Behavioral factors and the risk of viral infection: essential aspects during the COVID‑19 pandemic
Key words: COVID-19, diet, habits, health behavior, obesity



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Behavioral factors and the risk of viral infection: essential aspects during the COVID‑19 pandemic
The current COVID‑19 pandemic has been continuing for over 11 months. Several nutritional and behavioral aspects have been associated with an increased inflammatory state or oxidative stress, which could negatively affect the course of COVID‑19. Previous research showed that metabolic diseases, including obesity or type 2 diabetes mellitus (T2DM), in which proper diet is especially important, increase the risk of COVID‑19 and can exacerbate its course. This should be taken into account particularly in the areas with high prevalence of obesity and T2DM, such as the Western countries. In our paper, we briefly summarized the harmful and beneficial nutritional and behavioral aspects that are essential during the COVID‑19 pandemic and which are present in particular among patients with obesity and T2DM.
Introduction
According to the reports of the World Health Organization (WHO), we can constantly observe a growing number of new confirmed cases of COVID‑19. Currently, over 120 million cases have been confirmed, with almost 3 million deaths worldwide.1 Obesity and diabetes constitute recognized risk factors of upper respiratory tract infections and, as shown in recent studies, can be associated with a more severe course of COVID‑19.2,3 Patients with a BMI higher than 35 kg/m2 presented a higher risk of admission to an intensive‑care unit (ICU) among all hospitalized patients in the United States.4 Moreover, in France, almost 48% of ICU patients had a BMI exceeding 30 kg/m2, whereas over 28% of such patients showed a BMI higher than 35 kg/m2.5 In fact, patients undergoing invasive mechanical ventilation had an average BMI equal to 31.1 kg/m2, while those without invasive mechanical ventilation presented lower BMI values (mean, 27 kg/m2).5 The rate of diabetic individuals admitted to hospital with severe COVID‑19 varied from 11% to 35.5% depending on the source.6,7 Although the prevalence of type 2 diabetes mellitus (T2DM) in COVID‑19 patients could be lower than in the general population, recent research demonstrated that diabetes was associated with worse prognosis and more severe course of the disease.8,9 Moreover, diabetic patients were more likely to have severe complications and showed a higher risk of death due to infection.
On the other hand, it is essential to bear in mind that the global lockdown has resulted in major changes both in the dietary and behavioral patterns, which, among other aspects, have led to weight gain; for example, almost 30% of the studied adults in Poland noticed an increase in weight during lockdown.10 Furthermore, rapid spread of SARS‑CoV‑2 forced the authorities of many countries to implement social isolation of their citizens. These actions were intended to decrease the number of new cases; however, they were also the cause of numerous lifestyle changes. In fact, isolation, lockdown, and the impossibility to use public sports facilities, as well as the unstable economic situation significantly influenced the lifestyle behaviors worldwide.11,12 During isolation, the level of physical activity decreased by 27%, whereas the consumption of unhealthy food, snacking, or uncontrolled food intake increased.13 Since obesity and T2DM are strongly associated with nutritional and lifestyle factors, preventive strategies should focus also on behavioral approach. In our paper, we described selected potentially harmful and healthy behavioral factors which can be crucial during the COVID‑19 pandemic. However, it should be noted that studies evaluating the influence of diet, dietary habits, and behavior on the risk of COVID‑19 and its course are scarce. Our review discusses the few available reports and is mostly based on studies focused on other viral infections.
