Introduction
Myocarditis is an inflammatory heart disease induced by both infectious (ie, viral, bacterial, fungal) and noninfectious (ie, immune‑mediated organ‑specific or systemic disease, drugs, toxins) causes.1 It mainly affects young adults and children, leading to increased cardiac morbidity and mortality. Myocarditis is usually considered an uncommon disease, though its real incidence seems to be largely underestimated. Postmortem studies on sudden cardiac death (SCD) in young people revealed active myocarditis in 2% to 42% cases.2,3 Moreover, in the years 1990 to 2015, increased morbidity and mortality from myocarditis were recorded.4 In approximately 50% of patients, acute myocarditis resolves itself spontaneously, while in the remaining cases, it evolves into serious complications and / or to dilated cardiomyopathy (DCM). Finally, due to the variability of clinical presentation and its unpredictable prognosis, myocarditis still poses many diagnostic and therapeutic challenges.
In this review, we would like to summarize current knowledge about myocarditis and inflammatory cardiomyopathy, trying to outline some practical diagnostic algorithms, and to focus on more recent endomyocardial biopsy (EMB)-based therapeutic approaches. We will also highlight the importance of a close follow‑up of patients with clinically suspected or EMB‑proven myocarditis.
Definition
The diagnosis of myocarditis is only established following histological, immunohistochemical, and molecular confirmation based on EMB (Table 1).1 Inflammatory cardiomyopathy is defined as myocarditis with systolic or diastolic cardiac dysfunction.1 Autoimmune myocarditis can be defined as an EMB‑confirmed myocardial inflammation in the absence of a virus or other infectious agents, with or without serum antiheart autoantibodies (AHA).
a Recommended viral screen: enterovirus, influenza virus, adenovirus, cytomegalovirus, Epstein‑Barr virus, parvovirus B19, human herpes virus 6
Abbreviations: AHA, antiheart autoantibody; CD, cluster differentiation; PCR, polymerase chain reaction | |
Histological definition (Dallas criteria) | |
„Inflammatory infiltrates within the myocardium associated with myocyte degeneration and necrosis of non‑ischaemic origin”1 | |
Immunohistochemical criteria (abnormal inflammatory infiltrate) | |
| |
Etiology and immunological criteria | |
Virus‑positive myocarditis |
|
Autoimmune |
|
Immune‑mediated |
|
Virus‑triggered |
|
Etiology
Myocarditis can be the result of multiple causes, viral infection being the leading one (Table 2).1 A viral genome is found in myocardial tissue in about 15% to 30% of patients with active myocarditis,5,6 more frequently in early disease; in 30% of cases, multiple viral agents, mainly parvovirus B19 and herpes virus 6, can be detected.7
Infectious myocarditis | Noninfectious myocarditis | ||||
Immune‑mediated myocarditis | Toxic myocarditis | ||||
RNA viruses |
| Autoimmune |
| Drugs |
|
DNA viruses |
| Allergens / hypersensitive |
| Toxins |
|
Bacteria |
| Alloantigens | Heart transplant rejection | Physical pathogens |
|
Fungi |
| Heavy metals |
| ||
Parasites and protozoa |
| Miscellaneous |
| ||
Rickettsia |
| ||||
Autoimmune myocarditis may occur with exclusive cardiac involvement or in the context of systemic immune diseases (SIDs), such as hypereosinophilic syndromes, sarcoidosis, and connectivitis.8-10 In immune‑mediated myocarditis, specific AHA are directed against cardiac or neoantigens.1,9 Recently, a novel group of anticancer agents, immune checkpoint inhibitors, displayed the potential to induce auto‑immune myocarditis with serious complications.11
Pathogenesis
Genetic predisposition (in both human leukocyte antigen–related and unrelated forms) may play a role in the pathogenesis of myocarditis and its progression to postinflammatory cardiomyopathy (Figure 1).1,12,13
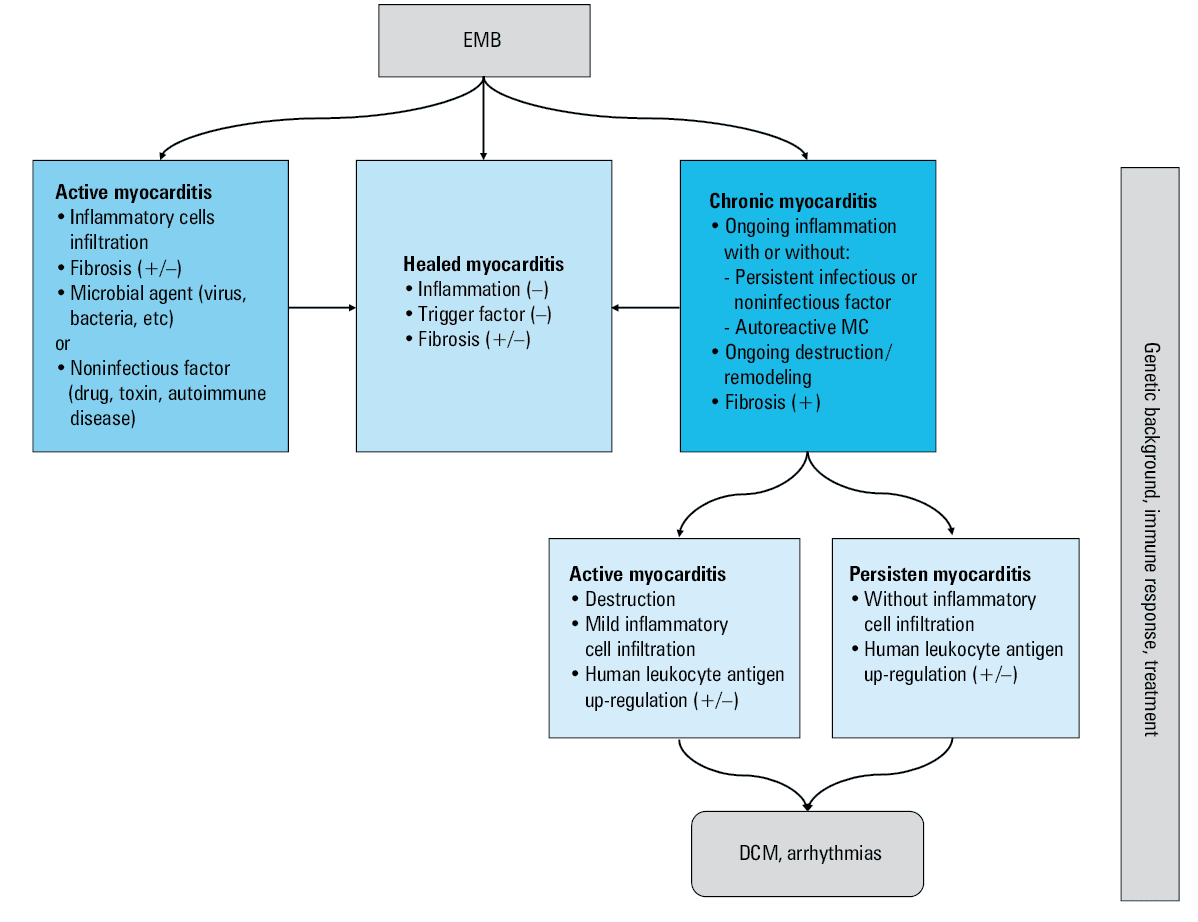
Regardless of its etiology, myocardial injury initiates an inflammatory cascade that, based on experimental animal models, evolves into 3 phases.
