Transformation of gastric mucosa-associated lymphoid tissue lymphoma into diffuse large B‑cell lymphoma with cardiac infiltration resistant to immunochemotherapy



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Transformation of gastric mucosa-associated lymphoid tissue lymphoma into diffuse large B‑cell lymphoma with cardiac infiltration resistant to immunochemotherapy
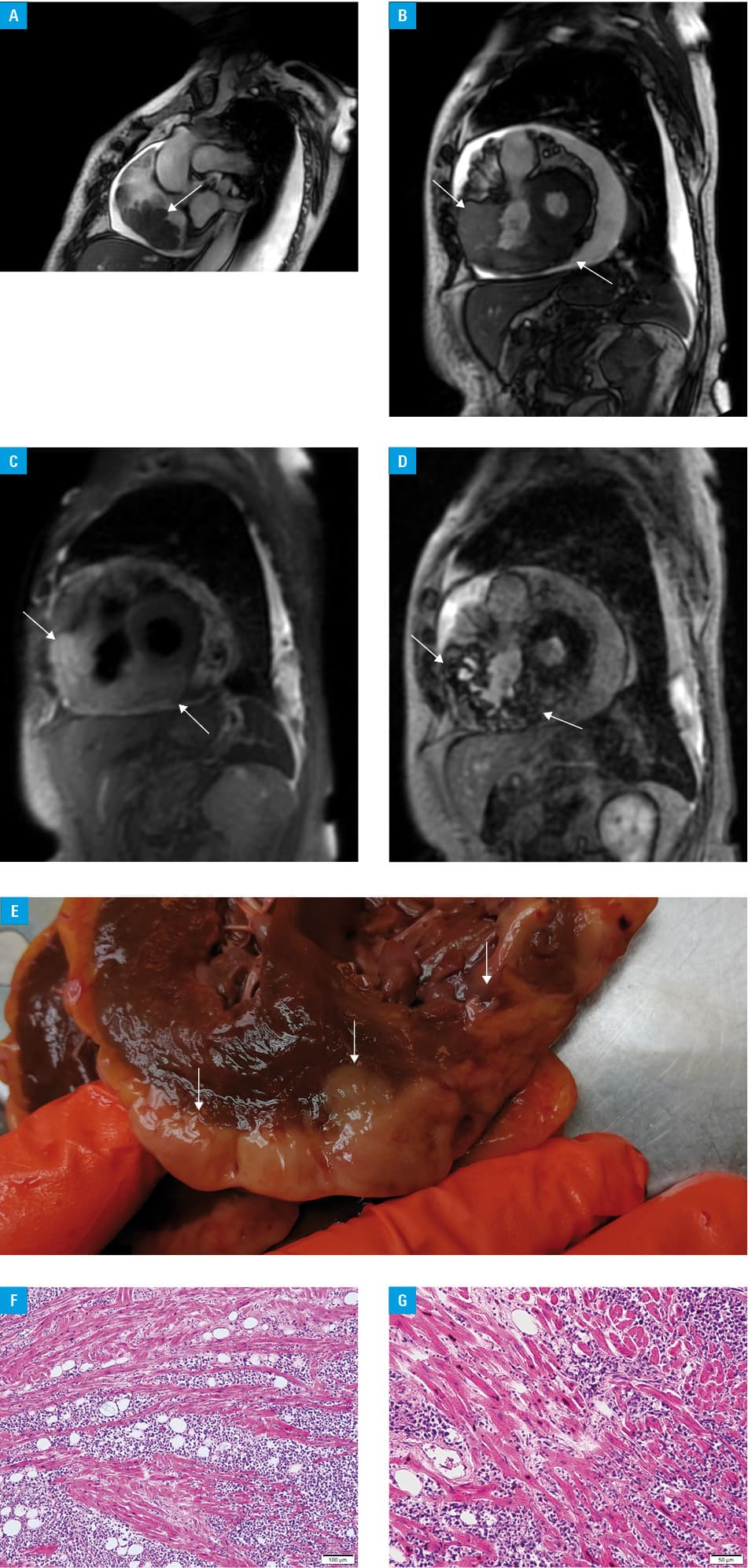
A 76‑year‑old woman was diagnosed in 2018 with gastric mucosa‑associated lymphoid tissue (MALT) lymphoma with plasmacytic differentiation and the following results of immunohistochemical analysis: CD38+, CD138–/+, CD79a+, CD20+, LCA+, Ki67 labeling index of 10%, CD56–, Kappa–/Lambda+++, cyclin‑D1–, as well as no lymphadenopathy on whole‑body computed tomography (CT) (Ann Arbor stage I). Helicobacter pylori eradication therapy was applied. Follow‑up gastroscopy showed only chronic gastritis. In 2019, the patient was referred with right cervical lymphadenopathy and enlargement of the right tonsil. Whole‑body CT revealed infiltration of the right maxillary sinus and bilateral cervical lymphadenopathy (Ann Arbor stage IV). Lymph node biopsy followed by fluorescence‑activated cell sorting showed clonal B‑cell CD19+, dominant phenotype CD20+++, CD200+++, CD79b+, CD22+, FMC‑7+, CD11c+dim, CD25+, CD10–, CD5, CD103–, CD123–, CD43–, Kappa–/Lambda+. The diagnosis of diffuse large B‑cell lymphoma (DLBCL) was confirmed by pathological examination. Rituximab‑bendamustine immunochemotherapy was started with a prompt regression of lymphadenopathy. The patient received a total of 6 cycles. Due to progression, after control echocardiography, immunochemotherapy was continued with the R‑CHOP regimen (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisolone). However, only one course was given due to toxicity (hemolytic anemia). Whole‑body contrast CT revealed an uneven contrast distribution in the lumen of the right atrium (RA) and the right ventricle, as well as pleural and pericardial effusion. Echocardiography showed normal left ventricular ejection fraction and a 2 to 3 cm tumor in the RA, impeding the flow through the tricuspid valve. Cardiac magnetic resonance imaging presented distinctive features of primary heart lymphoma—irregular tumor, 57 × 31 mm at the lower wall of the RA infiltrating the tricuspid valve leaflets, the lower and anterior walls of the right ventricle, and the lower wall of the left ventricle. The infiltration showed homogeneously low signal intensity in T1‑weighted images, increased signal intensity in T2‑weighted images and heterogenous late‑phase contrast enhancement. A significant amount of fluid in the pericardium suggested epicardial involvement (Figure 1A–1D). The patient was unsuitable for cardiac surgery and died of multiple organ failure. Autopsy confirmed heart infiltration by DLBCL (Figure 1E–1G).
