Secondary arterial hypertension (AH) affects 5% to 15% of the general hypertensive population.1 Because it is not common, patients are seldom screened for its presence. Screening is recommended when AH begins in young age, is resistant to pharmacotherapy, or when hypertensive organ damages can be found.1,2 Coarctation of the aorta (CoAo) is responsible for 1% of cases of secondary AH; it is also the most frequent reason for AH in children.1
A 42‑year‑old man was admitted to the Department of Cardiology at John Paul II Hospital in Kraków, Poland due to extremely high values of arterial pressure. Despite polypharmacotherapy his blood pressure was over 190/110 mm Hg. He had been treated for AH for 10 years and had been operated on in 2011 modo Bentall de Bono due to bicuspid aortic valve insufficiency and ascending aortic aneurysm. His concomitant diseases included left kidney agenesis and tooth decay.
Physical examination revealed the following abnormalities: elevated blood pressure with a significant difference (>20 mm Hg) between the upper and lower limbs, systolic murmur along the left edge of the sternum radiating to the interscapular region, and clicking of the artificial aortic valve. Transthoracic echocardiography showed CoAo with a transisthmic pressure gradient of 72/32 mm Hg, prolonged diastolic phase, and flattened flow in the abdominal aorta. The artificial aortic valve worked properly and no additional structures on the valve were visible; however, a large hypoechogenic structure attached to the ascending aortic prosthesis was revealed. Computed tomography (CT) angiography (Sonata Maestro Class, Siemens, Erlangen, Germany) confirmed CoAo with a minimum aortic diameter of 7 mm and coexisting expansion of collateral vessels. It also revealed pseudoaneurysm of the ascending aorta with involvement of the left coronary artery (Figure 1A). Of note, CoAo was not diagnosed before the first cardiac surgery.
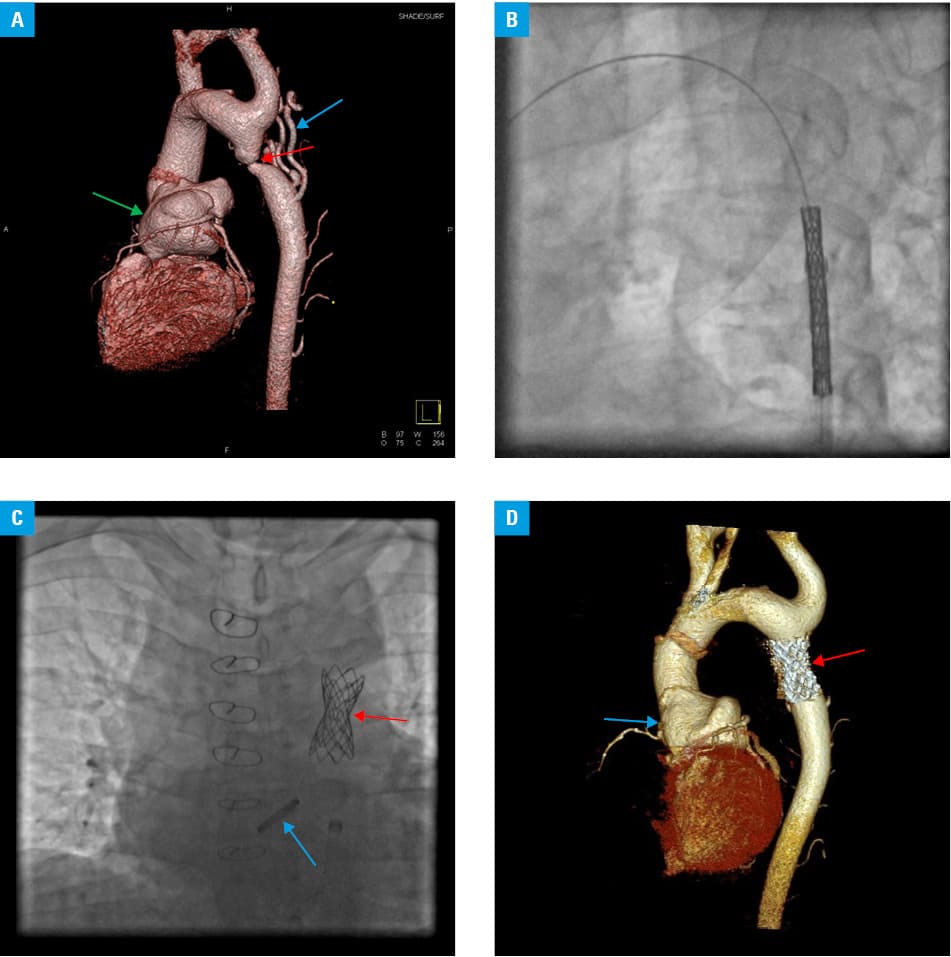
Pseudoaneurysms can be dangerous due to their increase in size as well as the possibility of rupture and active bleeding. The patient was referred for a hybrid procedure. The first stage involved percutaneous aortic angioplasty with stent implantation which caused a decrease in the aortic pressure gradient to 10 mm Hg (Figure 1B and 1C). Cardiac surgery exposed infectious lesions of the aorta and artificial aortic prosthesis, requiring a replacement of the valve and aortic graft. The aortic pseudoaneurysm could not be removed due to adhesions; it was only possible to close its gates and release the left coronary artery. Subsequently, standard pharmacological treatment of infectious endocarditis was started.
Six months later the patient was in functional New York Heart Association class I, with sufficient blood pressure control on pharmacotherapy. Echocardiography and CT revealed no dysfunction of the mechanical aortic prosthesis and size reduction of the aortic pseudoaneurysm (Figure 1D).
Our patient presented typical comorbidities of CoAo, namely, bicuspid aortic valve, ascending aortic aneurysm, and arterial hypertension. It is very important to be aware of these comorbidities during examination and echocardiography of any patient with arterial hypertension as their early recognition can prevent complications and ensure the initiation of timely and appropriate treatment. Despite elimination of the secondary cause, blood pressure does not always return to normal values. Such residual hypertension indicates that irreversible vascular remodeling has taken place. Thus, in patients with potentially reversible causes of hypertension, early detection and treatment are important to prevent changes in the vasculature and target organs.2
- Williams B, Mancia G, Spiering W, et al. 2018 Practice Guidelines for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. Blood Press. 2018; 27: 314‑340. | Crossref
- Rimoldi SF, Scherrer U, Messerli FH. Secondary arterial hypertension: when, who, and how to screen? Eur Heart J. 2014; 35: 1245‑1254. | Crossref
ARTICLE INFORMATION