin‑to‑creatinine ratio, defined as the amount of albumin excreted in the urine per 1 g of creatinine, approximately corresponds to daily albuminuria, and the use of this method allows errors related to the 24‑hour urine collection to be avoided.47,48 Twenty‑four‑hour urine collection is more inconvenient and is only slightly superior to point measurements in terms of predictive value or accuracy. Measuring only albumin in a urine spot sample (regardless of the method used: immunoassay or a sensitive albuminuria‑specific strip test) without simultaneously measuring urine creatinine is cheaper but is more likely to be false negative or false positive as a consequence of the variability of albumin concentration in urine, depending on the level of hydration.47,48 There is a large variability (>20%) in urinary albumin excretion measurements; therefore, to conclude that a patient has high or very high albuminuria, 2 out of 3 UACR samples collected over a period of 3 to 6 months should be abnormal. At the same time, it should be remembered that physical activity in the 24 hours preceding urine sample collection, coexisting infections, elevated body temperature, congestive heart failure, significant hyperglycemia, significant hypertension, or menstruation may increase the UACR value regardless of the degree of kidney damage.49
Category | Albumin excretion rate, mg/d | Albumin‑to‑creatinine ratio (random urine sample), mg/d or mg/g creatinine | Albumin excretion – urine collection, μg/min |
A1: normal or slightly increased albuminuria | <30 | <30 | <20 |
A2: moderately increased albuminuria | 30–300 | 30–300 | 20–200 |
A3: overt proteinuria | >300 | >300 | ≥200 |
eGFR should be calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD‑EPI) formula.47-49 Patients with urinary albumin greater than 30 mg/g creatinine and / or eGFR <60 ml/min/1.73 m2 should be monitored twice a year in order to optimize therapy.47-49
Effect of the renin‑angiotensin system inhibitors on albuminuria
When discussing clinical trials assessing the effect of antihypertensive treatment on albuminuria, studies such as BENEDICT, ROADMAP, ADVANCE, and ONTARGET deserve special attention.18,50,51
The BENEDICT (Bergamo Nephrologic Diabetes Complication Trial) study, the results of which were announced in 2006, included 1204 patients with hypertension and type 2 diabetes, and with normal urinary albumin excretion.18 In a 4‑year follow‑up, the effects of an angiotensin‑converting enzyme inhibitor, trandolapril, and a calcium antagonist, verapamil, as well as the combination of both these drugs on the increase in albuminuria were assessed. Compared with placebo, the beneficial effect of preventing the increase in albuminuria (new cases of moderately increased albuminuria) was obtained only in patients whose therapy was based on an angiotensin converting enzyme inhibitor.18
In 2011, the results of the ROADMAP (Randomized Olmesartan and Diabetes Microalbuminuria Prevention) trial were published in the New England Journal of Medicine.50 This was a randomized, double‑blind clinical trial conducted in 19 countries in Europe, including centers from Poland. Study participants—4447 patients with type 2 diabetes with normoalbuminuria, regardless of baseline blood pressure—were randomized to receive the angiotensin II receptor antagonist, olmesartan, or placebo. The primary endpoint was time to the first onset of microalbuminuria. The median follow‑up was 3.2 years.50
In the olmesartan group, microalbuminuria developed in 8.2% of patients (median time, 722 days), while in the placebo group, microalbuminuria occurred in 9.8% of patients (median time 576 days). The unadjusted hazard ratio for onset of microalbuminuria was 0.77 (P = 0.01). After adjustment for blood pressure difference, the hazard ratios were 0.83 (P = 0.08) and 0.82 (P = 0.06) adjusted for systolic and diastolic blood pressure, respectively. After adjustment for baseline differences in the body mass index, systolic blood pressure, and high‑density lipoprotein cholesterol and triglycerides levels, the hazard ratio for the primary endpoint was 0.75 (P = 0.006). There was also a significant reduction in the risk of microalbuminuria during treatment with olmesartan at a dose of 40 mg in the subgroups of patients with the following characteristics at baseline: systolic blood pressure >135 mm Hg, HbA1c ≤7.3%, eGFR ≤83.79 ml/min/1.73 m2, and albuminuria >4 mg/g creatinine.50
