Serum levels of selected micronutrients in patients with inflammatory bowel disease in clinical remission
Key words: copper, inflammatory bowel disease, iron, selenium, zinc



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Serum levels of selected micronutrients in patients with inflammatory bowel disease in clinical remission
Introduction: Patients with inflammatory bowel disease (IBD) can experience micronutrient deficiency regardless of disease activity and extent.
Objectives: We aimed to evaluate serum concentrations of selected trace elements in adult patients with IBD in clinical remission with involvement limited to the colon who received immunosuppressive treatment.
Patients and methods: We enrolled 32 patients with IBD (mean [SD] age, 41 [15.2] years) and 30 healthy controls (mean [SD] age, 39.1 [11.8] years). Serum selenium, iron, copper, and zinc levels as well as complete blood count were measured in both groups.
Results: Patients with IBD had lower zinc concentrations than controls (mean [SD], 0.76 [0.13] mg/l vs 0.83 [0.13] mg/l; P = 0.047). No differences were observed for selenium (mean [SD], 0.90 [0.24] μmol/l vs 0.93 [0.19] μmol/l) and copper levels (mean [SD], 1.03 [0.27] mg/l vs 0.97 [0.22] mg/l). Compared with controls, patients with IBD had lower red blood cell count (mean [SD], 4.4 [0.6] 106/μl vs 4.7 [0.4] 106/μl; P = 0.03), hemoglobin (mean [SD], 12.7 [2.2] g/dl vs 14.3 [0.8] g/dl; P = 0.001), and iron levels (mean [SD], 14.2 [9.4] μmol/l vs 23.4 [2.7] μmol/l; P = 0.0001). Patients with IBD showed a positive correlation between selenium and iron (R = 0.499; P = 0.004) as well as selenium and hemoglobin levels (R = 0.579; P = 0.001).
Conclusions: Patients with IBD, despite maintaining clinical remission, should undergo systematic laboratory test for anemia or micronutrient deficiencies.
What's new?
Micronutrient deficiency affects the immune system and occurs in a significant proportion of patients with inflammatory bowel disease (IBD), even during remission. Deficiency of some trace elements may be associated with disease‑related morbidity, interfere with the achievement of deep remission, and cause exacerbations earlier during disease course. We evaluated the micronutrient status in patients with IBD in clinical remission with involvement of the colon alone and without malabsorption syndrome who received immunosuppressive treatment. The study showed lower zinc concentrations in patients with IBD compared with controls. We concluded that patients with IBD, despite maintaining clinical remission, should undergo systematic laboratory test for anemia or micronutrient deficiencies.
Introduction
Inflammatory bowel disease (IBD) is a group of chronic and relapsing diseases that affect the gastrointestinal tract, especially the intestines.1 While ulcerative colitis (UC) is restricted to the colon, Crohn disease (CD) may affect any portion of the gastrointestinal tract.2 The etiology of IBD is multifaceted. The disease may result from dysregulation of immune responses to the intestinal microbiota due to genetic predispositions.2,3 Patients with IBD experience relapses and remissions and present with bothersome symptoms such as abdominal pain, diarrhea, or rectal bleeding.4 The disease is incurable and the primary goal of therapy is to achieve clinical remission, followed by endoscopic remission. Current medical treatment involves the use of 5‑aminosalicylic acid, corticosteroids, immunomodulators, or biologic drugs.