Gastric MALT lymphoma is a subtype of the marginal zone lymphoma associated with H. pylori infection; therefore, treatment is directed toward eradication of this pathogen. MALT lymphoma rarely transforms into DLBCL.1 In general, DLBCL infrequently involves the heart, with a predilection to the right heart wall (especially the RA), with infiltration of the pericardium and the epicardium, and clinical symptoms of heart failure.2,3 Cardiac involvement is usually diagnosed late and has a poor prognosis.2,3 Moreover, the transformation of MALT lymphoma may be associated with primary resistance to immunochemotherapy.4
The presented case shows cardiac involvement probably after transformation of MALT lymphoma to DLBCL with resistance to the standard immunochemotherapy. A short period of time (8 months) between diagnoses suggests transformation rather than the coexistence of lymphomas.5 Rapid deterioration of patient’s clinical condition precluded further therapy. We suggest that cardiac echocardiography should be performed more frequently during the treatment and follow‑up in patients with transformation to DLBCL. In addition to monitoring cardiac toxicity, it may facilitate early diagnosis of clinically asymptomatic cardiac infiltration and modification of the treatment.
- Fujita A, Tajika M, Tanaka T, et al. A case of API2‑MALT1‑positive gastric MALT lymphoma with concomitant diffuse large B‑cell lymphoma. Nagoya J Med Sci. 2017; 79: 251‑257.
- Kaiafa G, Bobos M, Savopoulos C, et al. Heart and lymphoma: an unusual case of secondary cardiac lymphoma manifested through presyncope and syncope episodes and atrial flutter. Hellenic J Cardiol. 2018; 59: 182‑185. | Crossref
- Yousif P, Kotecha A, Thakur A, et al. A rare case of diffuse large B cell lymphoma presenting as a cardiac mass. Am J Case Rep. 2019; 20: 1821‑1825. | Crossref
- Zhou H, Yang L, Dang Q, et al. Ibrutinib resistance in a patient with transformed diffuse large B‑cell lymphoma from primary pulmonary mucosa‑associated lymphoid tissue lymphoma. Cancer Biol Ther. 2020; 21: 303‑308. | Crossref
- Kiesewetter B, Lamm W, Dolak W, et al. Transformed mucosa‑associated lymphoid tissue lymphomas: a single institution retrospective study including polymerase chain reaction‑based clonality analysis. Br J Haematol. 2019; 186: 448‑459. | Crossref
ARTICLE INFORMATION