Phase I (acute myocarditis)
A specific infectious or noninfectious cause alters the myocyte membrane and triggers an immune response, ranging from transient / mild to fulminant / severe, which consists of predominant macrophage and lymphocyte infiltration of myocardial tissue. This may be associated with an increased production of immune mediators and cytokines leading to inflammatory changes (edema, hyperemia, necrosis with or without fibrosis) in myocardial tissue.
Phase II (healed or chronic myocarditis)
In most patients, after viral infection, the host immune response clears the pathogen and the inflammation is resolved. However, a substantial group of patients with altered immune reactivity develop a heart‑specific autoimmune reaction leading to acute and / or chronic myocardial inflammation.14,15
Phase III (immune‑mediated myocarditis)
The chronic phase may cause progressive myocyte loss, followed by collagen deposition (fibrosis), with or without residual inflammation. In turn, fibrosis progressively disturbs the myocardial architecture leading to tissue remodeling, loss of contractile function, and eventually to DCM. Further complications are linked to valvular dysfunction and arrhythmias due to the involvement of the conduction system, fibrosis‑related reentry phenomena, and stimulation of the myocardial adrenergic receptor by autoantibodies.16
Effector cells involved in adaptive immune response in phases II and III are mainly clusters of differentiation 4 (CD4) (helper T cell), CD8 T lymphocytes (cytotoxic T cells), and B lymphocytes.
Following cardiotropic viral infections, molecular mimicry and cross‑reactivity phenomena may contribute to the development of autoantibodies against myocardial tissue.17
Clinical features and diagnostic evaluation
Clinical manifestations of myocarditis may include ischemic‑like presentation, recent‑onset heart failure (HF) and, less frequently, cardiogenic shock and severe arrhythmic pictures.18 These clinical pictures differ in terms of clinical severity and prognosis. Sometimes, the onset of myocarditis is briefly preceded by a respiratory or gastrointestinal infection.1
Due to the variability of its clinical presentation, the diagnosis of myocarditis is sometimes challenging. Thus, a uniform approach to the diagnostic process is recommended (Figure 2).1 Diagnosis of clinically suspected myocarditis is based on the clinical picture and deviations in additional tests (Table 2).1 The more criteria are fulfilled, the higher the likelihood of myocarditis.
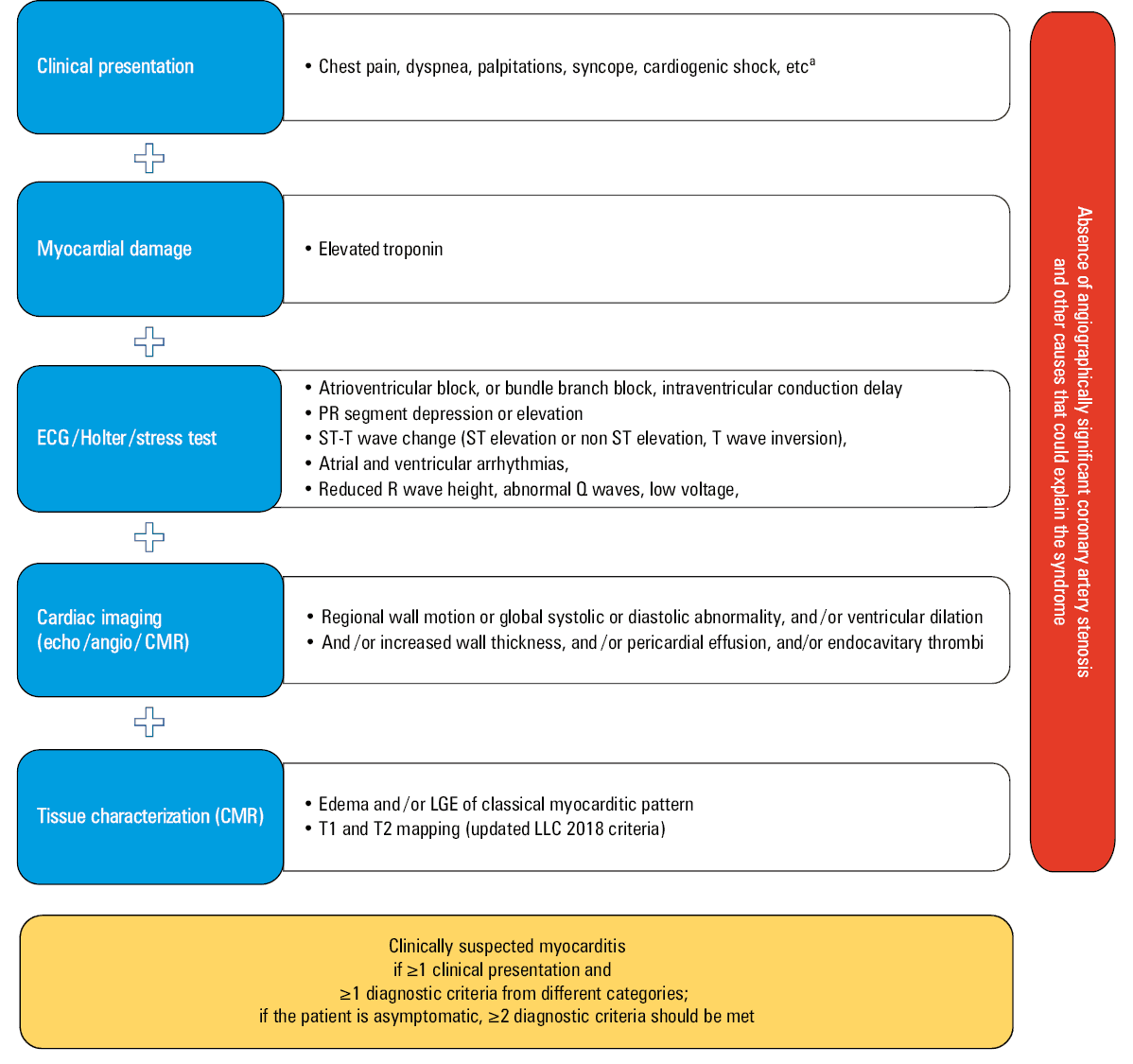
a Fever within the last 30 days with signs of respiratory or gastrointestinal infection; peripartum period; previous clinically suspected or definite myocarditis; personal and / or family history of allergic asthma, other types of allergy; extracardiac autoimmune disease; toxic agents; family history of dilated cardiomyopathy or myocarditis
