An 81‑year‑old man with COVID‑19, hypertension, and paroxysmal atrial fibrillation treated with a direct oral anticoagulant, dabigatran, was admitted to a temporary hospital for patients with COVID‑19. On admission, he presented with fever (39 ºC) and dyspnea. Physical examination revealed lung crepitations on auscultation, tachypnea (35 breaths/min), and oxygen saturation of 89% on air. Laboratory tests showed elevated levels of C‑reactive protein (113 mg/l; reference range, 0–5 mg/l), procalcitonin (1.16 ng/ml; reference range, 0–0.2 ng/ml), and increased white blood cell count (11.48 × 103/µl; reference range, 4–10 × 103/µl), while the D‑dimer level was within the reference range (0.45 mg/l; reference range, 0–0.5 mg/l). Chest radiography revealed slight interstitial inflammatory lesions in the left lung (Figure 1A). Treatment with oxygen, empirical antibiotics, and steroids was initiated. Dabigatran was continued at a full dose according to age.
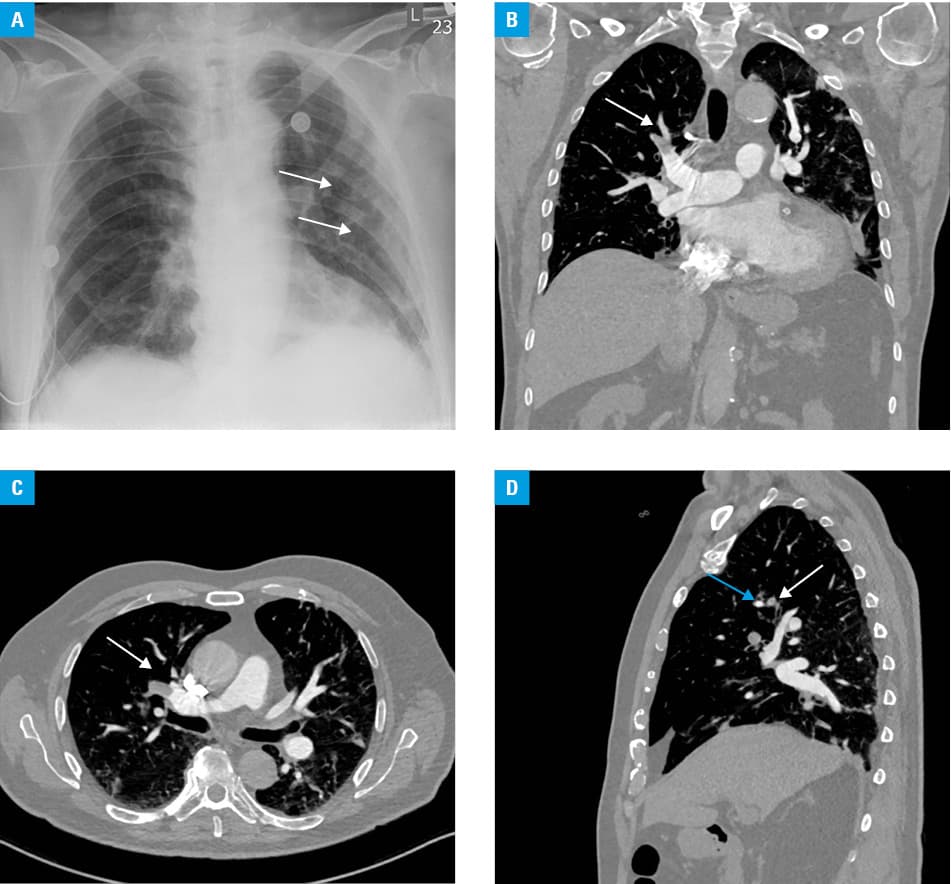
The treatment resulted in clinical improvement, and the patient began to breathe spontaneously. The levels of inflammatory markers were normal. However, on day 11, the patient developed dyspnea, pleuritic chest pain, and cough. Based on clinical data, low‑risk pulmonary embolism was diagnosed. Laboratory tests showed elevated D‑dimer levels (1.86 mg/l). Troponin and N‑terminal pro‑B‑type natriuretic peptide levels were unremarkable. Physical examination did not reveal edema of the lower extremities. Doppler ultrasound for deep vein thrombosis was unavailable. Computed tomography pulmonary angiography revealed emboli in the segmental and subsegmental arteries entering the right upper lobe (Figure 1B–1D). Low‑molecular‑weight heparin, nadroparin, was administered at a therapeutic dose (2 × 0.8 ml [2 mg/kg]). Dabigatran was discontinued. Respiratory symptoms resolved and normal D‑dimer levels were restored. At 4 weeks, the cardiovascular and respiratory status improved and the patient was discharged home.
Literature shows that severe COVID‑19 can be complicated with coagulopathy. Although the exact incidence of venous thromboembolism (VTE) is unknown, some reports suggest that it may be higher than in hospitalized patients with similar severity of VTE and without COVID‑19. Therefore, in the absence of contraindications, acutely ill hospitalized patients with COVID‑19 should receive anticoagulant thromboprophylaxis.1 However, some patients were reported to develop VTE even on anticoagulation.2,3 In our case, the patient had nonvalvular atrial fibrillation and received full‑dose anticoagulation. In line with the guidelines, he fulfilled dose‑reduction criteria based on age over 80 years, and dabigatran dose was reduced from 300 to 220 mg/d.4 Despite adequate anticoagulation, pulmonary embolism was diagnosed on day 11 of infection. Evidence on the best anticoagulant agent for VTE prevention is lacking. Based on randomized trials of thromboprophylaxis in acutely ill hospitalized patients without COVID‑19, experts of the American College of Chest Physicians recommend low‑molecular‑weight heparin or fondaparinux over direct oral anticoagulants in patients with COVID‑19.1 A similar case was described in May 2020 and concerned a patient whose D‑dimer level was 65‑fold higher.5 The D‑dimer level in our patient was 4.1‑fold higher. These data suggest that in the course of SARS‑CoV‑2 pneumonia, we cannot indicate a cutoff point for D‑dimer levels, which would enable us to exclude pulmonary embolism in patients using full‑dose anticoagulation due to atrial fibrillation.
- Moores LK, Tritschler T, Brosnahan S, et al. Prevention, diagnosis, and treatment of VTE in patients with coronavirus disease 2019: CHEST Guideline and Expert Panel Report. Chest. 2020: 158: 1143‑1163. | Crossref
- Helms J, Tacquard C, Severac F, et al; CRICS TRIGGERSEP Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis). High risk of thrombosis in patients in severe SARS‑CoV‑2 infection: a multicenter prospective cohort study. Intensive Care Med. 2020; 46: 1089‑1098. | Crossref
- Klok FA, Kruip MJHA, van der Meer NJM, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID‑19. Thromb Res. 2020; 191: 145‑147. | Crossref
- Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio‑Thoracic Surgery (EACTS). Eur Heart J. 2021; 42: 373‑498.
- Harsch IA, Skiba M, Konturek PC. Severe acute respiratory syndrome coronavirus 2 pneumonia and pulmonary embolism in a 66‑year‑old woman. Pol Arch Intern Med. 2020; 130: 438‑439. | Crossref
ARTICLE INFORMATION