The aim of the blood pressure‑lowering arm of the prospective ADVANCE (Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation) trial was to demonstrate whether a single‑pill combination of an angiotensin converting enzyme inhibitor and a thiazide‑like diuretic added to the standard treatment in patients with type 2 diabetes, regardless of blood pressure and treatment used, is associated with reduction in micro- and macroangiopathy.51 The study included 11 140 patients with type 2 diabetes and high cardiovascular risk (mean age, 66 years; 43% were females). There were 604 participants enrolled in the study in Polish centers. Over an average of 4.3 years of follow‑up, the active treatment group also showed a reduction in all cardiac events (14%), all kidney events (21%), development or progression of nephropathy (18%), and development of microalbuminuria (21%) compared with the placebo group. In the experimental group, the levels of proteinuria observed during treatment showed a strong, independent relationship both with renal and cardiovascular events.51
The ONTARGET (Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial) study, which included a very large group of patients with high or very high cardiovascular risk, showed that changes in urinary albumin excretion had a prognostic value for the occurrence of cardiovascular events and death, regardless of the baseline albumin excretion.30
When presenting studies assessing the effect of antihypertensive treatment on albuminuria, renal function, or the incidence of cardiovascular events, one should also mention other interesting research programs, which have shown a beneficial effect of RAS inhibitors on the reduction of albuminuria and chronic kidney disease progression, but discussing these studies in detail is beyond the scope of this paper.
Effect of calcium channel blockers on albuminuria
Calcium channel blockers lower blood pressure to a similar extent as other classes of antihypertensive drugs. However, the benefits of this class of drugs remain inconclusive in terms of their nephroprotective effects beyond those associated with lowering blood pressure. In an animal model, a beneficial effect of calcium antagonists in slowing down the progression of renal failure associated with aging has been shown.52 Several prospective, randomized clinical trials in patients with CKD with proteinuria have shown an increase in urinary protein excretion and an acceleration of renal disease progression after the use of dihydropyridine (DHP) calcium channel blockers.
However, there have been a few reports from small clinical trials showing a reduction in proteinuria and in the rate of nephropathy progression after administration of non‑dihydropyridine (NDHP) calcium channel blockers, but not in patients with advanced stages of chronic kidney disease. In the BENEDICT study, the nephroprotective effects of trandolapril, verapamil or a combination of both were assessed in patients with diabetic nephropathy and proteinuria.53 Target blood pressure values were achieved in all groups. It has been shown that administration of verapamil combined with trandolapril resulted in a greater decrease in proteinuria than monotherapy with trandolapril or verapamil.
A review of 28 clinical studies on the effect of calcium antagonists on renal function showed that DHP and NDHP calcium channel blockers have a similar hypotensive effect but differ in their impact on urinary protein excretion.52 Dihydropyridine derivatives increased proteinuria by 2%, while NDHP calcium antagonists decreased it by as much as 30% (P = 0.01).
The effect of classic DHP calcium channel blockers, such as nifedipine or amlodipine, on the glomerular vessels is based on the preferential dilatation of the arterioles that supply blood to the glomerulus, thereby increasing glomerular filtration and renal blood flow. Hence, in clinical trials, the beneficial effect of DHP calcium channel blockers on the improvement of renal function was found, especially in the case of contrast nephropathy, acute post‑transplant renal failure due to the nephrotoxic effect of cyclosporine.
However, such influence on the glomerular vessels increases the intraglomerular pressure, which may make classic DHP calcium channel blockers less effective in reducing microalbuminuria or proteinuria. A slightly different effect has been demonstrated for another DHP calcium channel blocker, lercanidipine, which has shown a greater affinity for calcium T‑channels compared with amlodipine and lacidipine in in vitro studies, and these properties may explain its clinical benefits.54 In studies on rats with arterial hypertension, lercanidipine showed a nephroprotective effect, which was most likely a consequence of vasorelaxation of both the afferent and efferent arterioles.55
A study by Zucchelli et al56 showed that although in patients with nondiabetic CKD, both nifedipine and captopril were associated with achieving similar blood pressure levels and a similar reduction in GFR decline, the angiotensin converting enzyme inhibitor was more effective in reducing proteinuria.