Approximately 85% of patients with IBD present with signs of malnutrition.5 Malnutrition can be classified as macronutrient or micronutrient deficiency.6 The former is determined by protein–energy malnutrition and usually affects patients with active and severe disease.6 Patients with IBD in remission usually have normal macronutrient intake and thus show a lower incidence of macronutrient deficiency.7 However, patients with a mild course of IBD or those in remission may develop micronutrient deficiency, various types of which have been described.6-10 Malnutrition in IBD may be caused by restrictive diet, malabsorption, inflammatory process, or drugs used for treatment.11 Nutritional deficiencies are associated with prolonged hospitalization, a complicated perioperative course, and higher mortality rates.12,13 Micronutrient deficiency may influence the immune system and predispose an individual to the onset and progression of IBD.14
The micronutrients that are involved in inflammatory signaling pathways include selenium, zinc, iron, and copper.11 Selenium shows antioxidant activity and protects cells against the harmful effects of free radicals. It regulates growth processes and is a component of numerous essential enzymes.15 Zinc is a micronutrient that plays an important role in cellular metabolism, namely, it supports the catalytic activity of numerous enzymes, facilitates protein and DNA synthesis, modulates the immune function, and improves intestinal barrier function.16 Copper, on the other hand, is an essential cofactor for enzymes and electron transport proteins required for antioxidant, neurotransmitter, and histamine metabolism, oxidative phosphorylation, as well as iron transport.17 Iron deficiency, the most common systemic complication and extraintestinal manifestation in IBD, leads to a defective T‑cell proliferative response and impaired cytokine production by lymphocytes.18
Unfortunately, there is little evidence on the importance of micronutrients and their routine evaluation in patients with IBD.9 Previous studies on micronutrients in this population are limited by the inclusion of nonhomogeneous populations (patients with CD and UC), inclusion of patients with different extent and activity of the disease, and the use of different therapy regimens.
The aim of this study was to determine serum concentrations of selected trace elements, such as selenium, iron, copper, and zinc, in adult patients with IBD in clinical remission with the involvement limited to the colon who received immunosuppressive treatment, in comparison with healthy individuals, and to select micronutrients that could serve as potential sensitive markers of disease activity.
The exclusion criteria were as follows: pregnancy, malignancy, diabetes mellitus, obesity (body mass index ≥30 kg/m2), cardiovascular disease (hypertension, coronary artery disease, valvular heart disease, or cardiac arrhythmias), tobacco smoking, body mass index of less than 18.5 kg/m2, intake of medications potentially affecting serum iron, selenium, zinc, or copper concentrations and diet supplements containing the tested microelements, malabsorption syndromes (eg, celiac disease, short bowel syndrome), as well as total or partial parenteral nutrition.
Biochemical studies
Biochemical analyses, including complete blood count and the measurement of serum iron concentrations, were conducted at the Diagnostics Unit of the University Hospital in Kraków. Venous blood samples were obtained in a fasting state. The levels of iron and complete blood count (hemoglobin, mean corpuscular volume [MCV], white blood cells [WBCs], red blood cells [RBCs], platelets, and red blood cell distribution width [RDW]) were evaluated on the same day. For selenium, zinc, and copper assays, blood samples were centrifuged at 1000 g for 15 minutes at a temperature of 4 °C, and the serum was collected and stored at a temperature of –80 °C until further analysis.
Serum copper, zinc, and selenium concentrations were measured in the laboratory of the Department of Food Chemistry and Nutrition at Jagiellonian University Medical College. Serum levels of copper and zinc were determined with a PerkinElmer 5100 ZL atomic absorption spectrometer (PerkinElmer Inc, Norwalk, Connecticut, United States) using the flame technique. The calibration curves for copper and zinc were performed using 0.00-, 0.25-, 0.50-, 1.00-, 2.00-, and 3.00‑mg·l−1 standards. These solutions were prepared by diluting certified standard solutions (1000 mg·l−1, Merck, Darmstadt, Germany; copper catalog no., 1.19786.0500; and zinc catalog no., 1.19806.0500). Defrosted serum (0.5 ml) was mixed with 2 ml of demineralized water (Millipore RQ10, Vienna, Austria) and analyzed as described above. Each sample was measured 3 times. If the relative standard deviation of the 3 measurements exceeded 5%, then the measurement was repeated. The correctness of the results was checked with Seronorm (catalog no., 200805) and Pathonorm (catalog no., 100705) control serum (Sero, Billingstad, Norway). The parameters of the copper and zinc analysis were as follows: 1) for copper, wavelength was 324.8 nm; lamp current, 15 mA; slit width, 0.7 nm; air flow, 9 l·min−1; and acetylene, 2 l·min−1; and 2) for zinc, wavelength was 213.9 nm; lamp current, 18 mA; slit width, 0.7 nm; air flow, 10.8 l·min−1; and acetylene 2 l·min−1.
