Subtle microvascular endothelial impairment in a young patient recovered from mild COVID-19



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Subtle microvascular endothelial impairment in a young patient recovered from mild COVID-19
COVID‑19, caused by SARS‑CoV‑2 infection, may induce significant cardiovascular conditions, including myocarditis, heart failure, severe arrhythmias, and thromboembolic complications. Importantly, increasing number of scientific reports indicate that SARS‑CoV‑2 affects microcirculation, causing serious dysfunction and inflammation of endothelial cells (endotheliitis) and, frequently, massive thrombosis in microvessels. Indeed, SARS‑CoV‑2 enters target cells via angiotensin‑converting enzyme 2 receptors, which are specifically extensively expressed on the surface of the lung epithelial and vascular endothelial cells in various tissues and organs.1 Due to accessibility of its assessment, peripheral microcirculation has been considered an indicator of systemic microvascular function.2
Laser speckle contrast imaging (LSCI) is a newly developed method based on speckle contrast analysis which allows for a noninvasive and real‑time microcirculation imaging over a wide area of tissue in response to a given stimulus.3 It shows an excellent reproducibility as well as very good spatial and temporal resolutions.4 Nowadays, we are also able to assess the changes in tissue biochemistry in vivo. A brand new technique, known as flow mediated skin fluorescence (FMSF) is based on monitoring the intensity of nicotinamide adenine dinucleotide (NADH) fluorescence on the forearm in response to blocking and restoring the blood flow.5 Therefore, FMSF enables noninvasive evaluation of the microvascular and metabolic regulation. Importantly, NADH is a major mitochondrial component, and plays a key role in cellular energy metabolism.5
A 36‑year‑old man, with unremarkable medical history, was referred to our cardiology outpatient clinic because of reduced exercise tolerance, shortness of breath, and fatigue, which had been continuing for about 2 months after COVID‑19. The molecular test performed in December 2020 using the real‑time reverse transcriptase–polymerase chain reaction yielded a positive result. However, besides general muscle weakness, the patient did not manifest any serious symptoms of infection. On admission, the levels of D‑dimer, B‑type natriuretic peptide, and cardiac troponin were within reference ranges. On 2‑dimensional echocardiography, normal left ventricular ejection fraction (65%) was noted, without regional dysfunction. Additionally, speckle tracking echocardiography showed normal (–22.4%) left ventricular global longitudinal strain (Figure 1A).
