IgG4-related retroperitoneal fibrosis: a condition commonly overlooked in daily clinical practice



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
IgG4-related retroperitoneal fibrosis: a condition commonly overlooked in daily clinical practice
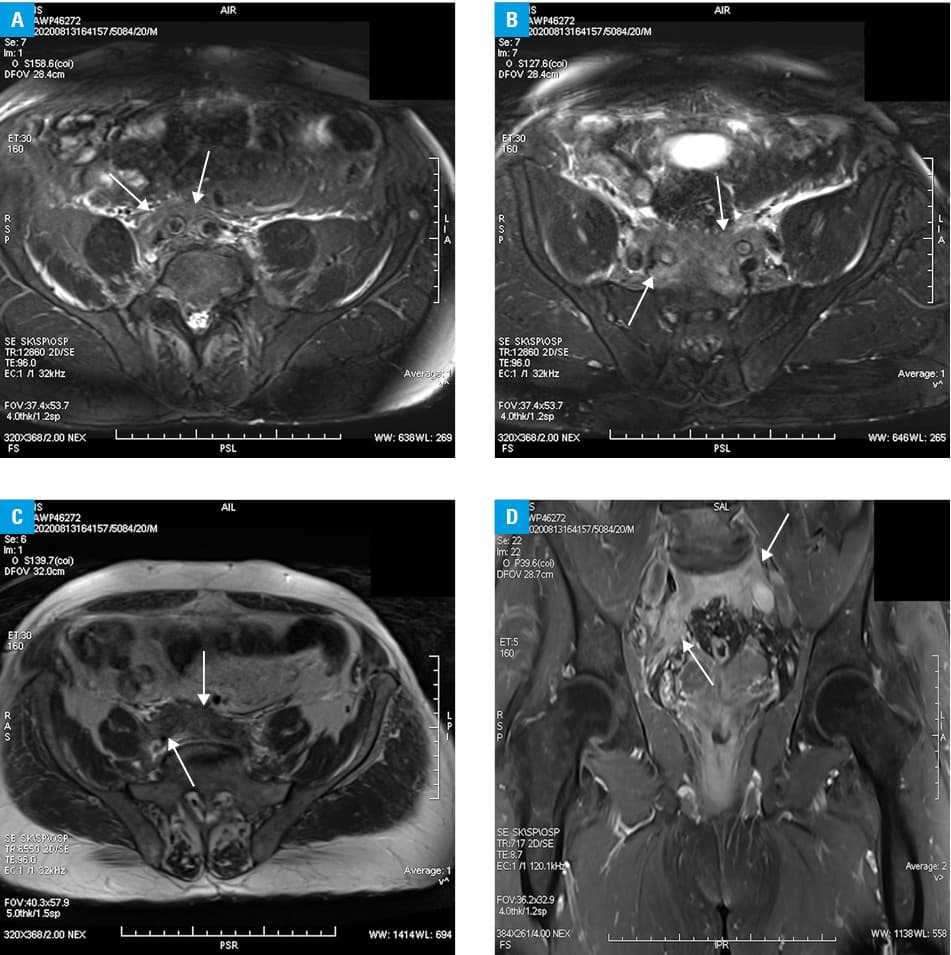
A 69‑year‑old man with prostatic hypertrophy and arterial hypertension was referred to the hospital due to swelling, pain, and redness of the lower limbs that had been increasing for a month. Apart from the reported ailments, the physical examination showed varicose veins and trophic changes in the lower limbs. Doppler ultrasound examination of the lower extremities excluded thrombosis. Abdominal computed tomography scan showed a nonspecific infiltration in the retroperitoneal and presacral spaces distal to the aortic bifurcation, narrowing the lumen of the iliac veins. The patient was referred to the Department of Internal, Autoimmune and Metabolic Diseases due to suspected retroperitoneal fibrosis. On admission, laboratory findings revealed elevated fasting glucose (6.22 mmol/l; reference range, 3.9–5.5 mmol/l), impaired glucose tolerance after 2‑hour oral glucose tolerance test (8.77 mmol/l; reference range <7.8 mmol/l), and mild normocytic anemia (hemoglobin, 131 g/l; reference range, 135–165 g/l). Moreover, serum albumin was 49% of total blood protein (reference range, 54%–65%), serum γ-globulin was 25% (reference range, 9%–18%), and albumin to globulin ratio was 0.96 (reference range, 1.27–1.96). Anti‑dsDNA antibodies as well as complement C3 and C4 components were negative. Of note, there was an extremely high IgG4 concentration of 5.003 g/l (reference range, 0.039–0.864 g/l). Other biochemical parameters remained within reference ranges. Echocardiography did not show any valve dysfunction or abnormal contractility, and left ventricular ejection fraction was 55%. Chest X‑ray showed no significant findings. Magnetic resonance imaging of the abdomen and the pelvis showed retroperitoneal paraspinal infiltration at the level of lumbar 4 and lumbar 5 spinal segments, and in the presacral space, surrounding the iliac vessels and the infrarenal aorta (Figure 1A–1D).
The high concentration of IgG4 together with the results of radiological examinations and the clinical condition led to the diagnosis of IgG4‑related retroperitoneal fibrosis. The patient was treated with systemic prednisone at a dose of 30 mg/day, which resulted in improvement of the patient’s clinical status.
IgG4‑related retroperitoneal fibrosis is a rare disease characterized by the accumulation and spreading of fibrous tissue around the abdominal aorta, iliac vessels, and adjacent structures in the retroperitoneum with lymphoplasmacytic infiltration of IgG4(+) plasma cells in the affected tissue.1,2 Our patient presented with a typical course of IgG4‑related disease with the involvement of the retroperitoneum, in terms of clinical, serological, and radiological findings, in accordance with the latest American College of Rheumatology / European League Against Rheumatism classification criteria for IgG4‑related disease.3 These novel, validated criteria are of high specificity (97.8%) and sensitivity (82%), facilitating the classification of the disease, taking into account the exclusion criteria. However, failure to meet the threshold of 20 points or more does not exclude the diagnosis, especially if the patient’s clinical diagnosis is IgG4‑related disease, but a representative biopsy cannot be performed.3 Our patient’s ailments were caused mainly by the vascular obstruction, but symptoms may also include vein thrombosis, hypertension, and postrenal injury due to compression of the ureter.4,5 Because of its rare occurrence and varied clinical course, IgG4‑related retroperitoneal fibrosis seems to be overlooked in everyday clinical practice.
- Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4‑related disease. Mod Pathol. 2012; 25: 1181‑1192.
- Perugino CA, Stone JH. IgG4‑related disease: an update on pathophysiology and implications for clinical care. Nat Rev Rheumatol. 2020; 16: 702‑714. | Crossref
- Wallace ZS, Naden RP, Chari S, et al. The 2019 American College of Rheumatology / European League Against Rheumatism classification criteria for IgG4‑related disease. Ann Rheum Dis. 2020; 79: 77‑87. | Crossref
- Ochoa Chaar CI, Aurshina A. Endovascular treatment of duplicated inferior vena cava compression from retroperitoneal fibrosis. J Vasc Surg Cases Innov Tech. 2018; 4: 311‑314. | Crossref
- Corradi D, Maestri R, Palmisano A, et al. Idiopathic retroperitoneal fibrosis: clinicopathologic features and differential diagnosis. Kidney Int. 2007; 72: 742‑753. | Crossref
ARTICLE INFORMATION