The selenium level was determined using an Agilent Technologies 240Z AA atomic absorption spectrometer (Agilent Technologies, Santa Clara, California, United States) with graphite furnace atomization and Zeeman background correction. The calibration curve was prepared using 3 serum standards containing 0.35, 0.61, and 1.77 µmol·l−1 selenium. The accuracy of the results was confirmed with Seronorm reference material (Trace Elements Serum L‑1, Sero). A hollow‑cathode lamp with enhanced light intensity (“ultra‑lamp”) was used as a light source, and high‑purity argon as an inert gas (99.998%).
Serum samples were mixed with 0.1% Triton solution (150 µl + 100 µl) to improve homogeneity. Owing to the presence of complex organic matrix in the samples, a chemical modifier was used and air‑assisted ashing was included in the temperature program of the graphite furnace. The samples were measured in duplicate unless the obtained precision was not satisfactory (in such cases, the measurement was repeated). The parameters of the analysis were as follows: wavelength, 196 nm; lamp current, 12 mA; slit, 1 nm; chemical modifier, 5% HNO3 containing 1500 mg·l−1 of palladium and 6000 mg·l−1 of Mg(NO3)2; air‑assisted ashing temperature, 400 °C; inert‑gas ashing temperature, 1150 °C; and atomization temperature, 2600 °C.
Ethical approval
The study protocol was approved by the Local Bioethics Committee at Jagiellonian University (decision no. KBET 122.6120.86.2015; as of May 24, 2015). All participants gave their written informed consent to be included in the study.
Statistical analysis
Descriptive statistics were calculated for all parameters in the IBD and control groups. The differences between groups were tested using the t test, the Welch test or the Mann–Whitney test, as appropriate. The Levene test was used to assess the equality of variances in the compared groups. The 2‑tailed Fisher test was used to assess the significance of the difference between 2 Pearson correlation coefficients. A probability level of P less than 0.05 was considered to be significant. The Pearson correlation coefficients were calculated for pairs of parameters. For parameters with non‑normal distribution Spearman correlation coefficients were calculated. The principal component analysis (PCA) model was used to further describe the correlation structure between parameters in the study group (using component weight analysis). The parameters with large weights (>0.3) in the PCA model were assumed to be correlated. To express the strength of bivariate associations, for the pairs of correlated parameters, the correlation weights were calculated. They are the algebraic products of corresponding weights of these 2 given parameters and cosine of the corresponding angle. The corresponding angle means the angle determined by 2 lines connecting the origin with coordinates of both parameters on the PCA weights plot. Statistical analyses were conducted using the STATISTICA, version 12 package (StatSoft, Tulsa, Oklahoma, United States), SIMCA‑P, version 9 package (Umetrics, Umeå, Sweden), IBM SPSS Statistics, version 27 and an online calculator (http://faculty.vassar.edu/lowry/rdiff.html) for the Fisher r-to-Z transformation. Finally, correlation weights for the pairs of parameters in the PCA were calculated using software delivered by MP System Co (Chrzanów, Poland).
Results
The comparison of analyzed parameters between the IBD and control groups is shown in Table 1. All but 3 patients in the IBD group had normal C‑reactive protein (CRP) values (<5 mg/l), with the maximum CRP level in this group being 7.66 mg/l (median, 1.95). None of the IBD patients had significantly elevated CRP. Patients with IBD had significantly lower RBC count, hemoglobin levels, and serum iron concentrations than controls. On the other hand, platelet count was significantly higher in patients with IBD. There was no difference in WBC count and MCV between groups. Serum zinc concentrations were lower in patients with IBD than in controls, but no significant differences were noted for selenium and copper levels.