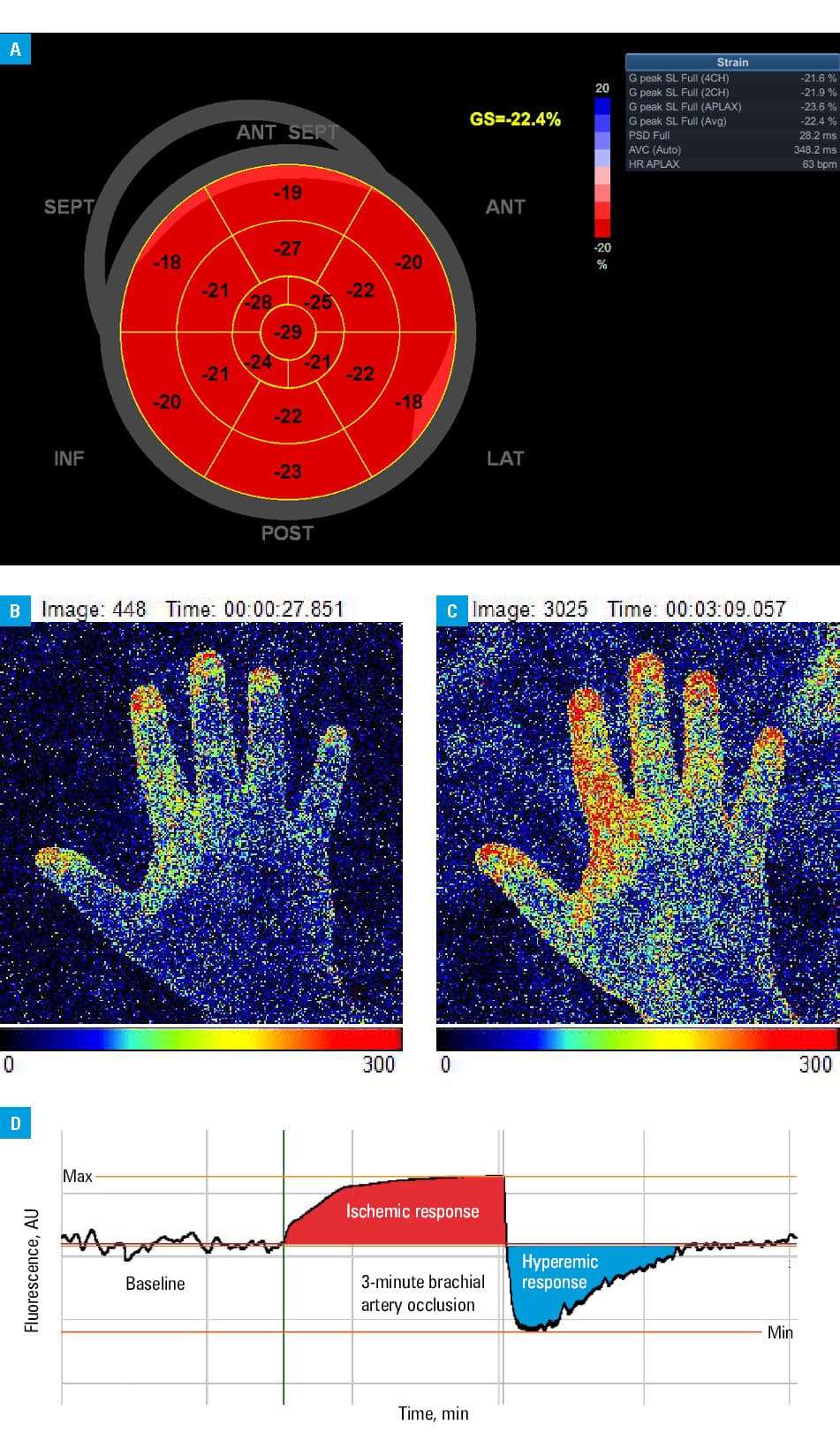
Abbreviations: Max, maximum; Min, minimum
We subsequently performed microcirculation measurements on the forearm during and following brachial artery occlusion simultaneously by LSCI (PeriCam PSI System, Perimed, Järfälla, Sweden) and FMSF (Angionica Ltd, Łódź, Poland). Speckle contrast analysis with colors ranging from blue (no perfusion) to red (high perfusion) showed basal microvascular perfusion (Figure 1B). A relatively weak postocclusive reactive hyperemic response was revealed by LSCI, suggesting a reduced endothelium‑dependent vasodilatation potential (Figure 1C). Likewise, using FMSF, we observed modest oscillations as well as slightly reduced ischemic and hyperemic responses. While hyperemic response reflects microvascular reactivity, ischemic response may mirror tissue sensitivity to hypoxia (Figure 1D).
To our best knowledge, this is the first report assessing microvascular and metabolic regulations in a patient recovered from COVID‑19. Indeed, accumulating evidence suggests that COVID‑19 is a systemic microvascular endothelial disorder with various clinical manifestations. Therefore, noninvasive, simple, and reliable methods for functional assessment of microcirculation are much needed.
- Varga Z, Flammer AJ, Steiger P, et al. Endothelial cell infection and endotheliitis in COVID‑19. Lancet. 2020; 395: 1417‑1418. | Crossref
- Hellmann M, Roustit M, Cracowski JL. Skin microvascular endothelial function as a biomarker in cardiovascular diseases? Pharmacol Rep. 2015; 67: 803‑810. | Crossref
- Pajkowski M, Chlebus K, Hellmann M. Microvascular endothelial dysfunction in a young patient with familial hypercholesterolemia. Pol Arch Intern Med. 2020; 130: 679‑680. | Crossref
- Roustit M, Cracowski JL. Assessment of endothelial and neurovascular function in human skin microcirculation. Trends Pharmacol Sci. 2013; 34: 373‑384. | Crossref
- Hellmann M, Tarnawska M, Dudziak M, et al. Reproducibility of flow mediated skin fluorescence to assess microvascular function. Microvasc Res. 2017; 113: 60‑64. | Crossref
ARTICLE INFORMATION