Abbreviations: AHA, American Heart Association; angio, angiography; CMR, cardiac magnetic resonance; ECG, electrocardiography; echo, echocardiography; ESC, European Society of Cardiology; LGE, late gadolinium enhancement; LLC, the Lake Louis Criteria
In particular, significant changes in coronary arteries or other conditions (eg, significant valvular heart defects, congenital heart disease, stress‑induced cardiomyopathy) should always be ruled out. In patients with a low pretest probability of coronary artery disease, noninvasive imaging modality, such as computed tomography angiography, should be preferred.19 Finally, in selected autoimmune / immune‑mediated diseases, myocarditis may be a part of the clinical picture.
Noninvasive diagnostics
Electrocardiogram
Although there are no pathognomonic changes associated with myocarditis, electrocardiogram (ECG) is usually abnormal (Figure 2).1 Most commonly, ST‑T wave abnormalities are observed. Atrioventricular block can be indicative of laminopathy, Lyme disease, cardiac sarcoidosis, or giant cell myocarditis.1 ECG parameters may correlate with abnormal tissue characteristics on cardiac magnetic resonance (CMR) and have some prognostic value.20,21
Biomarkers
There is no specific serum biomarker of inflammation in myocarditis, though erythrocyte sedimentation rate and C‑reactive protein levels may be elevated.1 An accompanying elevated eosinophil count may suggest a secondary disorder (eg, parasitic infection, allergy, drug- or vaccine‑related hypersensitivity reaction, myeloproliferative disease) or an idiopathic hypereosinophilic syndrome (eg, Loeffler syndrome, antineutrophil cytoplasmic antibodies–associated vasculitis).1
The serum troponin level, a recognized biomarker for detecting myocardial injury, is recommended by the European Society of Cardiology (ESC), but it is neither sensitive nor specific for myocarditis.1 Troponin levels can be elevated in over one‑third of patients with myocarditis, but they do not seem to have the same prognostic value in acute myocarditis as in acute coronary syndromes.1,22 Natriuretic peptides should be obtained when HF is suspected, but values within reference range do not exclude myocarditis.23 The usefulness of other cardiac biomarkers is limited.
In appropriate clinical settings, laboratory investigation can be particularly helpful in confirming or ruling out specific SIDs associated with cardiac involvement (hypereosinophilic syndromes, antineutrophil cytoplasmic antibodies–associated vasculitis, sarcoidosis, systemic lupus erythematosus, idiopathic inflammatory myopathies, etc).
