High-flow nasal oxygen therapy in the treatment of acute respiratory failure in severe COVID-19 pneumonia: a prospective observational study
Key words: acute respiratory failure, COVID-19, high-flow nasal oxygen, pneumonia, ROX index



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
High-flow nasal oxygen therapy in the treatment of acute respiratory failure in severe COVID-19 pneumonia: a prospective observational study
Introduction: A significant proportion of patients with COVID‑19 present with a rapidly progressing severe acute respiratory failure.
Objectives: We aimed to assess the efficacy of high‑flow nasal oxygen (HFNO) therapy in severe acute respiratory failure in the course of COVID‑19 in a noncritical care setting as well as to identify predictors of HFNO failure.
Patients and methods: This prospective observational study was conducted between March and December 2020. We enrolled all consecutive patients hospitalized with confirmed SARS‑CoV‑2 infection in whom HFNO therapy was used. The primary outcome was death or endotracheal intubation within 30 days from admission.
Results: Of the 380 patients with COVID‑19 hospitalized at our tertiary center, 116 individuals (30.5%) requiring HFNO due to severe pneumonia were analyzed. The primary outcome occurred in 54 patients (46.6%). The overall 30‑day mortality rates were 30.2% (35 out of 116 patients) in the entire cohort and 64.7% (34 out of 51 patients) among individuals requiring endotracheal intubation. A multivariable analysis revealed that the ROX index (the ratio of oxygen saturation / fraction of inspired oxygen to respiratory rate) below 3.85 measured within the first 12 hours of therapy was related to increased mortality (hazard ratio, 5.86; 95% CI, 3.03–11.35) compared with the ROX index of 4.88 or higher.
Conclusions: The results of our study suggest that nearly half of patients treated with HFNO due to severe COVID‑19 pneumonia will require mechanical ventilation. The ROX index is a useful tool for predicting HFNO failure in this population.
What's new?
The clinical presentation of COVID‑19 varies from asymptomatic infection to severe illness. A significant proportion of patients present with a rapidly progressing acute respiratory failure and require invasive mechanical ventilation. High‑flow nasal oxygen (HFNO) therapy is a technique consisting in delivering heated and humidified oxygen at high flows through a nasal cannula. The HFNO therapy in acute hypoxemic respiratory failure may help avoid intubation and mechanical ventilation. This prospective observational study showed that nearly half of patients with severe COVID‑19 pneumonia eventually required invasive mechanical ventilation and almost a third of these patients died within 30 days from hospital admission. Our results suggest that the ROX index (defined as the ratio of oxygen saturation / fraction of inspired oxygen to respiratory rate) may be a useful tool for stratification of HFNO failure risk in this population.
Introduction
The clinical presentation of COVID‑19 is highly variable and the disease affects multiple organs, with predominant involvement of the respiratory system. Approximately 15% of cases are severe, warranting hospitalization, and 5% of patients require admission to the intensive care unit (ICU).1 The highly contagious nature of SARS‑CoV‑2 in conjunction with the lack of effective causal treatment led to an exponential increase in the number of cases and a huge burden on healthcare systems globally. Since the first case of COVID‑19 in Poland had been confirmed in March 2020, almost 1.3 million Polish citizens got infected with SARS‑CoV‑2, with a peak monthly incidence of 400 000 new active cases in November 2020. Poland is characterized by one of the lowest ICU‑to–hospital bed ratios in the European Union (2%–5%), rendering the public healthcare system particularly prone to failure in the face of an increased patient load.2,3
A significant proportion of patients with COVID‑19 present with a rapidly progressing acute respiratory failure (ARF) and eventually require mechanical ventilation. The initially suggested approach included early intubation and mechanical ventilation with lung‑protective strategy recommended by the Acute Respiratory Distress Syndrome Network trial.4 Since the mortality of invasively ventilated patients remained high, it was hypothesized that some individuals with severe COVID‑19 pneumonia may benefit from other oxygenation improvement strategies allowing to avoid invasive mechanical ventilation and its adverse effects, that is, ventilator‑induced lung injury and ventilator‑associated pneumonia.5,6 Hence, high‑flow nasal oxygen (HFNO) therapy was suggested as an optimal treatment modality in this setting.