Parameter | Patients with IBD | Controls | P valuea | ||
Mean (SD) | Median (min–max) | Mean (SD) | Median (min–max) | ||
a Parameters were compared using the t test, the Welch test, or Mann–Whitney test.
SI conversion factors: to convert RBC count to × 106/l, multiply by 1.0; WBC count to × 109/l, by 1.0; platelet count to × 109/l, by 1.0; Hb to g/l, by 10.0; Zn to μmol/l, by 15.29; and Cu to μmol/l, by 15.73.
Abbreviations: Cu, copper; Fe, iron; Hb, hemoglobin; IBD, inflammatory bowel disease; max, maximum; MCV, mean corpuscular volume; min, minimum; RBC, red blood cell; RDW‑CV, red blood cell distribution width; RDW‑SD, red blood cell distribution width, standard deviation; Se, selenium; WBC, white blood cell; Zn, zinc | |||||
Age, y | 41 (15.2) | 36 (23–75) | 39.1 (11.8) | 37 (21–69) | 0.62 |
RBC count, 106/μl | 4.4 (0.6) | 4.5 (2.7–5.5) | 4.7 (0.4) | 4.9 (3.9–5.4) | 0.04 |
WBC count, 103/μl | 7.4 (2.3) | 7.2 (3.8–13.5) | 7.3 (1.2) | 7.1 (5–9.9) | 0.79 |
Platelet count, 103/μl | 308.3 (92.9) | 300 (146–601) | 263.3 (56.) | 276 (195–345) | 0.03 |
Hb, g/dl | 12.7 (2.2) | 13.1 (7.1–16) | 14.3 (0.8) | 14.4 (12.4–15.5) | 0.001 |
Fe, µmol/l | 14.2 (9.4) | 14.5 (2.4–37.9) | 23.4 (2.7) | 23.1 (19.1–28.8) | <0.001 |
RDW‑CV, % | 14.6 (2.1) | 14 (12.6–19.8) | 13.6 (3.4) | 12.9 (12.1–31.5) | 0.001 |
RDW‑SD, fl | 45.4 (5.5) | 44.1 (40.1–64.4) | 40.8 (2.1) | 40.5 (36.8–46.2) | <0.001 |
MCV, fl | 86.2 (7.4) | 86 (65.5–98.7) | 84.8 (3.3) | 84 (79.9–91.3) | 0.37 |
Zn, mg/l | 0.76 (0.13) | 0.76 (0.5–1.1) | 0.83 (0.13) | 0.81 (0.61–1.12) | 0.047 |
Cu, mg/l | 1.03 (0.27) | 0.98 (0.57–1.62) | 0.97 (0.22) | 0.94 (0.64–1.62) | 0.32 |
Se, mmol/l | 0.9 (0.24) | 0.93 (0.36–1.43) | 0.93 (0.19) | 0.91 (0.64–1.4) | 0.5 |
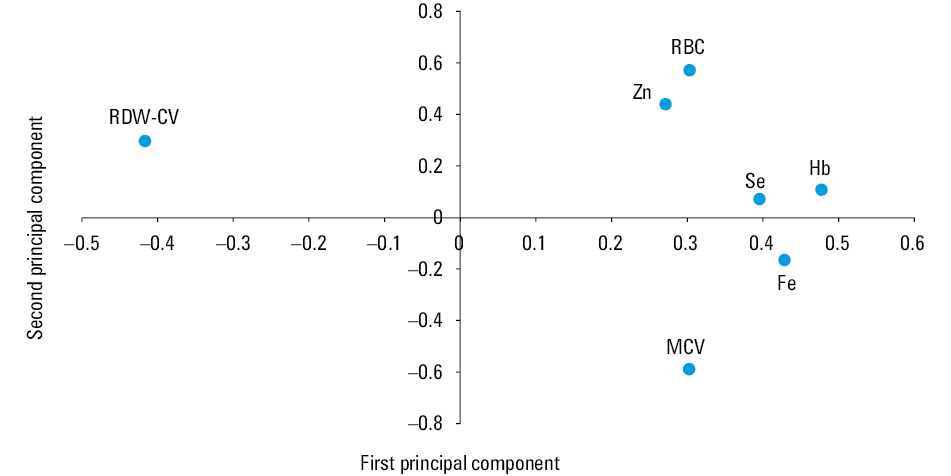
The PCA model, which fulfilled cross‑validation criteria, had 2 significant components with eigenvalues of 3.58 and 1.54, respectively. This model explained 73.2% of variance in the set of original parameters, reduced by 4 parameters that appeared to be uninformative (copper, platelets, RDW‑SD, WBC). In addition, 2 outlying patients were excluded from the model. The loadings for the first 2 principal components are shown in Figure 1. The first principal component in this model had positive loadings predominantly for hemoglobin, iron, and selenium. Therefore, the highest positive correlation weights based on this component were revealed between these parameters. Hemoglobin, iron, and selenium created the set of mutually correlated parameters. selenium and hemoglobin were strongly negatively correlated with RDW‑CV (Table 2). The second principal component was loaded mainly positively by mutually correlated RBC and zinc, and negatively, by MCV. Thus, MCV was negatively correlated with both RBC and zinc (Figure 1, Table 2). The PCA model confirmed some of the correlations revealed by the Pearson analysis (all in the cluster of parameters: hemoglobin, iron, selenium) as well as negative correlation between RDW‑CV and hemoglobin (Table 3, the Whole group column). Other negative correlations, presented in Table 2 were disclosed only by the by PCA.
