Risk factors and causes of early mortality in patients with newly diagnosed multiple myeloma in a “real-world” study: experiences of the Polish Myeloma Group
Key words: causes of death, comorbidities, early mortality, multiple myeloma



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Risk factors and causes of early mortality in patients with newly diagnosed multiple myeloma in a “real-world” study: experiences of the Polish Myeloma Group
Introduction: Despite the progress made in the treatment of multiple myeloma (MM), approximately 10% to 15% of patients die within the first year of diagnosis.
Objectives: The aim of the study was to determine risk factors of early mortality in patients with newly diagnosed MM treated with new drugs in clinical practice.
Patients and methods: This multicenter analysis included 197 patients with symptomatic MM, diagnosed between October 2006 and November 2019, with a survival of less than 12 months.
Results: The median overall survival was 2.5 months. The most common causes of early mortality were infections (35%), MM progression (23.8%), and cardiovascular disease (14.2%). In a multivariable analysis, the Zubrod performance score (P = 0.02), history of cardiovascular disease (P = 0.04), dependence on renal dialysis (P = 0.03), and MM response (P <0.001) were associated with early mortality.
Conclusions: Early mortality in MM patients requires further studies. When qualifying patients with newly diagnosed MM for chemotherapy, it is necessary to consider performance status and the history of comorbidities, including cardiovascular diseases.
What's new?
The use of proteasome inhibitors and immunomodulating drugs in the therapy of multiple myeloma (MM) resulted in the prolongation of overall survival. Approximately 10% to 15% of patients with MM die within 12 months of diagnosis. The most common causes of early mortality in our study group were infections, MM progression, and cardiovascular disease. In contrast, the most significant factors on early mortality were performance status, renal failure requiring dialysis, history of cardiovascular disease, and treatment effectiveness. The obtained results show how important it is to individualize the treatment of patients with MM.
Introduction
Multiple myeloma (MM) accounts for 1% of all cancers and about 10% of all hematological cancers.1 This hematological cancer is most common in the elderly, and the mean age of patients at diagnosis is approximately 65 to 74 years (median, 69 years).2 The incidence in Europe is 4.5 to 6/100 000/year.1 The introduction of new classes of drugs to the therapy of MM, such as proteasome inhibitors and immunomodulating drugs (IMiDs), changed the paradigm of treatment and improved long‑term survival in patients with MM over the past decade. Despite the prolongation of overall survival (OS), approximately 10% to 15% of patients with newly diagnosed (ND) MM die within 12 months of diagnosis.3,4 The causes and risk factors for early mortality (EM) are not fully understood in the age of new drugs. Early mortality is usually defined as death within 2 to 12 months of diagnosis.5,6 In the literature, 2, 6, or 12 months are also used, but it is generally death within 1 year of diagnosis which is accepted as a cutoff.7 Very EM (<2 months) in MM is associated with advanced age and poor patient performance status, as well as with limited use of new drugs.6 There are still little EM data in unselected real‑life patients with MM.4,6-10 Our study aimed to identify the causes of EM in patients with NDMM and clinical variables that can predict EM in MM.
Patients and methods
Patients
This retrospective study analyzed the records of 197 patients from 15 Polish sites who were started on therapy for symptomatic NDMM and died within 12 months of diagnosis between October 2006 and November 2019. We included patients who were initially treated with novel agents such as a proteasome inhibitor or IMiD. Patients diagnosed with monoclonal gammopathy of undetermined significance, asymptomatic MM, plasma cell leukemia, and patients who had an organ involvement with light‑chain amyloidosis at the time of diagnosis were excluded from the analysis. Treatment‑naïve patients with NDMM were also excluded.