Harmful behavioral approaches during the COVID‑19 pandemic
Harmful diets and eating habits
Several studies suggested that high levels of systemic adipose tissue and intestinal inflammation are responsible for the severity of COVID‑19.14,15 An excessive amount of adipose tissue is associated with the synthesis of proinflammatory cytokines, as well as adipokines, and can lead to inflammation and oxidative stress. However, these 2 factors can be both the result and the cause of obesity. Although oxidative stress is present during infectious diseases, its impact on the severity of the disease is not fully understood; however, several pathological processes during infection are associated with oxidative stress, and increased generation of the reactive species can result in fatal outcomes.16
Several dietary patterns can contribute to an increased inflammatory state and oxidative stress. Oxidative stress activates the inflammatory kinases and can affect insulin signaling, leading to diabetes. In a study by Gil‑Cardoso et al17 based on an animal model, the consumption of a high‑fat (45%–53% kcal from fat) and high‑fructose diet—a cafeteria (CAF) diet—was a possible cause of intestinal oxidative stress, not obesity itself. Additionally, the CAF diet was associated with increased production of reactive oxygen species, tumor necrosis factor α (TNF-α), and myeloperoxidase in the intestinal area. Interestingly, increased oxidative stress was observed after approximately 17 weeks, while increased inflammation was seen earlier. Moreover, significant gut dysbiosis could also be associated with food additives, as well as the deficiency of minerals and vitamins.18 On the other hand, a Western‑style diet (WD) most effectively induced obesity and its comorbidities, independently of major dysbiosis, when compared with the CAF diet, high‑fat diet (HFD), or low‑fat diet. Maternal consumption of a CAF diet during lactation in rats resulted in an impaired metabolic health of their offspring which was independent of a higher body weight, although accompanied by a higher fat accumulation.19 Additionally, the CAF diet increased oxidative damage in the white adipose tissue, which could disrupt tissue homeostasis.20 According to Bortolin et al,21 the major cause of changes in the microbiota was the CAF diet, not obesity. It could be an essential observation, since gut microbiota dysbiosis was found to be linked with obesity and diabetes.22
Among other elements, the WD is characterized by a high intake of simple sugars and saturated fatty acids (SFAs)—this dietary pattern is mostly seen in the developed or developing Western countries. A high intake of SFAs and simple sugars activates the innate immune system leading to chronic inflammation and, subsequently, to an impaired viral defense mechanism. Moreover, a high intake of SFAs activates the toll‑like receptor 4 on neutrophils and dendritic cells, which leads to chronic low‑grade inflammation.23 Mice fed with an HFD and a high‑SFAs diet presented an increased level of macrophages in the lungs which consequently led to an increased level of inflammation in the respiratory tract. Additionally, the HFD increased the infiltration of macrophages into the lung tissue, particularly to the alveoli.24 A decreased level of T‑lymphocytes, CD4 and CD8+ lymphocytes, as well as an increased level of proinflammatory Th17 cells in CD4 cells and high cytostatic CD8+ cell activity suggest a more severe COVID‑19 course.25 What is more, the WD inhibits the function of T‑lymphocytes by means of an increase in oxidative stress which, in turn, affects the growth and proliferation of T- and B‑lymphocytes and induces apoptosis.26 It is also associated with a higher prevalence of obesity and diabetes, and patients with these diseases are particularly susceptible to COVID‑19.27
Alcohol use and the risk of infection
Alcohol is the most consumed psychoactive substance worldwide; actually, it is estimated that about 2.4 billion people (1.5 billion men and 0.9 billion women) consume alcohol. In the Western countries, 8 to 12 liters of alcohol per citizen are consumed every year.28 Alcohol sale and consumption have increased during the COVID‑19 pandemic, which could be explained by the extended time spent in social isolation, depression, loneliness, or financial problems.29 However, it should be noted that an increase in alcohol sale cannot be used to reliably assess the overall alcohol consumption, since places where alcohol used to be regularly consumed (eg, pubs, clubs, restaurants) were closed during lockdown.30 It is vital to bear in mind that alcohol abuse can lead to serious health consequences, both functional and psychiatric, and can increase the number of falls, thus predisposing to injuries.31 Elderly patients with several comorbidities, including obesity, diabetes, cardiovascular disease, and liver or autoimmune diseases are especially exposed to the harmful influence of alcohol use. Additionally, these patients are likely to contract COVID‑19 more frequently, and its course tends to be more severe, often associated with acute respiratory distress syndrome and a need for mechanical ventilation. In addition, abusive alcohol use is associated with an increased risk of viral and bacterial infections. In a meta‑analysis by Simou et al,32 alcohol use increased the risk of community‑acquired pneumonia (CAP) by 83%, as compared with the nondrinking or less‑drinking individuals (relative risk, 1.83; 95% CI, 1.3–2.57). Additionally, every 10 to 20 g of ethanol increased the risk of CAP by 8%. In fact, Testino et al33 demonstrated an additional correlation between alcohol doses and viral infections. Chronic excessive alcohol use can