Abbreviations: see Table 1
Pairs of correlated parameters | Correlation weights |
a Only correlation weights with absolute values higher than 0.1 are shown
Abbreviations: see Table 1 | |
RBC–Zn | 0.251 |
Hb–Se | 0.189 |
Hb–Fe | 0.17 |
Fe–Se | 0.145 |
RBC–RDW‑CV | –0.113 |
MCV–Zn | –0.134 |
RDW‑CV–Se | –0.149 |
Hb–RDW‑CV | –0.183 |
RBC–MCV | –0.192 |
Pairs of parameters | IBD | Controls | Whole group (IBD + controls) | |||
Correlation coefficient | P value | Correlation coefficient | P value | Correlation coefficient | P value | |
a There was a difference (P = 0.014) between Pearson correlation coefficients in these 2 groups (IBD and controls).
Abbreviations: see Table 1 | ||||||
RBC–Hba | r = 0.706 | <0.001 | r = 0.375 | 0.041 | r = 0.694 | 0.001 |
RDW‑CV–RDW‑SD | r = 0.69 | <0.001 | rS = 0.292 | 0.11 | rS = 0.604 | 0.001 |
Hb–Se | r = 0.579 | 0.001 | r = 0.26 | 0.17 | rS = 0.370 | 0.004 |
Fe–Se | r = 0.499 | 0.004 | r = –0.093 | 0.63 | r = 0.324 | 0.01 |
Hb–Fe | r = 0.452 | 0.01 | r = –0.066 | 0.73 | r = 0.539 | 0.001 |
Hb–Zn | r = 0.417 | 0.02 | r = 0.085 | 0.66 | r = 0.349 | 0.007 |
RBC–Zn | r = 0.413 | 0.02 | r = –0.088 | 0.65 | r = 0.298 | 0.02 |
Fe–MCV | r = 0.411 | 0.02 | r = 0.148 | 0.43 | r = 0.243 | 0.06 |
PLT–Fe | r = –0.372 | 0.047 | r = –0.25 | 0.18 | r = –0.47 | 0.001 |
RDW‑CV–Se | r = –0.378 | 0.04 | rS = 0.199 | 0.3 | rS = –0.027 | 0.84 |
RDW‑CV–MCV | r = –0.492 | 0.006 | rS = 0.241 | 0.2 | rS = –0.112 | 0.39 |
Fe–RDW‑CV | r = –0.521 | 0.003 | rS = –0.016 | 0.93 | rS = –0.462 | 0.001 |
Hb–RDW‑CV | r = –0.624 | <0.001 | rS = 0.029 | 0.88 | rS = –0.333 | 0.009 |
MCV–Se | r = 0.325 | 0.08 | r = 0.498 | 0.006 | r = 0.332 | 0.01 |
Discussion
Patients with IBD are at high risk for nutritional deficiencies because of long‑term inflammation in the gut mucosa and reduced oral intake. Chronic inflammation leads to the sequestration of some trace elements in the liver due to proinflammatory cytokine release induced by inflammatory response.11 This type of deficiency is typical at diagnosis in active disease generally due to impaired absorption but may also persist throughout the course of the disease due to reduced food intake, direct enteric loss of nutrients, or a hypercatabolic state in this population.11 Chronic diarrhea and fistula output can lead to zinc, calcium, and potassium wasting,19 while iron deficiency is the most common nutritional deficiency in colitis due to chronic gastrointestinal bleeding.20 Malabsorption most commonly occurs in CD with active small bowel disease or small bowel resection. Moreover, numerous medications used for IBD, such as glucocorticoids, can affect normal micronutrient absorption.