Early mortality was defined as death within 12 months of diagnosis. Mortality rate and cause at 2, 6, and 12 months following the diagnosis were evaluated. Overall survival was defined as the period from the diagnosis of MM to death from all causes. The Zubrod performance score (ZPS) was used to assess patient performance status.11 Clinical staging of MM was performed using the International Staging System (ISS).12 The cytogenetic risk was classified as standard or high risk based on conventional cytogenetic studies or fluorescent in situ hybridization. High‑risk chromosomal abnormalities were defined as the presence of any of the following: t(4;14), t(14;16), t(14;20), or del(17p).13,14 Treatment outcomes were classified by the International Myeloma Working Group as complete response, stringent complete response, very good partial response, partial response, stable disease, and progressive disease.15 Overall response rate was defined as the proportion of all responses to at least partial response.
Local ethics committees approved the study in those sites where it was legally necessary. The study was carried out in accordance with the Declaration of Helsinki.
Statistical analysis
Statistical analysis and graphics were obtained using the statistical open source software Rstudio version 1.3.959 with a survival analysis package. The Kaplan–Meier method was used to assess survival and generate survival curves.16 The Cox proportional‑hazard regression method was used to fit univariable and multivariable survival models, the results of which are reported as hazard ratios (HRs) with 95% CIs. Variates with more than 50% of missing data were not included in the survival analyses. All reported P values are 2‑tailed and were considered significant if less than 0.05. Among the factors, those with P values of less than 0.05 were selected and included in the multivariable Cox regression analysis.
Results
Patient characteristics
Overall, the median patient age was 69 (range, 41–91) years, 126 (63.9%) patients were older than 65 years, and 55 (27.9%) patients were older than 75 years. There were 112 (56.8%) men. A total of 62 (31.5%) patients had ZPS 0 to 1, 120 (60.9%) patients had ZPS of more than 2, and the score of 15 (7.6%) patients was unknown. Two or more comorbidities were found in 106 (53.8%) patients. The most common comorbidities were: cardiovascular diseases found in 83 (42.1%) patients, arterial hypertension in 66 (33.5%) patients, and diabetes mellitus in 43 (21.8%) patients (diabetes coexisted with cardiovascular diseases in 38 [19.3%] patients). The coexistence of second cancer was found in 4 (2%) patients.
Using the ISS, 29 (14.7%), 20 (10.1%), and 118 (59.9%) patients were diagnosed with stages ISS‑1, ISS‑2, and ISS‑3 MM, respectively. In 30 (15.2%) patients, the ISS stage was unknown. A total of 100 patients (52.1%) had the immunoglobulin (Ig) G subtype of MM, 51 (24.4%) patients had the IgA subtype, 37 (15%) patients had light‑chain disease, and 9 (3.3%) patients had the IgM or IgD subtype. At the time of the MM diagnosis, 85 (43.1%) patients had renal impairment (RI), and 29 (14.7%) patients had extramedullary disease.
All patients were treated with regimens containing new drugs after the initial diagnosis. As the first‑line treatment, 80 (40.6%) patients received bortezomib‑based regimens, 49 (24.9%) were treated with bortezomib and IMiD‑based regimens, 43 (21.8%) solely with IMiD‑based regimens, and 25 (12.7%) according to other treatment protocols. A total of 127 (64.5%) patients received antiviral prophylaxis (acyclovir), and 94 (47.7%) received antibacterial prophylaxis (ciprofloxacin or trimethoprim‑sulfamethoxazole). Treatment efficacy was assessed in 179 (90.9%) patients. In the study cohort, overall response rate was 46.9% (3.3% complete response, 14% very good partial response, and 29.6% partial response). Stable disease was achieved in 48 (26.8%) patients. Baseline patient characteristics are shown in Table 1.
Characteristics | Whole group (n = 197) | Time of early mortality | ||||
<2 months (n = 90) | 2–6 months (n = 57) | >6–12 months (n = 50) | ||||
Data are presented as number (percentage) of patients unless otherwise indicated.
a Defined as presence of t(4;14), t(14;16), t(14;20) or del17p in the absence of any trisomy.