Viral serology is no longer recommended since it does not correlate with the EMB‑proven diagnosis of myocardial infection.1
Detectable specific serum AHAs suggest an immune‑mediated myocarditis or inflammatory cardiomyopathy.1,16,17,24-26 AHAs are IgG class serum antibodies which, beyond specificity for myocarditis and inflammatory cardiomyopathy, have been proven to also be reliable biomarkers for identifying the patients’ relatives who are at risk.1 More recently, AHAs and intercalated disk autoantibodies have been described as providing markers of autoimmune involvement in arrhythmogenic right ventricular cardiomyopathy for patients and their relatives.27
Echocardiography
Standard echocardiographic evaluation with tissue‑Doppler imaging analysis is an integral imaging modality in the initial diagnostic workup in all patients with suspected myocarditis, also during follow‑up (Figure 2).1,8 Indeed, echocardiographic changes can differentiate acute (nondilated hypokinetic left ventricle [LV], and / or a transient increase in wall thickness, and / or pericardial effusion, and / or cardiac thrombus) and chronic myocarditis, and also help to rule out other conditions. Speckle tracking echocardiography (STE) is a useful tool in the detection of subclinical myocardial dysfunction and should be implemented into routine clinical practice; it may reveal intrinsic cardiac deformation with high sensitivity and reproducibility and correlate with EMB results.28 Moreover, STE show a prognostic role, particularly when the LV ejection fraction (LVEF) is still preserved.29
Cardiac magnetic resonance imaging
Cardiac magnetic resonance is the preferred noninvasive imaging tool for the diagnosis of suspected myocarditis, since it is able to identify a substantial number of heart diseases that usually go undetected on echocardiography.30 Cardiac magnetic resonance provides essential information about the morphology and function of cardiac structures and has also a unique potential for myocardial tissue characterization.1,9,31
Myocardial edema, hyperemia, and capillary leaking in early gadolinium enhancement as well as myocyte necrosis and fibrosis in late gadolinium enhancement (LGE), are usually considered primary imaging markers of inflammation.32,33 Acute inflammation and cell injury cause edema that is detected by T2‑weighted sequences. The release of inflammatory mediators produces regional coronary microvasculature dilatation and hyperemia, which in turn increases local gadolinium (a CMR contrast agent) uptake. Gadolinium accumulates in the extracellular space where it increases the T1 signal, allowing detection of edema in myocardial tissue.32 Hyperemia and consequent global enhancement of the myocardium are indicative of pre- and post‑contrast T1‑weighted sequences. Detection of LGE suggests myocardial scarring and fibrosis.32-34
The Lake Louis Criteria (LLC) 2009, consisting of a few CMR techniques (late enhancement sequences, T2‑weighted edema images, and T1‑weighted sequences [before and after contrast injection—early enhancement]), are widely adopted in the diagnosis of suspected myocarditis.32 When 2 of 3 criteria are met, the LLC have higher sensitivity (of 67%) and specificity (of 91%) in the diagnosis of acute myocarditis compared with single CMR techniques alone, but the accuracy decreases in patients with chronic manifestation.15,32,35 Recently, the LLC were supplemented by novel quantitative imaging parameters (T1 and T2 mapping sequences) and should be used routinely.33,36-38 All myocardial areas involving a pathologic process (ie, edema, fibrosis) lead to increased T1 and T2 relaxation times and expansion of the extracellular volume. T1 and T2 mapping sequences provide direct quantification of T1, T2, including extracellular volume fraction values of the myocardium, and show more extensive myocardial involvement.33,34 Clinical evidence demonstrates that adding these novel techniques improves diagnostic accuracy in detecting acute, chronic and subclinical myocarditis.33,34,38,39
Nevertheless, CMR cannot replace EMB in the diagnostic workup of myocarditis.1 The diagnostic utility of CMR is particularly limited in patients with chronic cardiomyopathy and in the presence of frequent ventricular and atrial arrhythmias.
Nuclear imaging
The 2013 ESC recommendations did not support nuclear imaging in the diagnostic workup of myocarditis because of insufficient evidence.1 A promising imaging method that could improve the accuracy of the diagnostic process is 18F‑2‑fluoro‑2‑deoxy‑D‑glucose positron emission tomography (FDG‑PET). It is capable of detecting inflamed tissue via increased glucose uptake and therefore provide metabolic information on ongoing myocardial inflammation.40,41 FDG‑PET might be particularly useful in chronic myocarditis where CMR accuracy is low.42 FDG‑PET imaging already has an established role in the detection of cardiac and extracardiac localizations of sarcoidosis and therapy monitoring.43 Moreover, FDG‑PET is allowed in patients with metallic implants, CMR‑incompatible heart valves, or cardiac devices. Nevertheless, FDG‑PET requires appropriate dietary preparation to suppress physiological glucose uptake and is associated with radiation exposure.
Invasive diagnostics—endomyocardial biopsy
Nowadays, EMB is the only method enabling a certain diagnosis of myocarditis. The current ESC position statement recommends consideration of EMB in all patients with clinically suspected myocarditis (Table 3).1 If routinely performed in patients with suspected myocarditis, EMB would be of great clinical and scientific value, providing valuable information about etiology and the true prevalence of the disease.