modulate both the innate and acquired immunity. Ethanol may disrupt the ability of immunological cells to recruit natural killer cells and thus inhibit the phagocytosis or inflammatory response mechanisms.34 Alcohol affects natural killer cells by binding with target cells, changing the profile of secreted cytokines and influencing cytolytic activity.34 Additionally, chronic alcohol use can increase the risk of severe influenza and elevate mortality levels by affecting the response of CD8+ lymphocytes.35 In fact, alcohol consumption leads to a decrease in the level of T‑lymphocytes and affects their functioning. What is more, it decreases the number of B‑lymphocytes, affecting at the same time the production of immunoglobulins. It is also associated with the production of proinflammatory cytokines—mostly interleukin (IL) 1, TNF-α, and IL‑6—which are essential in the inflammatory processes in the lung tissue during SARS‑CoV‑2 infection.36 Among other mechanisms, alcohol can reduce tension in the nasopharynx, which is associated with an increased risk of microaspiration affecting the function of the macrophages and causing undernutrition.32 SARS‑CoV‑2 binds with the angiotensin‑converting enzyme 2 (ACE‑2) receptor; therefore, the increased expression of this enzyme can be a risk factor of cell infection. In the process of invasion of the respiratory epithelium, SARS‑CoV‑2 binds to the cell surface of ACE‑2, hence an increase in the expression of this enzyme may be a factor contributing to cell attack. Thus, it can be suggested that diabetic patients prone to chronic alcohol consumption, in whom both the impairment of immune response and cytokine storm are observed, are more susceptible to infection and more severe course of the disease.37,38 What is more, alcohol use can affect and disrupt blood glucose and insulin profiles.39 Although data regarding the association between blood glucose profile and the course of COVID‑19 are imprecise and frequently contradictory, there are many reports concerning severe acute respiratory syndrome and H1N1 influenza in which patients with poorer glycemic control presented an increased risk of infection and death.40,41
Preventive measures during the COVID‑19 pandemic are particularly necessary; thus, a reduction in alcohol use (to a maximum of 1 drink per day) or total abstinence is recommended, especially among high‑risk patients.
Healthy behavioral approaches during the COVID‑19 pandemic
During the pandemic, an immunological response is necessary for the prevention of infection. A deficiency of protein, antioxidative vitamins, zinc, or vitamins A and D can decrease the immunological response. On the other hand, high intake of fiber has a protective effect on the course of infection.42 It is worth noticing that the abovementioned deficiencies are usually present in patients with obesity and diabetes.43
Body weight reduction and COVID‑19
Oxidative stress and inflammation can modify the response of the immune system to infection. Chronic low‑grade inflammation leads to impaired immunological response, increasing the risk of infection, including that with SARS‑CoV‑2.44 It is worth bearing in mind that obese people show higher leptin concentrations and lower adiponectin concentrations, which can also lead to impaired function of the immune system. Additionally, as mentioned before, research indicates that in people with obesity influenza lasts for a longer period than in individuals with normal body weight.45 Hence, it seems that body weight reduction could constitute another essential aspect in the prevention of COVID‑19, as well as other infections. What is more, body weight reduction leads to a decrease in the levels of inflammatory state markers and oxidative stress.46 Additionally, weight reduction among patients with overweight or obesity leads to a decrease in C‑reactive protein (CRP) concentration. In fact, Rejeski et al47 noticed that reductions in CRP concentrations were greater when weight reduction was combined with resistance training. Moreover, it has been shown that in Italy, COVID‑19 patients with overweight and obesity were younger than patients with normal body weight and they more frequently required ventilation and admission to an ICU.48 It is essential to remember that body weight reduction has several health benefits, including reduced cardiovascular risk and improved insulin sensitivity.49 Taking into account the abovementioned facts, weight loss among overweight and obese patients should be recommended in order to decrease the risk of viral infection, possibly including infection with SARS‑CoV‑2.
Vegetarian diet
Vegetarian and vegan diets, which eliminate some or all animal‑based products, have been gaining popularity, also in the Western countries. A healthy vegetarian diet, rich in whole grain products, fresh fruit and vegetables as well as coffee or tea, could reduce the inflammatory state assessed by the concentration of high‑sensitivity CRP (hs‑CRP) and transforming growth factor β.50 Additionally, vegetarian diet can influence adipose tissue inflammation by reducing femoral adipose tissue macrophage.51 On the other hand, a study by Menzel et al52 showed no differences between vegans and omnivores in the levels of inflammatory markers, for example, adiponectin, intracellular adhesion molecule 1, IL‑18, IL‑1 receptor agonist, omentin 1, or resistin. Currently, there are no studies investigating the association between the adherence to a vegetarian diet and the risk for, or the course of COVID‑19; however, there is an urgent need to perform large cohort studies comparing the effects of a Western vegetarian diet and the traditional Western diet on the prevalence of COVID‑19.