Abbreviations: Hb, hemoglobin; IgA, immunoglobulin A; IgG, immunoglobulin G; IMiD, immunomodulatory drug; ISS, International Staging System; LDH, lactate dehydrogenase; LLN, lower limit of normal value; ULN, upper limit of normal value | ||||||
Age, y, median (range) | 69 (41–91) | 72 (42–88) | 68 (44–91) | 62 (41–87) | ||
Age distribution | ≤65 y | 71 (36) | 23 (25.5) | 19 (33.3) | 29 (58) | |
66–75 y | 71 (36) | 34 (37.8) | 23 (40.4) | 14 (28) | ||
>75 y | 55 (28) | 33 (36.7) | 15 (26.3) | 7 (14) | ||
Sex | Male | 112 (56.8) | 48 (53.3) | 37 (64.9) | 27 (54) | |
Female | 85 (43.2) | 42 (46.7) | 20 (35.1) | 23 (46) | ||
Zubrod performance score | 0–1 | 62 (31.5) | 17 (18.9) | 18 (31.6) | 27 (54) | |
≥2 | 120 (60.9) | 65 (72.2) | 37 (64.9) | 18 (36) | ||
Not available | 15 (7.6) | 8 (8.9) | 2 (3.5) | 5 (10) | ||
Number of reported comorbidities | <2 | 91 (46.2) | 33 (36.6) | 25 (43.8) | 33 (66) | |
≥2 | 106 (53.8) | 57 (63.4) | 32 (56.2) | 17 (34) | ||
ISS stage | ISS‑1 | 29 (14.7) | 10 (11.1) | 9 (15.8) | 10 (20) | |
ISS‑2 | 20 (10.1) | 10 (11.1) | 5(8.8) | 5 (10) | ||
ISS‑3 | 118 (59.9) | 51 (56.7) | 38 (66.6) | 29 (58) | ||
Not done | 30 (15.2) | 19 (21.1) | 5 (8.8) | 6 (12) | ||
First‑line therapy | Bortezomib‑based | 80 (40.6) | 38 (42.2) | 27 (47.4) | 15 (30) | |
IMiD‑based | 43 (21.8) | 19 (21.1) | 7 (12.3) | 17 (34) | ||
Bortezomib + IMiD | 49 (24.9) | 18 (20) | 17 (29.8) | 14 (28) | ||
Others | 25 (12.7) | 15 (16.7) | 6 (10.5) | 4 (8) | ||
Multiple myeloma subtype | IgG | 100 (52.1) | 46 (51.1) | 32 (56.1) | 22 (44) | |
IgA | 51 (24.4) | 20 (22.2) | 14 (24.6) | 17 (34) | ||
Light‑chain disease | 37 (15) | 21 (23.3) | 7 (12.3) | 9 (18) | ||
Others | 9 (3.3) | 3 (3.3) | 4 (7) | 2 (4) | ||
Serum creatinine >2 mg/dl | 85 (43.1) | 46 (51.1) | 26 (45.6) | 13 (26) | ||
β2-microglobulin ≥5.5 mg/l | 118 (70.6) | 51 (73.9) | 38 (73.1) | 29 (65.9) | ||
Serum LDH | >ULN | 77 (39) | 37 (41.1) | 23 (40.3) | 17 (34) | |
Not done | 17 (8.6) | 11 (12.2) | 4 (7) | 2 (4) | ||
Serum calcium ≥11.5 mg/dl | 32 (16.2) | 11 (12.2) | 10 (17.5) | 11 (22) | ||
Hb <10 g/dl or >2 below LLN | 112 (56.8) | 53 (58.9) | 34 (59.6) | 25 (50) | ||
Cytogenetic data available | 59 (100) | 18 (20) | 21 (36.8) | 20 (40) | ||
Cytogenetic high‑risk categorya | 25 (69.2) | 5 (27.8) | 9 (15.8) | 11 (55) | ||
Causes and characteristics of early mortality
A total of 90 (45.7%) patients died within the first 2 months after the diagnosis, 57 (28.9%) patients died between 2 to 6 months, and 50 (25.4%) patients died between more than 6 to 12 months. In our study group, 134 (68.0%) deaths were related to nonmyeloma causes, 47 (23.8%) to progression or refractory MM, and 16 (8.1%) to unknown causes.