Micronutrient deficiencies occur in more than half of patients diagnosed with IBD.5 Some authors showed that systemic inflammatory response reduces serum levels of micronutrients including zinc, selenium, and copper as well as vitamins A, B6, C, and D, which may occur irrespective of the actual nutritional status.21,22 On the one hand, these deficiencies result from serious disease, but on the other hand, they also cause morbidity12,13,23 and are associated with a high risk of poor outcome. Thus, trace elements seem to be an important subject of research on the prevention and control of IBD. Unfortunately, little attention is paid to nutritional support and estimation of micronutrient content in these patients. Moreover, most previous studies on micronutrient deficiency in IBD were performed in patients with active disease with different disease locations and therapy regimens. To our knowledge, this study is the first to assess micronutrient status in IBD patients during disease remission, with involvement limited to the large intestine, and receiving the same treatment with mesalazine and azathioprine.
Selenium and zinc are important trace elements with various functions that influence the immune system. Dietary zinc and selenium deficiency was shown to worsen experimental colitis by affecting various signaling pathways involved in inflammation and oxidative stress, as well as by affecting the intestinal microbiota.11,24 Zinc reduces the number of proinflammatory cells and production of proinflammatory cytokines.5,25 Furthermore, it was shown to reduce the activity of inducible nitric oxide synthase in activated macrophages, thus protecting against the production of reactive oxygen and nitrogen species and cellular damage.26 Zinc intake is also believed to reduce the risk of CD and UC.27 As shown by previous studies, zinc deficiency is common in patients with IBD, with a prevalence ranging from 15% to 40%.28,29 Our study also demonstrated decreased serum zinc concentrations despite clinical remission and absence of evident malabsorption. This result is in line with the findings reported by MacMaster et al,10 who identified several biochemical micronutrient deficiencies, including that of zinc, among patients with IBD in remission.
Zinc is absorbed in the small intestine, which explains its deficiency in patients with chronic diarrhea or malabsorptive disorders. It is noteworthy that this deficiency is not only a consequence of poor zinc intake but is also related to an inflammatory process in IBD. This is supported by the finding that zinc deficiency is common even among patients with IBD who have received sufficient oral supplementation.30 In our patients, malabsorption syndrome was not observed and the small intestine was not affected by the disease. However, the limitation of this study is the fact that we did not confirm endoscopic remission and did not evaluate the concentration of calprotectin in the stool in our patients. It is possible that reduced zinc concentrations are caused by persistent colonic inflammation.