Guidelines | Recommendation |
ESC 20131 | EMB should be considered in all patients with clinically suspected myocarditis. |
EMB may be repeated if necessary, to monitor response to aetiology‑directed therapy, or if a sampling error is suspected in a patient with unexplained progression of HF. | |
ESC 201651 | EMB should be considered in patients with rapidly progressive HF despite standard therapy when there is a probability of a specific diagnosis which can be confirmed only in myocardial samples and specific therapy is available and effective. |
AHA 201659 | EMB should be performed in clinically suspected unexplained acute myocarditis which require inotropic support or MCS; Mobitz type 2 second‑degree or higher heart block; sustained or symptomatic ventricular tachycardia; failure to respond to guideline‑based medical management within 1 to 2 weeks. |
EMB may be considered in patients with clinically suspected myocarditis. | |
Endomyocardial biopsy, using broad histological, immunohistochemical, and biomolecular (polymerase chain reaction [PCR], in situ hybridization) analyses, allows for: detecting active / chronic / healed myocarditis; defining the type of inflammation (eg, lymphocytic, in 95%, eosinophilic, giant cell, sarcoid); defining the underlying etiology; establishing the presence of viral infection; describing myocardial fibrosis qualitatively and quantitatively; adjusting treatment; and monitoring outcomes (Figure 2).1,44 What is more, EMB provides key clues for differential diagnosis (ie, arrhythmogenic right ventricular cardiomyopathy, peripartum cardiomyopathy, Takotsubo cardiomyopathy, infiltrative / storage disorders).31
Importantly, the complication rate of EMB is low (0%–0.8%)1,26,44 in experienced centers. In a large single‑center study, summarizing over 4000 EMB treatments, no patient died and the rate of major complications (including perforation with or without cardiac tamponade, embolization) was 0.33% for left and 0.45% for right ventricular EMB.44 The principal EMB complications are mainly vascular and include hematoma, aneurysm, atrioventricular fistula, vasovagal reaction, but also less frequently infection, pneumothorax, heart block (mostly transient), arrhythmia, tricuspid or aortic valve damage, systemic embolism, and heart perforation with hemopericardium or cardiac tamponade.44-46
Techniques and general sampling
Commonly, EMB is performed under local anesthesia with fluoroscopic or echocardiographic guidance using femoral or jugular venous access, while LV EMB is carried out with arterial access (femoral or radial / brachial).47,48 There are no strict recommendations indicating which ventricle should be chosen for EMB. However, there are data indicating that biventricular EMB might increase diagnostic accuracy of myocarditis and idiopathic cardiomyopathies.44 Particularly in suspected cardiac sarcoidosis, giant cell myocarditis, unexplained cardiomyopathy, echocardiographic or CMR abnormalities suggesting isolated LV involvement, LV or biventricular EMB may be considered.49
To increase the diagnostic accuracy and sampling error and to perform all analyses, it is necessary to gather at least 5 tissue samples (recommended 5–10), each 1 to 2 mm in size, from different regions (right ventricle mainly from the interventricular septum and LV mainly from the free wall).1,50
According to the current ESC recommendations, safe and targeted treatment of myocarditis is based on the EMB results.1 Immunosuppressive or antiviral therapy without an EMB result should be avoided. If necessary, EMB may be repeated when a sampling error is suspected, in order to monitor response to treatment, or in a patient with unexplained progression of HF.1
Treatment
Conventional and supportive therapy
Unfortunately, in most situations, treatment of myocarditis is still symptomatic. High‑quality and systematic data are absent, and most studies are small or report very heterogenous groups, without a clear diagnostic and etiologic definition, or information about “virus‑positive” or “virus‑negative” EMB‑proven myocarditis. General therapeutic management should be adjusted to the severity of the clinical profile and the occurrence of a short‑term spontaneous or treatment‑induced recovery. Patients with myocarditis presenting symptomatic HF, arrhythmias, or comorbidities should be managed according to the appropriate guidelines.51,52 However, standard cardiovascular therapy can only delay the progression of the disease to DCM. Treatment with nonsteroidal anti‑inflammatory drugs (ie, ibuprofen) is ineffective or harmful (risk of increased inflammation and mortality), and should be reserved, in combination with colchicine, only for patients with concurrent pericarditis with preserved or nearly preserved LV function.51,53 Patients with acute eosinophilic myocarditis are at a higher risk of intracardiac thrombosis and peripheral embolization, thus anticoagulation should be considered until resolution of the acute inflammatory phase.
The management of arrhythmias should mainly be supportive, as in myocarditis, arrhythmias often diminish or disappear following the resolution of acute myocardial inflammation. Patients with life‑threatening arrhythmias should be referred to centers with advanced mechanical hemodynamic and electrophysiology support.51,52 When indicated, patients with refractory or worsening arrhythmias may undergo radiofrequency endocardial or epicardial catheter ablation, although with a limited success rate.54 However, ablative management of arrhythmias in patients with active myocarditis showed moderate effectiveness (approximately 45% recurrence of premature ventricular contractions from other locations at 3‑month follow‑up).55 Recent data showed a reduced arrhythmia burden in EMB‑proven infectious negative myocarditis following a tailored immunosuppressive treatment.56 Recommendations regarding an implantable cardioverter defibrillator (ICD) should be evaluated individually.52 However, in the absence of ventricular arrhythmias, urgent ICD implantation is not recommended for patients with recent onset clinically suspected myocarditis and LVEF of less than 30%.51 In recent‑onset myocarditis, referral for a heart transplant, LV assist device, or prophylactic ICD implantation should be deferred for 3 to 6 months and reassessed.57 In patients at an increased risk of SCD, the use of a wearable cardioverter‑defibrillator may be advisable.58
Myocarditis‑specific therapy
The management of myocarditis is multidisciplinary, and a myocarditis Heart Team should always include a cardiologist, radiologist, cardiovascular pathologist, clinical immunologist, or rheumatologist as well as an infectious disease specialist.8
Immunosuppressive therapy