The main causes of EM in the study group were infections (69 [35%] patients) and refractory or progression MM (47 [23.8%] patients, including 29 with refractory MM).
The most common form of infection was septic shock with pneumonia, and the rate of death from infection remained constant for 6 months (38.9% at <2 months, 40.3% at 2–6 months) and then decreased (22% at >6–12 months). The cause of infection of 36 (52%) patients was confirmed microbiologically, and 12 (33.3%) of them had extended‑spectrum β-lactamase (ESBL)-positive Escherichia coli sepsis, and 7 (19.4%) had ESBL‑positive Klebsiella pneumoniae sepsis. The microbiological pathogens are summarized in Table 2.
Infectious causes of death | Value, n (%) |
Abbreviations: ESBL, extended‑spectrum β-lactamase | |
Confirmed microbiological diagnosis | 36 (52) |
Escherichia coli ESBL‑positive | 12 (17.4) |
Klebsiella pneumonia ESBL‑positive | 7 (10.1) |
Enterococcus faecium | 5 (7.3) |
Staphylococcus aureus | 4 (5.8) |
Pseudomonas aeruginosa | 3 (4.3) |
Acinetobacter baumani | 1 (1.4) |
Proteus mirabilis | 1 (1.4) |
Influenza virus | 2 (2.9) |
Pneumonary Aspergillosis | 1 (1.4) |
Unconfirmed microbiological diagnosis | 33 (48) |
In patients who died due to infection, prophylactic antibiotic therapy was administered to 22 (31.9%) patients. No information was obtained for 4 (5.8%) patients.
Death rate from disease progression was low for the first 6 months (14% at 2 months, 22.8% at 2–6 months) and then increased gradually. Between more than 6 to 12 months after the diagnosis, 42% of patients died due to MM progression.
In the group of patients who died in the first 2 months, the following causes of EM were found: infection in 35 (38.9%) patients, cardiovascular diseases in 18 (20%), MM progression in 13 (14.4%), RI in 4 (4.4%), other causes in 13 (14.4%), and unknown causes in 8 (7.7%).
Of the patients who died within 2 to 6 months, the following causes of EM were identified: infection in 23 (40.3%) patients, MM progression in 13 (22.8%), cardiovascular diseases in 6 (10.5%), RI in 4 (7%), other causes in 7 (12.3%), and unknown causes in 4 (7%).
For patients who survived more than 6 to 12 months, the causes of EM were as follows: refractory MM in 21 (42%) patients, infection in 11 (22%), cardiovascular diseases in 4 (8%), and other causes in 9 (18%), and unknown causes in 5 (10%).
The causes of EM were analyzed depending on age (≤65 vs >65 years). In the group of patients aged 65 years or younger, the following causes of EM were found: MM progression in 27 (41%) patients, infection in 20 (30.4%), cardiovascular diseases in 4 (6%), RI in 3 (4.5%), other causes in 9 (13.6%), and unknown causes in 3 (4.5%). In the group of patients older than 65 years of age, the causes of EM were as follows: infection in 49 (37.4%) patients, cardiovascular diseases in 24 (18.3%), MM progression in 20 (15.3%), RI in 5 (3.8%), other causes in 20 (15.3%), and unknown cause in 13 (9.9%).
Survival results and clinical variables associated with early mortality in patients with newly diagnosed multiple myeloma
The median OS was 2.5 months. Hazard ratios were calculated using univariable and multivariable analyses to validate the associations of clinical variables with EM.