There is compelling evidence that chronic inflammation in the intestine is related to oxidative and nitrosative stress both in patients with UC and those with CD.31 The impact of prooxidative status is further reinforced by a reduced antioxidant level (which is also commonly observed during remission), suggesting that oxidative stress plays an important role in disease recurrence.31 Zinc functions as an antioxidant.32 It is possible that its reduced levels may be secondary to enhanced production of a zinc‑containing enzyme with antioxidant activity. Research revealed lower activity of copper–zinc superoxide dismutase in patients with IBD, which explains the reduced ability to scavenge free radicals in these patients. This reduction may be partly due to zinc deficiency and an impaired antioxidant system.26
Zinc is an important component for the synthesis of proteins and erythrocytes.15 This is in line with our observations on the positive correlation between RBC count and zinc concentrations.
Siva et al33 showed that serum zinc deficiency is correlated with disease‑related morbidity, as reflected by increased rates of hospitalizations, surgery interventions, and disease‑related complications in patients with CD compared with individuals with normal zinc concentration.33
Ananthakrishnan et al27 suggested that normal zinc concentrations may contribute to longer remission periods. Therefore, it might be hypothesized that lower zinc levels in patients during remission might predict early exacerbation. This is supported by the study by MacMaster et al,10 who reported a strong relationship between zinc deficiency and time to next relapse, especially in patients with CD. It appears that decreased zinc concentrations could be a sensitive marker for disease activity in patients with subclinical mucosal inflammation.
Selenium is an important micronutrient associated with numerous selenoproteins with important functions. The absorption of selenium has been generally poorly researched, although the highest absorption has been reported in the ileum, followed by the jejunum and large intestine.8
An epidemiological study suggested that selenium status is negatively correlated with IBD activity and colon cancer risk.34 The mechanism behind this correlation has not been elucidated, but it may be hypothesized that the effect is due to the ability of selenium to polarize macrophages from an M1- to M2‑like phenotype, hence reducing inflammation and accelerating healing of the epithelium.35
Some studies reported reduced selenium concentrations in patients with IBD as compared with controls, regardless of disease activity and location36-39; however, the exact prevalence is unknown. Selenium deficiency was revealed in patients with IBD even during remission, and reduced selenium concentrations were shown to be associated with increased disease severity.40,41 Regarding the extent of the disease, Castro Aguilar‑Tablada et al41 reported significantly higher serum selenium concentrations in patients with proctosigmoiditis than in those with ileal or colonic involvement and significantly lower concentrations in patients with an inflammatory form of IBD as compared with those with a chronic intermittent or chronic continuous form. They also reported a possible relationship between corticosteroid treatment and a reduction of serum selenium levels.41 In addition, Han et al6 reported that corticosteroid use and inflammation may predispose to selenium deficiency. In such a case, selenium deficiency may result from insufficient supply, decreased absorption, or increased mobilization for antioxidant defense.39
In contrast to the above studies, Sikora et al42 and Stochel‑Gaudyn et al43 did not find any significant differences in selenium concentrations between patients with IBD and the control group. Moreover, Sikora et al42 reported significantly lower serum iron and zinc levels in children with IBD compared with controls. These results are in line with our observations. We reported no significant differences for selenium levels between the study groups; however, patients with IBD had a significantly lower RBC count, hemoglobin level, and serum iron concentrations than controls. Moreover, selenium concentrations correlated positively with hemoglobin and iron levels. This is in line with the study by Castro Aguilar‑Tablada et al,41 who reported a positive correlation between serum selenium levels and biochemical parameters related to the iron status.41
Relatively high selenium levels in IBD patients in our study can be explained by the fact that the disease did not involve the small intestine, which is the main site of absorption. Whether selenium deficiency is the cause or effect of IBD remains the subject of debate. The selenium level comparable between healthy individuals and patients with IBD in remission would rather suggest that the selenium concentrations is affected by inflammatory process and not the other way round. Copper is a trace element involved in biological transport of electrons and oxygen. Its deficiency is rather rare owing to large stores in the liver, muscles, and bones.8 Various studies reported discrepant results regarding serum copper concentrations in patients with IBD as compared with healthy controls.26,39,44 These differences may be partly due to different degrees of disease severity. Filippi et al7 showed decreased serum copper levels in patients with CD in remission compared with controls. However, this finding was not corroborated by other studies.38,45 As for patients with UC, some studies reported similar copper levels to controls, while others revealed elevated levels.38,46 In a study by Stochel‑Gaudyn et al,43 the mean serum copper concentration was significantly higher in IBD patients at diagnosis than in healthy controls. Mohammadi et al26 reported that copper concentrations did not differ between patients with IBD and controls. This result is in line with our study.