Mediterranean diet
The Mediterranean Diet (MeD) is characterized by a high intake of whole grain products, vegetables, fruit, olive oil, nuts, fish, and—in moderate quantities—red wine. On the other hand, red meat, dairy products, sweets and refined products are consumed less frequently.53 This diet is rich in vitamins C, D, and E as well as in zinc, calcium, iron, and other anti‑inflammatory and immunosuppressive nutrients.54 In fact, the dietary inflammatory index score was lower for the MeD than for a low‑fat diet. Additionally, individuals with coronary heart disease who followed the MeD had lower levels of high‑sensitivity IL‑6 and higher levels of hs‑CRP, both of which were statistically insignificant.55 Similarly, Michalsen et al56 did not observe any essential changes in hs‑CRP, fibrinogen, fasting insulin, lipids, and fatty acids concentrations in patients with coronary heart disease following the MeD. However, strict adherence to the MeD was found to be associated with lower CRP, IL‑6, homocysteine, and fibrinogen concentrations in comparison with lower adherence.57 It has been noticed that the concentrations of oxidised low‑density lipoprotein significantly decreased among individuals following a vitamin E–enriched MeD when compared with those adhering to a high‑fat WD. What is more, the vitamin E–enriched MeD reduced postprandial risk factors of cardiovascular disease, such as oxidised low‑density lipoprotein, and the expression of inflammation- and oxidative stress–related genes.58 Additionally, according to the study by Casas et al,59 the MeD, supplemented with extra virgin olive oil or nuts, was associated with a significant decrease in the levels of inflammatory biomarkers, such as CRP and IL‑6, when compared with a low‑fat diet. Concentrations of hs‑CRP, IL‑6, IL‑7, and IL‑8, as well as insulin resistance decreased among individuals following the MeD.60 Moreover, there were no differences in body weight among obese patients following a low‑calorie vegetarian diet and low‑calorie MeD. Di Daniele et al61 demonstrated that higher adherence to the MeD resulted in reduced body weight and adipose tissue content, particularly visceral fat, which could lower the risk of metabolic diseases and have a positive impact on their course. It was reported that during the COVID‑19 pandemic in Italy, more citizens followed the MeD, especially in the northern and central part of the country, where the citizens presented with lower BMI values. In fact, research suggests that the MeD is one of the most optimal and beneficial dietary patterns and could constitute a supportive treatment of COVID‑19.62 However, it should be noted that despite the beneficial influence of the MeD on the immune system and metabolic disorders, the morbidity and mortality of COVID‑19 were high in Italy and Spain where this diet is frequently followed.
Vitamin D and zinc
Sufficient concentration of vitamin D is essential for a proper functioning of the immune system, and the association between the vitamin D status and the risk for and course of COVID‑19 has been highly discussed.63 Exposure to sunlight is an essential and the most important contributor to the production of vitamin D in the human body. Although vitamin D can be found in several food products, its concentrations in nonfortified products are generally insufficient in ensuring its proper status and additional supplementation is needed and encouraged. It should be highlighted that limited outdoor activity is associated with decreased sun exposure, resulting in deficiency in vitamin D which protects from viral infections by producing cathelicidins and defensins as well as decreasing the inflammatory cytokines. As shown in the current studies, the levels of outdoor activity are much lower during lockdown.10,64 Moreover, vitamin D concentrations are usually lower among the aging population or individuals with obesity, and those groups are also more vulnerable to COVID‑19.65 In a systematic review and meta‑analysis by Pereira et al,66 vitamin D deficiency—observed more frequently (by 64%) in severe than in mild cases—was not associated with increased risk of COVID‑19; however, insufficient vitamin D concentration increased the rates of hospitalization and mortality from COVID‑19. Similar results were observed in other studies.67,68 Moreover, a negative correlation between mean concentration of vitamin D and the number of COVID‑19 cases was observed.69
Zinc is an important trace element in developing and maintaining a proper immune function; its deficiencies may alter the humoral and cell‑mediated immunity and increase the risk of infectious disease.70 Moreover, it maintains the integrity of the skin and mucosal cell membrane and protects cells from oxidants.71 It was shown that the intake of zinc from poultry, red meat, nuts, and pulses was associated with milder course of severe acute respiratory syndrome.72 It can be assumed that proper status of zinc could be important during SARS‑CoV‑2 infections, and its deficiency could worsen the course of COVID‑19. Several clinical trials investigating the efficacy and influence of drugs or nutritional supplements with zinc on COVID‑19 patients have been conducted; however, in most of them, the results regarding the influence of zinc on individuals with COVID‑19 are not available yet (eg, NCT04323228; NCT04342728; NCT04468139).
