Coinfection of COVID-19 and pneumocystosis in a patient after kidney transplantation



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Coinfection of COVID-19 and pneumocystosis in a patient after kidney transplantation
COVID‑19 is a worldwide pandemic caused by SARS‑CoV‑2. Typical findings on chest high resolution computed tomography (HRCT) include appearance of crazy paving and diffuse peripheral ground‑glass opacities.1 The CORADS classification is a standardized system for the radiologists to describe the level of suspicion of the infection.2 Pneumocystosis is a fungal opportunistic infection caused by Pneumocystis jiroveci. Typical findings on computed tomography are very similar to COVID‑19; however, ground‑glass opacities are characterized by a central distribution.3
A 47‑year‑old man after kidney transplantation in 2009 was hospitalized at a district hospital due to COVID‑19 confirmed by a polymerase chain reaction test. HRCT showed bilateral diffuse interstitial changes including ground‑glass opacities and crazy paving localized peripherally, corresponding to CORADS 5. Blood tests showed a stable level of creatinine (1.2 mg/dl; reference range <1.0 mg/dl) and an elevated C‑reactive protein level (67 mg/l; reference range <5 mg/l). Dexamethasone and antibiotic therapy with clarithromycin and ceftriaxone followed by meropenem were started. Acute kidney injury (creatinine level, 3.2 mg/dl), caused by an interaction between clarithromycin and ciclosporin, was observed and the patient was transferred to a COVID‑19 designated ward at a university hospital for further management.
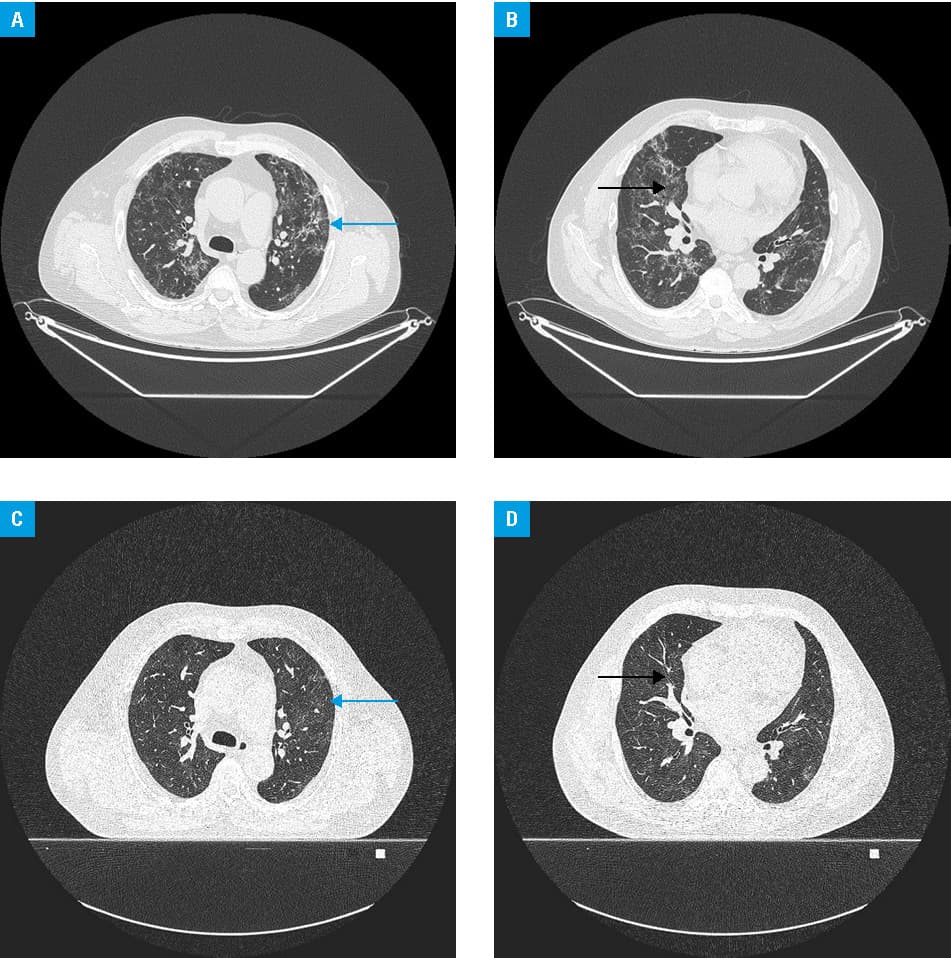
In the beginning, the clinical course of the patient after the admission was uneventful. Creatinine levels normalized and meropenem was discontinued. However, despite a decrease in C‑reactive protein levels, fever and cough persisted. Additional tests of blood and urine and repeated HRCT were performed. The test for CMV pp65 antigen was negative, although pneumocystosis immunoglobulin (Ig) G antibodies were positive with a borderline titer of IgM antibodies. Stenotrophomonas maltophilia growth was found in urine culture. HRCT showed ground‑glass opacities with central distribution typical of pneumocystosis and some located peripherally typical of COVID‑19, which suggested coinfection of these 2 diseases (Figure 1A and 1B). The patient was treated with trimethoprim / sulfamethoxazole, and both pathogens were sensitive to the agent. The clinical symptoms subsided and in follow‑up HRCT after 1 month of treatment, interstitial lesions were still present; however, they had less intensity (residual lesions were present in peripheral and central parts of the lung; Figure 1C and 1D). The patient was still experiencing weakness and dizziness during physical exercise at the time of publication; however, fever did not recur.
Fever is one of the most common symptoms of COVID‑19 which can also last for a long period. However, in immunocompromised patients such as kidney transplant recipients, other infections may have similar clinical presentation. A meta‑analysis by Raja et al4 demonstrated that secondary infection and coinfection in kidney transplant recipients are found to be rare and most of them are bacterial urinary tract infections. Nevertheless, infections caused by other opportunistic microorganisms, in particular cytomegalovirus, Aspergillus species, or Candida species are also possible. Underdiagnosis of these infections explains high overall mortality in solid organ transplant recipients (almost 20%).4 In such cases, pneumocystosis can even be lethal.5
Our patient had COVID‑19 followed by pneumocystosis, and the latter was diagnosed early enough to achieve cure. This underlines the need to evaluate HRCT thoroughly and consider coinfection with other life threatening pathogens.
- Jędrusik P, Gaciong Z, Sklinda K, et al. Diagnostic role of chest computed tomography in coronavirus disease 2019. Pol Arch Intern Med. 2020; 130: 520‑528. | Crossref
- Bai H, Hsieh B, Xiong Z, et al. Performance of radiologists in differentiating COVID‑19 from non‑COVID‑19 viral pneumonia at chest CT. Radiology. 2020; 296: E46‑E54. | Crossref
- Kanne JP, Yandow DR, Meyer CA. Pneumocystis jiroveci pneumonia: high‑resolution CT findings in patients with and without HIV infection. AJR Am J Roentgenol. 2012; 198: W555‑W561. | Crossref
- Raja MA, Mendoza MA, Villavicencio A, et al. COVID‑19 in solid organ transplant recipients: a systematic review and meta‑analysis of current literature. Transplant Rev (Orlando). 2021; 35: 100588. | Crossref
- De Francesco MA, Alberici F, Bossini N, et al. Pneumocystis jiroveci and SARS‑CoV‑2 co‑infection: a common feature in transplant recipients. Vaccines. 2020; 8: 544. | Crossref
ARTICLE INFORMATION