Among micronutrients, zinc and copper have an essential function in inflammation, with an increased copper‑to‑zinc ratio in chronic inflammation and free radical overproduction.44 Systemic inflammation has the opposite effect on serum zinc and copper concentrations, resulting in an increased copper‑to‑zinc ratio.47 In contrast to zinc, copper concentrations increase during the acute‑phase response.48 A higher copper‑to‑zinc ratio has been described in patients with active colitis with elevated copper and diminished zinc levels in the serum of patients with IBD compared with healthy controls.45 These results are in line with our findings. Despite remission, the copper‑to‑zinc ratio in our patients seemed to be increased because zinc concentrations were reduced and copper levels were slightly (although nonsignificantly) increased as compared with controls. This supports the finding of Mohammadi et al26 that the ratio of copper to zinc is clinically more important than the concentration of either element alone.26 Therefore, an increased ratio may be also a potential marker of inflammatory process in clinical remission in patients with IBD. However, this observation, reported previously by Malavolta et al,44 has to be confirmed in future studies assessing correlations of the copper‑to‑zinc ratio with endoscopic and histologic disease markers.
Multiple factors in IBD contribute to iron deficiency: intestinal blood loss, reduced dietary iron intake, duodenal disease involvement, or surgical resection of the duodenum leading to diminished iron absorption.20 Iron deficiency is linked to disease activity.20 Inflammatory cytokines increase the production of liver hepcidin, which blocks ferroportin‑1 and prevents iron release from enterocytes, macrophages, and hepatocytes.49 As shown by previous studies, iron deficiency is common in patients with IBD.42,43 Our study also reported decreased serum iron concentrations despite clinical remission and absence of evident malabsorption. Because the concentrations of some micronutrients, including iron concentration, may change as a result of proton pump inhibitors use,50 none of the patients enrolled in this study took these drugs long term.
In conclusion, if we looked at patients in clinical remission only, some of nutritional deficiencies persisted. Undoubtedly, a drawback of the study is a small study group and an relatively large variety of disease locations and extent, although we tried to minimize these differences by eliminating those with rectal involvement only. Patients with IBD, despite maintaining clinical remission, should undergo systematic laboratory tests for anemia or micronutrient deficiencies. Correction of these deficiencies, which impair the immune response, could facilitate achievement of long and deep remission. This is consistent with the European Society for Clinical Nutrition and Metabolism guidelines published in 2017, which recommend that micronutrients should be assessed in patients in clinical remission to guide the decision on supplementation but also alert to the fact that inflammatory process may influence the results. Further research is needed to confirm whether zinc levels could serve as a predictor of the course of IBD or as a therapeutic target to maintain disease remission.
- Barnett M, Bermingham E, McNabb W, et al. Investigating micronutrients and epigenetic mechanisms in relation to inflammatory bowel disease. Mutat Res. 2010; 690: 71‑80. | Crossref
- Abraham C, Cho JH. Inflammatory bowel disease. N Engl J Med. 2009; 361: 2066‑2078. | Crossref
- Zhang YZ, Li YY. Inflammatory bowel disease: pathogenesis. World J Gastroenterol. 2014; 20: 91‑99. | Crossref
- De Lange KM, Barrett JC. Understanding inflammatory bowel disease via immunogenetics. J Autoimmun. 2015: 64: 91‑100. | Crossref
- Weisshof R, Chermesh I. Micronutrient deficiencies in inflammatory bowel disease. Curr Opin Clin Nutr Metab Care. 2015; 18: 576‑581. | Crossref
ARTICLE INFORMATION