A 66‑year‑old male patient was admitted to the emergency unit with a suspicion of acute upper gastrointestinal bleeding. His medical history was unremarkable. The symptoms appeared for the first time 3 days earlier and they encompassed vomiting and abdominal pain. On the day before admission, the patient started to vomit with fresh blood. On admission, he was hemodynamically stable and his body temperature was normal. Physical examination of the abdomen revealed tenderness in the epigastric region, without any palpable mass. There were no signs suggestive of peritonitis, and the peristalsis was intact. Digital rectal examination revealed melena.
Blood tests showed leukocytosis with a hemoglobin level of 18 g/dl. There were laboratory signs of acute kidney injury of prerenal origin. The patient underwent urgent upper gastrointestinal endoscopy which revealed multiple areas of black mucosa with diffuse white exudates in the middle and distal parts of the esophagus (Figure 1A and 1B). There were also signs of hiatal hernia. Moreover, there was deep ulceration in the duodenal bulb (Forrest IIc) with duodenal deformation and stricture. Insertion of the gastroscope into the distal part of the duodenum was impossible.
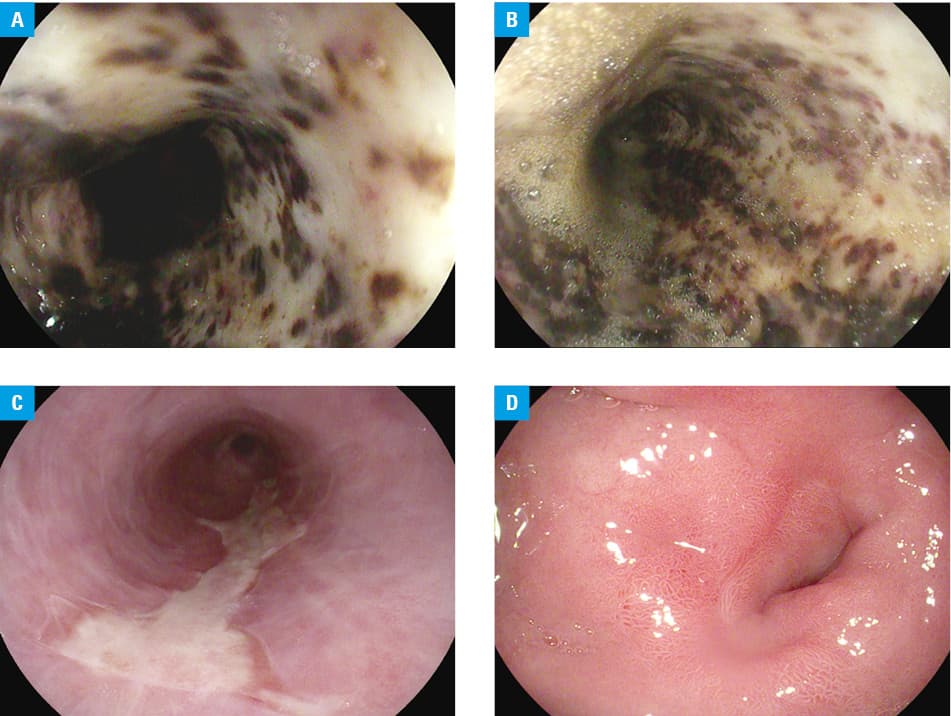
Gastroscopy revealed typical macroscopic signs of acute esophageal necrosis (AEN), also known as “black esophagus.”1 It is a rare entity typically associated with multiorgan dysfunction, hypotension, sepsis, acute alcohol intoxication, or other severe underlying conditions.1-3 Clinical presentation of AEN includes mainly hematemesis and abdominal pain. The etiology is unknown; however, it seems that local hypoperfusion and chemical injury caused by gastric content are the most important driving factors.1 Typical endoscopic appearance of black mucosal discolorations frequently accompanied by massive, white exudates localized in the middle and distal parts of the esophagus allows for making the final diagnosis; further histological confirmation is not necessary.1 Treatment should be focused on the underlying conditions as well as therapy with proton pump inhibitors, nil‑per‑os restriction are also needed.1,2
All symptoms of our patient resolved after the initiation of conservative treatment. Follow‑up gastroscopy performed after 4 weeks revealed almost complete healing of the esophageal lesions with focal exudative mucosal remnants (Figure 1C). The ulceration of the duodenal bulb was healed with a stricture (Figure 1D) which could be easily passed by the endoscope.
Our case report shows that AEN can also appear in patients without severe comorbidities. Gastric outlet obstruction resulting from a complicated duodenal ulcer disease, hiatal hernia, and acute dehydration probably were the main driving factors of AEN.1
- Gurvits GE. Black esophagus: acute esophageal necrosis syndrome. World J Gastroenterol. 2010; 16: 3219‑3225. | Crossref
- Cho JH, Kim TN. Acute esophageal necrosis (black esophagus) associated with duodenal ulcer bleeding: a case report. Int J Clin Exp Med. 2019; 12: 6249‑6253.
- Siddiqi A, Chaudhary FS, Naqvi HA, et al. Black esophagus: a syndrome of acute esophageal necrosis associated with active alcohol drinking. BMJ Open Gastro. 2020; 7: e000466. | Crossref
ARTICLE INFORMATION