Although rapidly increasing, available data on the effectiveness of immunosuppressive therapy (IT) in autoimmune myocarditis are still not conclusive. The rationale for IT in autoimmune myocarditis is to suppress the immunomediated cellular and humoral response that fuels myocardial inflammation. Beyond corticosteroids, azathioprine, cyclosporine, mycophenolate mofetil, and other agents have been tested in various combinations. However, current ESC recommendations support immunosuppressive therapy in EMB‑proven, virus‑negative myocarditis / inflammatory cardiomyopathy refractory to standard therapy, particularly in patients with giant cell myocarditis, cardiac sarcoidosis and eosinophilic myocarditis, and no contraindications to IT.1,59 Giant cell myocarditis usually requires immediate and aggressive immunosuppression to prevent SCD or the need for urgent cardiac transplantation.1,60 Immunosuppression improves long‑term survival, and its withdrawal may be associated with fatal recurrence of the disease.60,61 In addition, giant cell myocarditis can recur in a grafted heart requiring more aggressive IT.1,62,63 In noninfectious eosinophilic myocarditis, immediate discontinuation of the suspected cause and administration of high dose corticosteroids are usually followed by prompt remission, though the duration of immunosuppressive therapy should be tailored to the patient; a follow‑up EMB may guide the length and intensity of immunosuppressive therapy, as well as the timing of its withdrawal.64
Two main studies reported a sustained beneficial effect of combined prednisone and azathioprine therapy on LVEF (up to approximately 90% improvement in the treatment group), along with a very favorable safety profile.5,65 However, they were both single‑center studies based on small populations that still require confirmation in larger, multicenter studies. Currently, a multicenter, randomized study (IMPROVE‑MC, EudraCT no. 2020‑003877‑23) on combined prednisone and azathioprine immunosuppression in virus‑negative myocarditis is ongoing. Selected data from the most important studies on immunosuppression in myocarditis and DCM are presented in Table 4. A recent meta‑analysis also suggested a favorable risk / efficacy profile in EMB–proven myocarditis.66
Author (trial) | Year | Population characteristics | Patients / controls, n | Patient type | Treatment (duration) | Endpoints | Results | Outcome comment | Trial comment | |
Treated patients | Controls | |||||||||
Parillo et al93 | 1989 | Total: median (IQR) age, 43 (23–67) y; LVEF, 17% (3%–35%); duration of symptoms, 8 mo (2 wk to 11 y) | 49/52 | “Reactive” patients (n = 60) vs “nonreactive” DCM (n = 42) | Prednisone vs placebo (for 3 months and then on alternate days) | LVEF after 3 mo | 53% improved; 47% unchanged / deterioration | 27% improved; 73% unchanged / deterioration | LVEF increased in 67% in reactive group vs 28% in nonreactive (P = 0.004) |
|
Mortality | No difference | No difference | ||||||||
Mason et al94 (MTT) | 1995 | Mean (SD) LVEF, 24% (10%); interventional group: age, 43 y; duration of symptoms <2 y | 64/47 | Myocarditis and LVEF <45% | Prednisone and cyclosporine or azathioprine vs placebo (for 24 wk) | LVEF after 6 mo | No difference | No difference | No benefit, no harm |
|
Mortality | No difference | No difference | ||||||||
Wojnicz et al65 | 2001 | Interventional group: age, 41 y; mean (SD) LVEF, 23.8% (8.6%); duration of symptoms >6 mo | 41/43 | Chronic (>6 months) dilated (inflammatory) cardiomyopathy + upregulation of HLA and LVEF ≤40% | Prednisone and azathioprine vs placebo (for 3 mo) | Death, heart transplantation, or hospital readmission at 2 y | No difference | No difference | LVEF improved after 3 mo and sustained after 2 y |
|
LVEF after 3 mo | Improved in majority | Improved in minority | ||||||||
Frustaci et al5 (TIMIC) | 2009 | Total: mean (SD) age, 42.7 (15.4) y; LVEF 27.1% (6.5%); duration of symptoms >6 mo | 43/42 | Active lymphocytic myocarditis (virus‑negative) and LVEF <45% | Prednisone and azathioprine vs placebo (for 6 mo) | LVEF after 6 mo | 88.3% improved; 11.7% unchanged / deterioration | 0% improved; 100% unchanged / deterioration | Favorable results sustained after 1 y |
|
Maisch et al (ESETCID) | 2011 | No data | 54/47 | Autoreactive inflammatory dilated cardiomyopathy (virus‑negative) and LVEF <45% | Prednisolone and azathioprine vs placebo (for 6 mo) | LVEF, MACE after 6 mo | LVEF + MACE improved | Some spontaneous improvement | Favorable |
|
In patients with SIDs and EMB‑proven myocarditis, disease‑specific IT regimens should be adapted in every single patient in order to achieve remission. In fact, current evidence seems to support more intensive and prolonged IT in patients with SIDs and infectious‑negative autoimmune / immune‑mediated myocarditis.31
Immunomodulatory therapy
The efficacy of intravenous immunoglobulin (IVIG) in the treatment of myocarditis is still debatable. A recently published meta‑analysis (1534 cases from 13 studies, mainly children) showed that in patients with suspected acute myocarditis, IVIG therapy reduced in‑hospital mortality and increased LVEF, and was well tolerated.67 However, it should be pointed out that most of the included studies were not based on EMB‑proven myocarditis and had no clear etiological definition, and that one study reporting a neutral effect on LV was excluded from the meta‑analysis.68 In addition, another meta‑analysis on the pediatric population showed no improvement in survival rates.69 Thus, IVIG are not currently recommended in the treatment of myocarditis / inflammatory DCM and further prospective controlled studies are needed to clarify their therapeutic role.1
Antiviral therapy
No efficacy‑proven antiviral therapy is still approved for virus‑positive myocarditis. The role of viral infection remains controversial. What is more, a recently published meta‑analysis of 10 studies (1006 patients with myocarditis or DCM) showed no significant difference in the prognosis of virus‑positive and virus‑negative patients.70 However, in the setting of infective myocarditis, a targeted antiviral therapy may be used, both in acute and chronic myocarditis. Some efficacy was shown for antiretroviral drugs and targeted antibiotic therapy for opportunistic infections in HIV EMB‑proven myocarditis; acyclovir, ganciclovir, and valacyclovir are used for herpes virus infection and targeted therapy for influenza or Lyme disease myocarditis.1,31 In patients with a EMB‑confirmed viral infection (enterovirus, adenovirus, and / or parvovirus B19 genomes), treatment with interferon beta was shown to improve viral clearance, quality of life, LV function, and New York Heart Association (NYHA) class and was also well tolerated.71,72 In another study, both spontaneous enterovirus clearance and interferon beta administration were associated with better survival rates than persistent infection.6
Long‑term follow‑up and prognosis: the role of a myocarditis outpatient clinic
According to our experience and the current literature, a prospectively scheduled close follow‑up (at least 6 months) after the diagnosis of myocarditis is of great importance in prognostic stratification and disease management. A suggested short‑term evaluation scheme depending on the initial presentation and EMB result is presented in Figure 3.