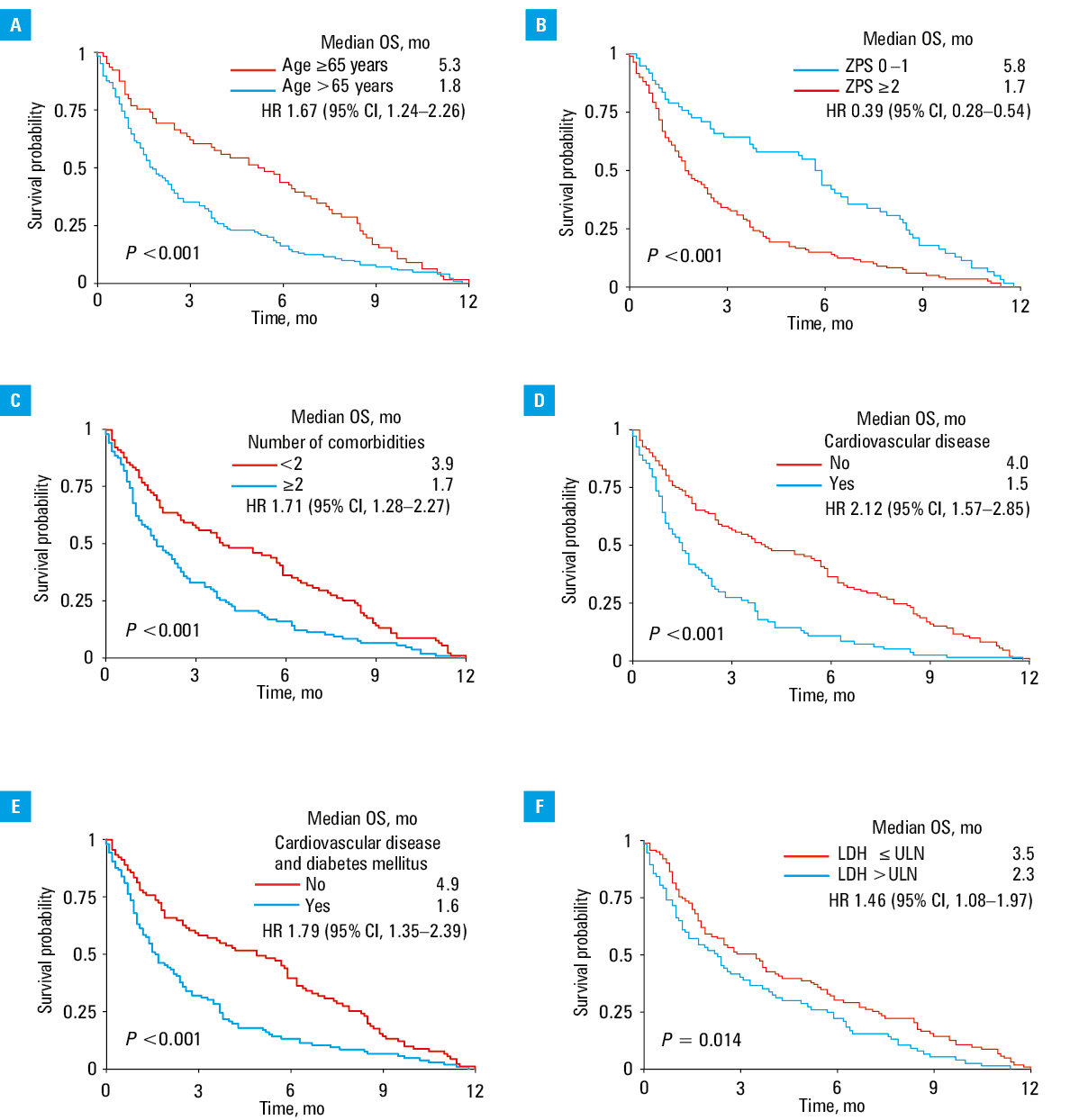
In the univariable analysis, 9 baseline factors were associated with EM (Table 3). Kaplan–Meier curves of selected baseline factors associated with EM (age, ZPS, number of comorbidities, history of cardiovascular diseases and diabetes mellitus, and serum lactate dehydrogenase [LDH] levels) are presented in Figure 1. Sex, disease stage, serum levels of albumin, β2‑microglobulin, calcium, creatinine as well as hemoglobin level, and platelet count were not associated with EM.