Gastrointestinal problems, intestinal microbiota, and COVID‑19
It is essential to remember that COVID‑19 can be associated with several gastrointestinal problems that affect around 5% to 50% of patients—the receptor for coronavirus is ACE‑2, which is also present in the cells of the digestive system (enterocytes, colonocytes, stomach mucosa, and esophageal cells).73 Currently, there are only a few studies assessing the mutual influence between the course of COVID‑19 course and gut microbiota. “Healthy” microbiota provide vitamins, maintain the integrity of the mucosal barrier, regulate host immunity, and are, alongside with the immune system, the first‑line defense against pathogens; therefore, they protect from the development of several diseases.74 Their antimicrobial function is based on the production of substances like bacteriocin and strife for the limited nutrients that inhibit pathogen colonization.75,76 Gut microbiota are also associated with the innate immune system of intestinal mucosa due to direct interactions with epithelial cells.75,77
Data from China showed that in some patients with COVID‑19 there was a dysbiosis of the gut microbiota, with lower amounts of Lactobacillus and Bifidobacterium.78,79 Shen et al80 reported that microbiota in patients infected with SARS‑CoV‑2 and those with CAP were similar, with the advantage of pathogens or increased levels of upper and oral respiratory commensal bacteria. In China, 58% to 71% of COVID‑19 patients received antibiotics and diarrhea occurred in 2% to 36% of patients.81,82 However, even though probiotic administration is useful, it is unlikely to have a direct effect on COVID‑19 severity.79 In the case of antibiotic use, probiotic treatment was recommended in order to strengthen the composition of gut microbiota. In 2 meta‑analyses, minor effectiveness of probiotic administration in decreasing the frequency and duration of respiratory tract viral infection was shown.82,83 According to the current data, about 2% to 47% of infected patients require invasive mechanical ventilation.81,84 In 2 independent randomized‑controlled trials, probiotic administration (Lactobacillus rhamnosus GG, live Bacillus subtilis, and Enterococcus faecalis) was associated with a less severe course of ventilator‑associated pneumonia compared with placebo among critically ill patients.85,86
Nutrients can promote or inhibit microbial growth, and dietary patterns significantly affect the composition of gut microbiota. Although a strict association between gut microbiota and COVID‑19 is not known yet, focusing on the proper diet in order to enhance the gut microbial composition seems reasonable. Dietary fiber, fermented food and nonalcoholic beverages, plant protein, and the MeD have a favorable effect on intestinal microbiota. On the other hand, the consumption of the WD, animal protein, saturated fatty acids, and simple sugars should be limited, since they affect intestinal microbiota in a negative way.87
Diet, COVID‑19 symptoms, and pharmacological treatment
Apart from respiratory symptoms and illnesses, other systemic disorders caused by SARS‑CoV‑2 infection may be noticed—symptoms may include nausea, vomiting, diarrhea as well as loss of taste and smell.88-90 Interestingly, olfactory dysfunction can be considered an early predictor for lower severity of COVID‑19.91,92 Among the Polish population, at least a single gastrointestinal symptom was reported in more than half of the patients, and almost 50% reported olfactory and taste disorders.93 Moreover, lack of appetite and diarrhea were reported by 17.6% of COVID‑19 patients. Interestingly, those symptoms were significantly higher among women than men. In the case of olfactory dysfunction, olfactory training (repeated and deliberate sniffing of a set of odorants for 20 seconds each at least twice a day for 3 months or longer) can be considered among patients with COVID‑19 since it was reported to improve postinfectious smell dysfunctions.94,95 Moreover, among patients who had undergone endoscopic resection of sellar and parasellar masses, omega‑3 supplementation possibly protected from olfactory loss; however, these results were not confirmed in patients with SARS‑CoV‑2 infection.96
Currently, the pharmacotherapeutic protocol for patients with mild and moderate COVID‑19 course includes corticosteroids (dexamethasone, methylprednisolone), remdesivir, tocilizumab, and nonsteroidal anti‑inflammatory drugs (for treatment of fever).97 However, all these drugs can also negatively affect the gastrointestinal system. For example, according to the product characteristics, remdesivir can increase liver parameters (alanine aminotransferase and aspartate aminotransferase), and the uncommon side effects of tocilizumab include diverticulitis, stomach ulcer, swollen red areas in the mouth, and gastritis. Commonly, diarrhea and stomach pain may occur. Moreover, metamizole—used for the treatment of fever—can also cause diarrhea. On the other hand, the use of corticosteroids can increase the risk of ulcer disease. However, due to the nature of the disease and the risk of cytokine storm and severe respiratory failure, all of the treatment recommendations should be followed (accordingly to the severity of the disease), and nutritional support should be implemented if necessary.