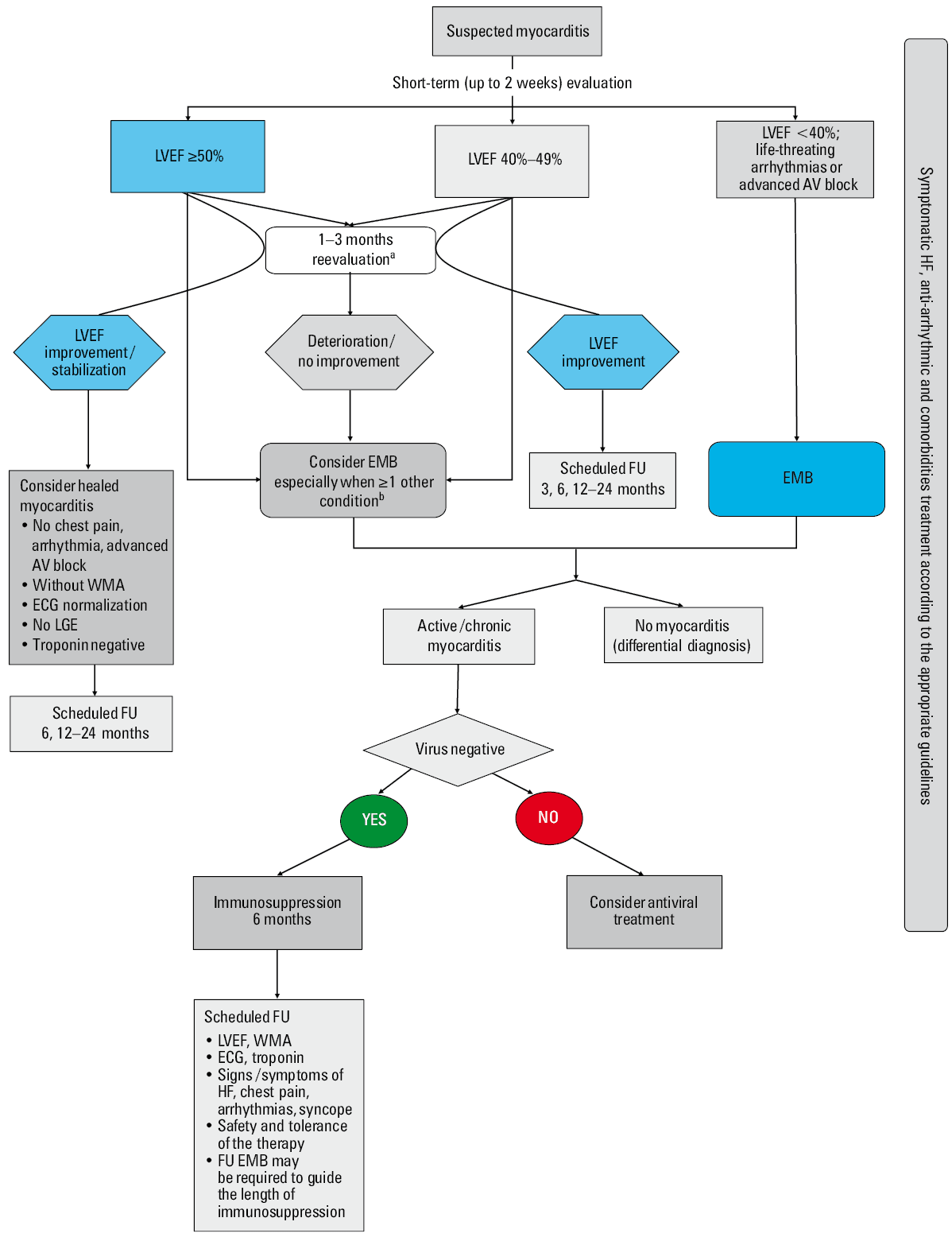
a ECG, Holter ECG, troponin measurement, echocardiographic reassessment, consider exercise test
b Persistently elevated or increase in troponin level; context of autoimmune disease; potential triggers (drugs, allergens); persistent cardiac arrhythmia and/or chest pain; persistent WMA and/or decrease in LVEF; LGE areas at baseline; positive AHA if available
Abbreviations: AV, atrioventricular; FU, follow‑up; WMA, wall motion abnormalities; others, see Figures 1 and 2, Tables 3 and 4
In patients with EMB‑proven myocarditis, reported long‑term (the median follow‑up was 4.7 years) all‑cause mortality was 19.2%, while SCD occurred in 9.9% of patients.73 Spontaneous or treatment‑induced improvement (40%–50%; up to 90%, respectively) of LV function occurs within a few months of the disease onset.5,31,57 Therefore, the identification of reliable early predictors of long‑term outcomes is crucial for the prognosis and clinical management.
Follow‑up evaluation is mainly based on clinical (sign and symptoms of HF and / or arrhythmia, chest pain), biochemical (troponin), ECG, and echocardiographic assessment (including STE), but additional tests (Holter‑ECG, exercise test, CMR) may also be useful.1,31,57 Although CM may also be useful, its role in follow‑up is not clear; therefore, the routine use of CMR for disease monitoring is currently not recommended. Persistence of LGE and disappearance of edema are more likely associated with worse prognosis compared with complete resolution or persistence of both LGE and edema. Persistent edema can suggest an ongoing process with some residual chance of recovery.74
Infarct‑like presentation of myocarditis is predominantly associated with excellent prognosis and spontaneous resolution, mainly when accompanied by preserved LV function at baseline, no wall motion abnormalities, stable arrhythmic profile and resolution of ECG abnormalities.31,57,75,76 Worse outcomes (60% heart transplant‑free 10‑year survival) are associated with symptomatic HF, malignant ventricular arrhythmias, severe atrioventricular conduction abnormalities, and / or fulminant myocarditis presentation.57
The most commonly reported factors associated with negative prognosis in myocarditis are: positive viral PCR, giant‑cell myocarditis etiology, reduced LVEF, NYHA class II–IV, LGE at baseline, and the persistence of a viral genome in cardiac tissue at follow‑up. The persistence of symptomatic HF (NYHA class III–IV) and improvement / normalization of LVEF (defined as LVEF increase of 20% or LVEF >50%) within the first 6 months emerged as independent predictors of long‑term outcomes.77 Baseline LGE was found to be a powerful (and stronger than LVEF) predictor of outcomes (all‑cause mortality or cardiovascular death, resuscitated cardiac arrest, heart transplantation, appropriate ICD shock, rehospitalization, and recurrent acute myocarditis), irrespective of LVEF.73
In a few studies, the troponin level was reported to be not relevant to the prognosis of acute myocarditis in adults or children.31,76 Nevertheless, troponin and / or natriuretic peptides may be useful in monitoring HF evolution and response to therapy.31
The prevalence of ventricular arrhythmias in myocarditis varies by LVEF, LGE presence, and histological type, and is higher in cardiac sarcoidosis, giant cell and eosinophilic hypersensitivity myocarditis than in lymphocytic myocarditis.35,78,79 Polymorphic and irregular ventricular arrhythmias are more common in active myocarditis, while monomorphic and regular ventricular arrhythmias are associated with healed myocarditis.80 On the other hand, there are limited data on the burden and prevalence of atrial arrhythmias in patients with myocarditis.