Predictor | Univariable analysis | Multivariable analysis | ||
HR (95% CI) | P value | HR (95% CI) | P value | |
Abbreviations: HR, hazard ratio; PR, partial response; others, see Table 1 | ||||
Age >65 y | 1.67 (1.24–2.26) | <0.001 | 1.11 (0.76–1.61) | 0.6 |
Male sex | 0.86 (0.65–1.15) | 0.33 | – | – |
Zubrod performance score >2 | 0.39 (0.28–0.54) | <0.001 | 0.62 (0.41–0.93) | 0.02 |
Number of comorbidities ≥2 | 1.71 (1.28–2.27) | <0.001 | 1.42 (0.94–2.15) | 0.1 |
History of cardiovascular disease | 2.12 (1.57–2.85) | <0.001 | 1.57 (1.01–2.54) | 0.04 |
History of cardiovascular disease and diabetes | 1.79 (1.35–2.39) | <0.001 | – | – |
Dependence on renal dialysis | 1.49 (1.05–2.14) | 0.03 | 1.7 (1.05–2.76) | 0.03 |
Hb <10 g/dl or >2 below ULN | 1.05 (0.78–1.39) | 0.7 | – | – |
Platelets <150 G/l | 1.17 (0.87–1.58) | 0.3 | – | – |
Serum creatinine >2 mg/dl | 0.71 (0.53–0.95) | 0.02 | 1.05 (0.7–1.57) | 0.8 |
Serum albumin <3.5 g/dl | 1.64 (0.66–4.06) | 0.28 | – | – |
Serum β2‑microglobulin ≥5.5 mg/l | 0.91 (0.6–1.37) | 0.66 | – | – |
Serum LDH level >ULN | 1.46 (1.08–1.97) | 0.01 | 1.09 (0.76–1.57) | 0.6 |
ISS‑3 | 1.22 (0.87–1.70) | 0.25 | – | – |
Cytogenetic high‑risk | 1.69 (0.98–2.8) | 0.05 | 1.29 (0.7–2.38) | 0.4 |
Response: ≥PR | 0.3 (0.21–0.43) | <0.001 | 0.33 (0.22–0.49) | <0.001 |
The 9 factors associated with EM (P <0.05) were included in the multivariable logistic regression analysis, and following a stepwise procedure, 4 variables were identified as associated with a higher likelihood of EM: ZPS greater than 2, history of cardiovascular diseases, dependence on renal dialysis, and no response to MM treatment (Table 3). In contrast, age above 65 years, comorbidities, RI (serum creatinine >2 mg/dl), high serum LDH levels, and cytogenetic risk were not associated with EM.
Discussion
The introduction of drugs with new mechanisms of action changed the paradigm of MM therapy’ and significantly improved patient outcomes. Recent studies have shown that new drugs used in patients with MM provide better survival, but EM in patients with MM is little understood. This problem is rarely analyzed in both phase III NDMM and real‑world studies. For this reason, we decided to explore Polish data for the causes of EM in the most frequently assessed periods, ie, 2 months, 6 months, and 12 months from the diagnosis.
In our study, the most common causes of death were infections (35% of patients), progression of MM (23.8% of patients), and cardiovascular disease (14.2% of patients). Our results corroborated those by Holmstreöm et al,9 who found that infections, cardiovascular failure, and RI were the most common causes of death.
In our study, infections accounted for 40% of all EM causes in the first 6 months after MM diagnosis and then decreased to 20% in the next 6 months. In half of the patients, the causes of infections were ESBL‑positive Enterobacteriaceae. Pneumonia, sepsis, and septic shock were the most common causes of EM infection, despite the fact that half of the patients were receiving prophylactic antibiotics, most commonly ciprofloxacin or trimethoprim‑sulfamethoxazole.