In the AASK (African‑American Study of Kidney Disease) and the IDNT (Irbesartan Diabetic Nephropathy Trial), a DHP calcium channel blocker, amlodipine, was shown to be less effective in slowing renal function loss and reducing proteinuria than RAS blockers or even a β-blocker.57,58
The ZAFRA (Zandip en Función Renal Alterada) study in patients with chronic kidney disease showed a beneficial nephroprotective effect of lercanidipine.59 When this drug was added to a RAS blocker, a significant reduction in blood pressure was observed. The levels of creatinine and urea did not change, but there was a significant increase in creatinine clearance, and at the end of the study, after 6 months of treatment, proteinuria decreased significantly. However, it should be noted the lercanidipine is contradicted in patients with eGFR of less than 30 ml/min/1.73 m2.
In the DIAL (Diabete, Ipertensione, Albuminuria, Lercanidipina) study, no difference was found in the effect of lercanidipine and ramipril on the reduction in albumin excretion rate.60 The proportion of patients progressing from microalbuminuria to proteinuria or vice versa was similar, while a 50% reduction in albumin excretion rate was achieved by 34.2% of patients in the lercanidipine group and 22.2% in the ramipril group.
On the other hand, in the RED LEVEL trial,61 the combination of enalapril and lercanidipine had a stronger nephroprotective effect than enalapril and amlodipine alone after 12 months of treatment.
Based on these results, the 2019 guidelines of the Polish Society of Hypertension indicated lercanidipine as the preferred DHP calcium channel blocker in patients requiring special nephroprotection.2
Effect of other antihypertensive drugs on albuminuria
Diuretics
The NESTOR (Natrilix SR versus Enalapril Study in hypertensive Type 2 diabetics with Microalbuminuria) study compared the effects of long‑acting indapamide (SR) vs enalapril on albuminuria in patients with hypertension and type 2 diabetes older than 65 years.62 Both drugs produced a similar reduction in blood pressure. Similarly, UACR reduction was comparable in both groups (46% for indapamide SR and 47% for enalapril).
β-Blockers
Studies on the effects of this class of drugs on albuminuria are based on older (noncardioselective) β-blockers. In the LIFE study,63 which demonstrated the superiority of losartan over atenolol in reducing cardiovascular events (especially stroke), the former drug was also more effective in reducing UACR (33% for losartan vs 15% for atenolol; P <0.001). Data on the effect of modern cardioselective β-blockers are not available.
Aldosterone antagonists
Aldosterone antagonists, although used only in the fourth line of antihypertensive therapy, has a well‑documented beneficial effect on microalbuminuria.64,65 A meta‑analysis of 31 studies involving 2767 patients showed that the use of aldosterone antagonists decreased UACR by 25% and 24‑hour urinary albumin excretion by 32%.66 A beneficial effect of the therapy was observed for spironolactone, eplerenone and finerenone. These studies confirm that aldosterone plays an important role in the development of albuminuria. Reduction in albuminuria after the use of aldosterone antagonists has also been observed in patients previously treated with angiotensin‑converting enzyme inhibitors or angiotensin II receptor blockers This group of patients should be carefully monitored for the risk of hyperkalemia. This risk will probably be minimized in the future when patiromer is introduced for use in clinical practice.67
Imidazole receptor agonists
Activation of the sympathetic nervous system may, both directly and indirectly (through a stimulating effect on the RAS), lead to impaired renal function and the development of microalbuminuria. This hypothesis was confirmed by a study evaluating the effect of low‑dose moxonidine on albuminuria in patients with type 1 diabetes.68 It turned out that despite no reduction in blood pressure, inhibition of the sympathetic system activity through the use of an imidazole receptor agonist led to a decrease in urine albumin excretion.
