A rare endoscopic image of Boerhaave syndrome in a patient treated with pleural effusion drainage



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
A rare endoscopic image of Boerhaave syndrome in a patient treated with pleural effusion drainage
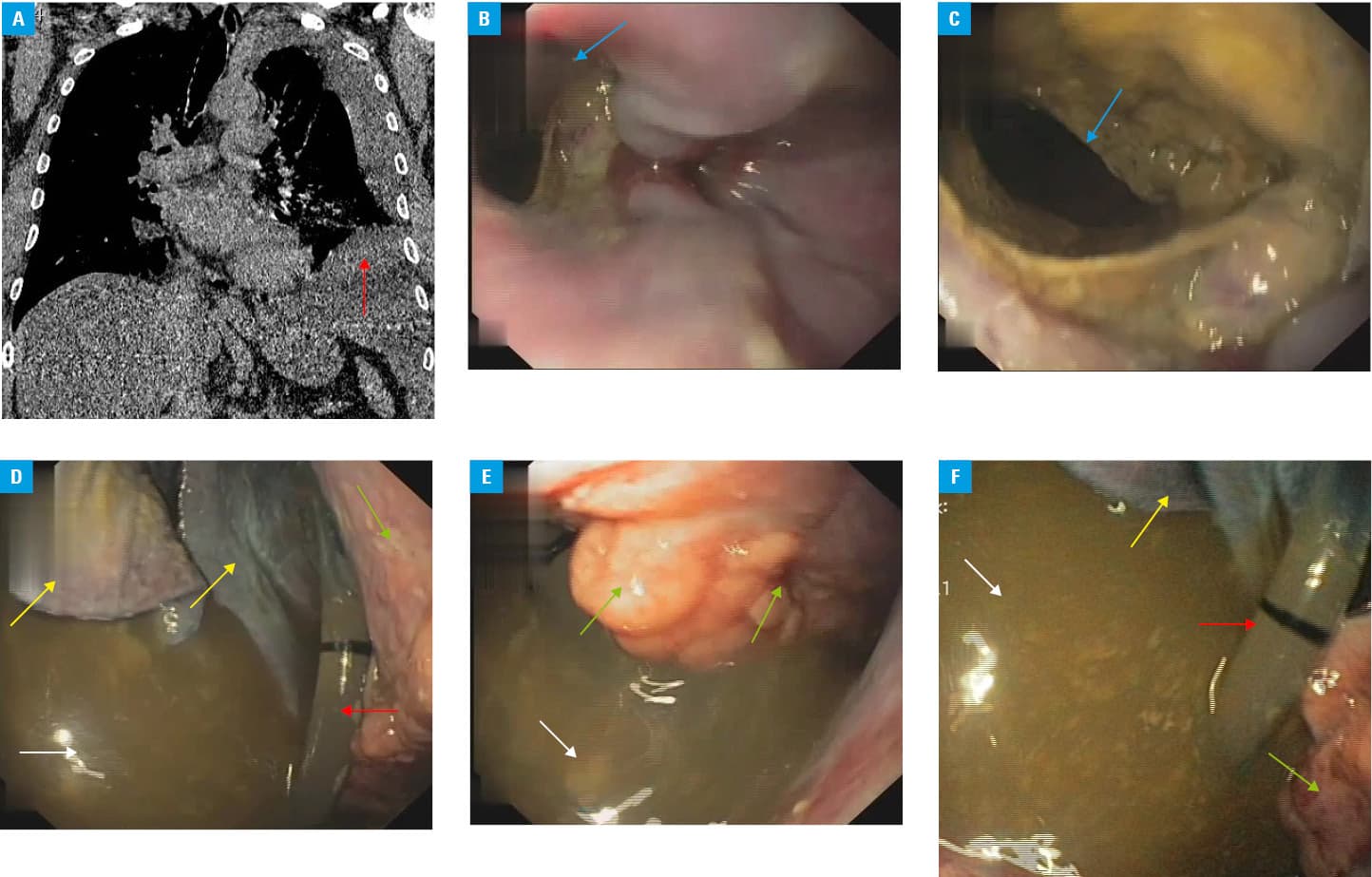
A 48‑year‑old man was admitted to our department because of thoracic injury following a car accident. Initially, the patient complained of dyspnea and chest pain. Imaging examinations (Figure 1A) performed on admission revealed 4 fractured ribs (VII–X) in the midclavicular line and left‑sided pleural effusion. The left pleural cavity was subsequently drained of 200 ml of cloudy fluid. On the first day of hospitalization, the patient experienced nausea and severe vomiting as well as deterioration of general condition. He was referred for endoscopic examination of the upper gastrointestinal tract to diagnose the abovementioned symptoms. Gastroscopy (Figure 1B–1F) was performed, which revealed a large perforation in the esophageal wall. Through the perforation, the gastroscope was introduced into the chest, visualizing the mediastinal structures, fluid with food fragments, and the pleural drain (Figure 1B–1F). The fluid and food fragments were removed from the left pleural cavity during the procedure; however, attempts to repair the esophageal perforation failed, and the patient was referred for surgical management of Boerhaave syndrome. On the second day after the accident, suturing of the esophageal perforation via the thoracic access with drainage of the pleural cavity was successfully performed. The patient was discharged after 6 days of hospitalization in good general condition.
Boerhaave syndrome is a pressure‑induced rupture of the esophageal wall and is associated with high morbidity and mortality.1,2
Despite reports of successful endoscopic management of esophageal rupture,3,4 surgery is the first‑line treatment for Boerhaave syndrome, especially in stable, young patients without severe comorbidities.1,2
Due to the rapid development and severe clinical course of Boerhaave syndrome (it is often accompanied by sepsis caused by mediastinitis), an endoscopic view such as the one described here is very rarely obtained during gastroscopy. In the presented case no symptoms suggesting Boerhaave syndrome were noticed prior to gastroscopy. In our opinion, dyspnea on admission was due to fluid in the left pleural cavity, while chest pain resulted from fractured ribs following the car accident. In our patient, slight perforation of the esophagus occurred during thoracic trauma. Severe vomiting caused by the esophageal perforation led to full‑thickness tear of the esophageal wall and Boerhaave syndrome.
- Whyte RI. Boerhaave’s syndrome. N Engl J Med. 2001; 344: 138‑139. | Crossref
- Carrott PW Jr, Low DE. Advances in the management of esophageal perforation. Thorac Surg Clin. 2011; 21: 541. | Crossref
- Schweigert M, Beattie R, Solymosi N et al. Endoscopic stent insertion versus primary operative management for spontaneous rupture of the esophagus (Boerhaave syndrome): an international study comparing the outcome. Am Surg. 2013; 79: 634‑640. | Crossref
- Patel SK, Ali Shera I, Raj V. Do esophageal stents have a role in Boerhaave syndrome? Case reports. Indian J Thorac Cardiovasc Surg. 2018; 34: 78‑80. | Crossref
ARTICLE INFORMATION