Due to the high rate of observed infections that cause EM, it is necessary to consider antibacterial prophylaxis, mainly as multiresistant sepsis is the most prevalent. Also, further research is required to determine the optimal prophylactic antibiotic and dosing regimen. Oken et al17 found that the use of trimethoprim‑sulfamethoxazole during the first 2 months of initial chemotherapy was effective prophylaxis in patients with early MM bacterial infection. By contrast, Vesole et al18 found that prophylactic antibiotic use in the first 2 months of treatment of NDMM (trimethoprim‑sulfamethoxazole or ciprofloxacin or placebo) did not affect the frequency of infections (20% vs 23% vs 22%, respectively; P = 0.95). On the other hand, the TEAMM (Levofloxacin Prophylaxis in Patients with Newly Diagnosed Myeloma) study showed that patients with MM treated with innovative treatment methods and who underwent prophylaxis with levofloxacin had a lower infection rate than those who did not receive prophylaxis (19% vs 27%; P = 0.002).19 In our study, two‑third of patients who died from an infection did not receive antibacterial prophylaxis. Although our group was relatively small, the use of prophylactic antibiotics during the first 2 to 6 months of MM treatment, especially in patients older than 65 years of age, seems to be of importance.
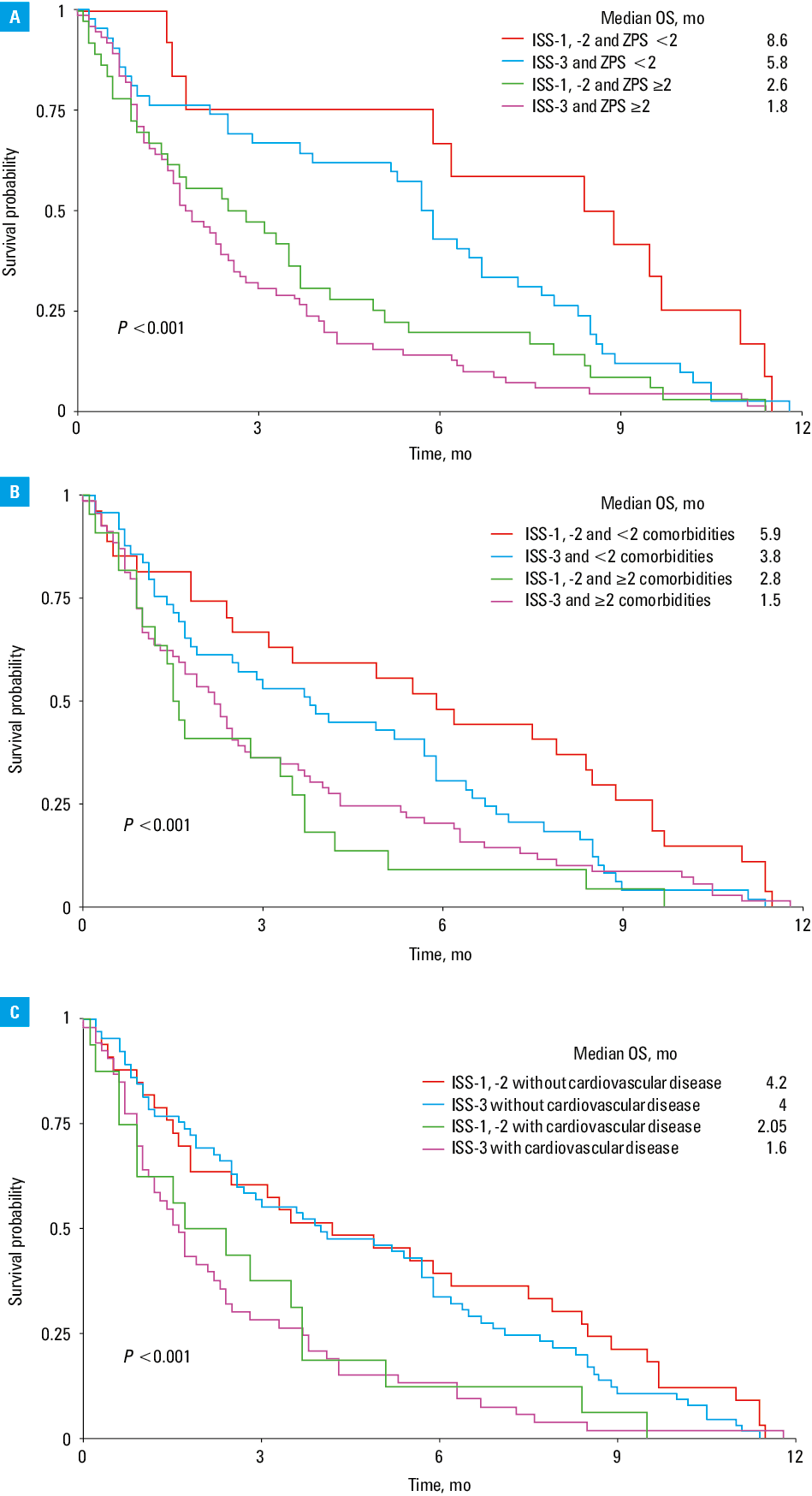
In addition to administering prophylactic antibiotics, identifying MM patients at high risk of EM is also essential. We observed that higher serum LDH (P = 0.01) and creatinine (P = 0.02) levels as well as dependence on renal dialysis (P = 0.03) increased the risk of EM. Similar results were obtained by Kumar et al,4 who found that low serum albumin (<3.5 g/dl), high serum β2‑microglobulin (>6.5 mg/dl), and high serum LDH (>180 IU/l) increased the risk of EM in patients with MM. These results suggest that more attention should be paid to MM patients with these unfavorable prognostic factors. The prognosis in NDMM depends on the stage of advancement, patient characteristics, disease biology, and treatment outcomes.20 Although 