Endothelin antagonists
For many years, attempts have been made to find the place for endothelin antagonists in the treatment of arterial hypertension. Due to side effects (especially fluid retention), nonselective protoplasts of this class of drugs were not introduced to the market. Hope is associated with selective endothelin A receptor antagonists. Atrasentan has been shown to reduce albuminuria while not increasing fluid retention significantly.69,70 The SONAR (Study of Diabetic Nephropathy with Atrasentan) showed a reduction in the risk of renal events; however, no reduction in the risk of hospitalization or death was observed.71
Sodium‑glucose cotransporter‑2 inhibitors
The sodium‑glucose cotransporter‑2 inhibitors are a new group of antidiabetic drugs, which is characterized by additional properties: lowering of blood pressure, reducing the incidence of cardiovascular events and death in patients with heart failure, and also having nephroprotective properties. It has been shown that sodium‑glucose cotransporter‑2 inhibitors reduce albuminuria across the range of eGFR and in patients with normoalbuminuria, moderately increased albuminuria, and severely increased albuminuria. A meta‑analysis based on 15 studies with 17 540 patients showed a mean reduction in albuminuria of 25%. Additionally, this effect might be greatest in patients with moderately and severely increased albuminuria.72-74
Summary
The available data from clinical trials clearly show a significant, linear relationship between albuminuria and the risk of cardiovascular complications. Analyzes of clinical trials suggest that a decrease in albuminuria may be an indicator of a reduction in cardiovascular risk. Renin‑angiotensin system inhibitors as well as other antihypertensive drugs, sodium‑glucose cotransporter‑2 inhibitors and statins reduce albuminuria.65 In conclusion, as summarized in Table 4, it should be remembered that albuminuria is a simple and cheap marker of cardiovascular risk as well as an indicator of optimal therapy in patients with arterial hypertension. Therefore, the group of experts who prepared this position statement paper strongly recommends that albuminuria should be estimated more often in everyday clinical practice.
Albuminuria is an indicator of early damage (dysfunction) of the endothelium and blood vessels (including the glomerular vessels). It is directly related to the risk of cardiovascular events. |
Albuminuria is an established risk factor for the progression of chronic kidney disease and a useful surrogate in nephroprotective treatment. |
The most useful method of assessing albuminuria is the assessment of albumin and creatinine concentrations ratio in the first morning or random urine sample. |
The reliability of albuminuria determination is influenced by, among others: physical exercise, diet (high in protein or high in sodium), fluid supply, fever, menstruation, urinary tract infection, hyperglycemia, increase in blood pressure, heart failure. |
Low‑grade albuminuria is defined as a ratio of albumin to creatinine concentration in urine sample <10 mg/g. |
Moderately increased albuminuria (microalbuminuria) is defined as a ratio of albumin and creatinine concentration in urine sample 30–300 mg/g. |
Renin‑angiotensin system inhibitors—angiotensin converting enzyme inhibitors and angiotensin II receptor blockers—prevent the development of microalbuminuria (moderately elevated albuminuria) and reduce albuminuria in patients with moderately elevated albuminuria. |
Among other antihypertensive drugs, albuminuria reduction was shown for calcium channel blockers (lercanidipine), diuretics (indapamide), aldosterone antagonists, and centrally acting drugs (rilmenidine). |
Reduction of albuminuria may serve as a surrogate marker of antihypertensive drug effectiveness in reduction of cardiovascular risk apart from blood pressure reduction. |
- Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens. 2018; 36: 1953‑2041.
- Tykarski A, Filipiak KJ, Januszewicz A, et al. 2019 Guidelines for the management of hypertension – Part 1‑7. Arterial Hypertension. 2019; 23: 41‑87. | Crossref
- Keen H, Chlouverakis C, Fuller J, Jarrett RJ. The consomitants of raised blood sugar: studies in newly‑detected hyperglycaemics. II. Urinary albumin excretion, blood pressure and their relation to blood sugar levels. Guys Hosp Rep. 1969; 118: 247‑254.
- Mogensen CE. Microalbuminuria predicts clinical proteinuria and early mortality in maturity‑onset diabetes. N Engl J Med. 1984; 310: 356‑360. | Crossref
- Stevens LA, Levey AS. Current status and future perspectives for CKD testing. Am J Kidney Dis. 2009; 53: S17‑S26. | Crossref
ARTICLE INFORMATION