Therefore, considering the adverse effects of pharmacotherapy and the high frequency of gastrointestinal symptoms among patients with COVID‑19, appropriate food intake can be disrupted, thus affecting the nutritional status. In this regard, several dietary approaches (presented in Table 1) could be proposed to reduce the severity of symptoms. A proper energy intake, adjusted to the body’s needs, is associated with proper immune response against a viral infection. Furthermore, SARS‑CoV‑2 infection may negatively impact the nutritional status and increase the risk of malnutrition.98,99 Undernourished patients have decreased muscle strength and mass, which can impact the function of respiratory muscles. When a patient is not able to meet the dietary requirements and sustain a proper nutritional status, oral nutritional supplements (ONS) should be considered. This recommendation particularly refers to hospitalized and older individuals. In these 2 groups of patients with a good prognosis, enteral nutrition (EN) should be introduced regardless of the nutritional state, in case they are unable to consume a sufficient amount of energy via the oral route. However, if EN is contradicted or insufficient, parenteral nutrition (PN) should be considered. Consequently, if COVID‑19 patients cannot reach the recommended caloric intake, ONS should be introduced, and if this measure is not sufficient, EN or PN should be implemented.100 According to the American Society for Parenteral and Enteral Nutrition, early introduction of EN is recommended in every COVID‑19 patient requiring intensive care. The treatment should start within the first 36 hours since admission to the ICU or within the first 12 hours since the initiation of mechanical ventilation. If EN is not possible, PN should be used, especially among high‑risk patients.
Symptom | Nutritional and behavioral approaches |
Note: nutritional screening tools must be used among hospitalized patients and considered among patients with mild and moderate course of the disease, especially when they experience weight loss. | |
Nausea and vomiting |
|
Diarrhea |
|
Loss of smell and / or taste |
|
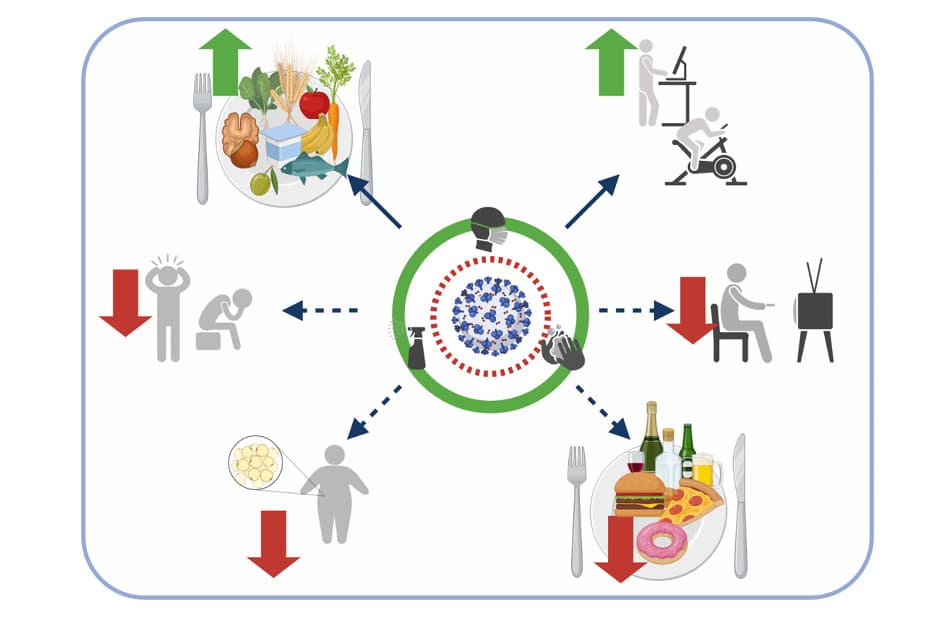
Conclusions
Due to the fact that obesity, T2DM, and SARS‑CoV‑2 infection have all been associated with behavioral risk factors, it is crucial to adopt proper nutritional and lifestyle approaches (Figure 1). Furthermore, according to the dietary recommendations, a physically active lifestyle is also vital, as it may potentially prevent SARS‑CoV‑2 infection and accelerate recovery from COVID‑19. Since all of these diseases are accompanied by inflammation and oxidative stress, an anti‑inflammatory diet, rich in whole grain products, dairy, plant protein, as well as fresh fruit and vegetables, should be implemented in the groups of patients at high risk. Additionally, it is beneficial to avoid the WD due to its negative influence on viral defense mechanism. In conclusion, a strategy for combating obesity and tackling the increasing occurrence of T2DM, which would include behavioral approaches, is particularly necessary during the COVID‑19 pandemic. Promoting healthy diet by means of nutrition education should be performed mainly in the Western countries, where a high consumption of the WD increases the risk of SARS‑CoV‑2 infection, thus, indirectly, also potentially increasing the risk of COVID‑19. This field, however, requires further research.