70% of patients with NDMM were diagnosed with ISS‑2 and ISS‑3, no significant differences were found in the analyzed 12 months of OS depending on the MM stage. It seems that patient‑related predictors, including ZPS, number of comorbidities, including cardiovascular disease, should be added to EM risk assessment (Figure 2).
This study had some limitations. First, it was a retrospective study, and the sample size was relatively small. Second, treatment regimens were relatively heterogeneous, making it challenging to analyze the association between induction treatment and EM in MM patients without confounders. Overall, our study showed that infections were the leading cause of EM. Higher LDH levels, high serum creatinine levels, high cytogenetic risk, and treatment response significantly impacted EM.
Apart from age, it seems that in addition to the factors listed above, EM is most influenced by general condition and the incidence of comorbidities, including heart disease and RI requiring dialysis. Also, antibiotic prophylaxis should be considered in patients with MM, especially those at high risk of EM. Further research is needed to identify the prognostic factors for EM in unselected patients with MM.
- Palumbo A, Bringhen S, Ludwig H, et al. Personalized therapy in multiple myeloma according to patient age and vulnerability: a report of the European Myeloma Network (EMN). Blood. 2011; 118: 4519‑4529. | Crossref
- Stat Fact Sheets SEER. Myeloma. http://seer.cancer.gov/statfacts/html/mulmy.html. Accessed February 14, 2021.
- Fonseca R, Bergsagel PL, Drach J, et al. International Myeloma Working Group molecular classification of multiple myeloma: spotlight review. Leukemia. 2009; 23: 2210‑2221. | Crossref
- Kumar SK, Dispenzieri A, Lacy MQ, et al. Continued improvement in survival in multiple myeloma: changes in early mortality and outcomes in older patients. Leukemia. 2014; 28: 1122‑1128. | Crossref
- Murakami H, Hayashi K, Hatsumi N, et al. Risk factors for early death in patients undergoing treatment for multiple myeloma. Ann Hematol. 2001; 80: 452‑455. | Crossref
ARTICLE INFORMATION