Optimal duration of pharmacotherapy after restoration of LV function has not been defined and should be individualized, because relapses and recurrences are observed. No specific test, apart from EMB, can establish complete resolution of inflammation in myocarditis and this can be particularly important in the certification of athletes. In selected patients, a follow‑up EMB may be required in orienting IT intensity and extension.1
Physical activity
Physical activity should be restricted for at least 6 months from the onset of myocarditis, depending on clinical severity, LV function, and the extent of inflammatory changes on CMR at baseline.1,59 This applies both to competitive and amateur exercise regardless of age, gender, clinical presentation, and applied treatment.1 In myocarditis, especially when associated with strenuous physical exertion, SCD may occur despite normal LV function (myocarditis was detected in up to 20% of athletes who experienced SCD).81 In the murine model of coxsackie virus myocarditis, physical activity was shown to be associated with increased viral load, progression of cardiomyopathy, and increased risk of death.82 Patients with a previous episode of myocarditis are also at an increased risk of progression and / or recurrence of the disease and require periodical reassessment, especially within the first 2 years.
Before returning to sporting activity, patients should be carefully re‑evaluated. Clinical and functional testing is indicated1,59 and the following criteria should be met: normality of LVEF and serum cardiac biomarkers, absence of clinically relevant arrhythmias on 24‑h ECG and exercise test, and no evidence of ongoing inflammation or fibrosis on CMR.1,59,81 The significance of persistent LGE in a clinically healed myocarditis is unknown, though myocardial fibrosis represents a potential risk factor for ventricular arrhythmias; consequently, athletes should remain on annual clinical reassessment.83-85 Patients with extensive LGE area (>20%) and persistent LV dysfunction should abstain from moderate‑intensive exercise.81 Consultation with an arrhythmia and sports specialist is suggested in challenging cases.
COVID‑19 myocarditis
Clinically suspected myocarditis has also been reported in SARS‑CoV‑2 acute respiratory syndrome, yet conclusive evidence that SARS‑CoV‑2 is a novel cardiotropic virus is still lacking.10,86,87 Cardiac dilatation, wall motion abnormalities, ischemia, troponin release, thrombi, and / or pericardial effusion are commonly observed and constitute an element of post‑COVID‑19 syndrome.88 CMR studies show conflicting results with a very high to low complication rate of fibrosis (LGE areas) or active myocardial edema meeting the LLC for myocarditis.89,90 COVID‑19 myocarditis can develop during the acute phase or weeks / months after the SARS‑CoV‑2 infection. The severity of COVID‑19 does not correlate with the risk of myocarditis. It seems that the mechanism of myocarditis as a complication of COVID‑19 is mainly immune‑mediated. SARS‑CoV‑2 can also invade the myocardium; however, a typical lymphocytic myocarditis with viral presence is rare.91
Conclusions
Myocarditis represents a growing challenge for physicians and requires highly integrated multidisciplinary management by an experienced myocarditis Heart Team. Besides standardized protocols, integration of novel immunological (AHA), echocardiographic (STE), CMR (updated LLC), and nuclear imaging techniques for decision‑making is advisable. Still, EMB is the diagnostic gold standard and represents a key tool for etiological and differential diagnosis. There are more and more available data supporting the efficacy of IT in EMB‑proven myocarditis: giant cell, eosinophilic, immune‑mediated, and virus‑negative lymphocytic myocarditis. However, further controlled, multicenter clinical trials are required to confirm prior studies and to collect more data regarding etiology‑oriented therapies. Finally, organization of a myocarditis outpatient clinic and implementation of specific screening and follow‑up schedules for myocarditis patients seem particularly advisable.
- Caforio AL, Pankuweit S, Arbustini E, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013; 34: 2636‑2648, 2648a‑2648d. | Crossref
- Lynge TH, Nielsen TS, Gregers Winkel B, et al. Sudden cardiac death caused by myocarditis in persons aged 1‑49 years: a nationwide study of 14 294 deaths in Denmark. Forensic Sci Res. 2019; 4: 247‑256. | Crossref
- Fabre A, Sheppard MN. Sudden adult death syndrome and other non‑ischaemic causes of sudden cardiac death. Heart. 2006; 92: 316‑320. | Crossref
- Disease GBD, Injury I, Prevalence C. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990‑2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018; 392: 1789‑1858.
- Frustaci A, Russo MA, Chimenti C. Randomized study on the efficacy of immunosuppressive therapy in patients with virus‑negative inflammatory cardiomyopathy: the TIMIC study. Eur Heart J. 2009; 30: 1995‑2002. | Crossref
ARTICLE INFORMATION