Practical behavioral recommendations are summarized below.
-
During the pandemic, focus on your diet and lifestyle behaviors as they are essential in the prevention of COVID‑19 and may affect its course.
-
Pay attention to alcohol consumption, as there may be a chance it has increased during the COVID‑19 pandemic. Try to limit it to 1 drink per day.
-
Consider the supplementation of vitamin D; although it can be synthesized in the skin from May to September (in Poland), you possibly do not meet the criteria for the proper synthesis due to lower outdoor activity or remote working. Consult with your healthcare provider in order to establish the correct dosage.
-
Try for your diet to include food products rich in fiber, zinc, iron, and vitamins (especially A, C, D, and E) and try to increase the consumption of fresh vegetables and fruit. Include vegetable oils in your diet and try to limit the consumption of processed food, sweets, and sweetened beverages (you may replace them with those sweetened with low‑calorie sweeteners). Remember: these small actions may improve your health and immune system.
-
If your BMI is higher than 24.99 kg/m2 (especially when it exceeds 29.99 kg/m2), try to focus on your diet, also in the context of the number of calories you consume. Decrease it by 10% to 20% and introduce regular physical activity adjusted to your preference, abilities, and government restrictions. Remember: even a small reduction in body weight may positively influence your health and improve the course of potential SARS‑CoV‑2 infection—try to take care of it from now on.
- World Health Organization. Weekly Operational Update on COVID‑19. https://www.who.int/publications/m/item/weekly‑operational‑update‑on‑covid‑19–-5‑april‑2021. Accessed April 5, 2021.
- Milner JJ, Rebeles J, Dhungana S, et al. Obesity increases mortality and modulates the lung metabolome during pandemic H1N1 influenza virus infection in mice. J Immunol. 2015; 194: 4846‑4859. | Crossref
- Rychter AM, Zawada A, Ratajczak AE, et al. Should patients with obesity be more afraid of COVID‑19? Obes Rev. 2020; 21: e13083. | Crossref
- Kalligeros M, Shehadeh F, Mylona EK, et al. Association of obesity with disease severity among patients with COVID‐19. Obesity (Silver Spring). 2020; 28: 1200‑1204. | Crossref
- Simonnet A, Chetboun M, Poissy J, et al; LICORN and the Lille COVID‑19 and Obesity study group. High prevalence of obesity in severe acute respiratory syndrome coronavirus‑2 (SARS‑CoV‑2) requiring invasive mechanical ventilation. Obesity (Silver Spring). 2020; 28: 1195‑1199. | Crossref
ARTICLE INFORMATION