The HFNO therapy involves delivery of oxygenated gas, heated and humidified to body conditions, via a nasal cannula at a maximum flow up to 80 l/min.7,8 The therapy is believed to have numerous benefits, including adequate humidification, reduction of anatomical dead space and work of breathing, as well as an increase in end‑expiratory lung volume due to the provision of positive end‑expiratory pressure. During the past years, its use in the critical care setting has extended to treatment of hypoxemic ARF after extubation as well as postoperative treatment of high‑risk or obese patients.9 Previous studies, mainly retrospective in design and with a limited sample size, suggested potential benefits associated with the use of HFNO in the treatment of respiratory failure in COVID‑19.10-13
Facing the growing number of patients with severe respiratory failure due to COVID‑19 along with insufficient ICU resources, our tertiary center adopted the strategy of HFNO administration by experienced respiratory physicians in noncritical care setting. The aim of this study was to assess the therapeutic success of HFNO in severe respiratory failure in the course of COVID‑19. Our secondary goal was to identify factors associated with HFNO failure.
Patients and methods
Study design
This was a prospective observational study conducted between March and December 2020 at the Department of Pulmonology and Allergology, University Hospital in Kraków, Poland. The study protocol complied with the Declaration of Helsinki and was approved by the Ethics Committee of Jagiellonian University Medical College, Kraków, Poland (KBET 1072.6120.145.2020) on May 28, 2020. The study participants provided written informed consent and were informed that the HFNO therapy was introduced regardless of this study, in accordance with the guidelines for the treatment of respiratory failure in COVID‑19.
Patients and data collection
We enrolled all consecutive patients with confirmed SARS‑CoV‑2 infection admitted to our center in whom HFNO therapy was used. Patients in whom the goal of care did not include intubation and invasive mechanical ventilation and those in whom HFNO was used after successful extubation were excluded from analysis. Study personnel collected detailed demographic and clinical data (including symptoms, comorbidities, vital signs, laboratory results, and imaging studies) based on history taking and available medical records.
High‑flow oxygen therapy
The indication for administration of HFNO was severe respiratory failure defined as the necessity to receive oxygen supplementation with fraction of inspired oxygen (FiO2) of 50% or higher to achieve satisfactory oxygen saturation (SpO2). High‑flow nasal oxygen was delivered by an Airvo 2 device (Fisher & Paykel Healthcare, Irvine, California, United States). The HFNO flow and FiO2 were titrated to achieve an SpO2 between 92% and 96% for patients without hypercapnia and between 88% and 92% for those with hypercapnia. In each patient, we recorded initial and maximal HFNO settings. Additionally, within the first 12 hours of HFNO therapy, we recorded FiO2, SpO2, and respiratory rate to calculate the ROX index. Respiratory rate and SpO2 were measured automatically by continuous patient monitoring systems. According to the formula presented by Roca et al,14 ROX index is defined as the ratio of SpO2/FiO2 to respiratory rate. For subjects in whom invasive mechanical ventilation was initiated within 12 hours from admission, we recorded the above parameters at the time of decision to intubate.
The primary outcome was a composite of death and endotracheal intubation within 30 days from enrollment.
Statistical analysis
Categorical variables were presented as numbers (percentages), whereas continuous variables were reported as medians with interquartile ranges (IQRs) or means with SDs, depending on the distribution. Quantitative data were analyzed using the t test or Mann–Whitney test. An adjusted analysis of factors associated with the incidence of primary outcome was performed using a Cox proportional hazard model including selected variables, such as age, sex, diagnosis of obesity, D‑dimer level on admission, disease stage (defined as early for patients with ≤7 days from symptom onset to HFNO therapy initiation and late for patients with >7 days from symptom onset to HFNO therapy initiation), and ROX category (≥4.88, 3.85–4.87, and <3.85).14 The analysis was performed after confirmation that the proportional hazards assumption was justified. The variables included in the model were selected based on our knowledge as well as the available evidence. This was a complete‑case analysis. A 2‑sided P value of less than 0.05 was considered significant. All analyses were performed using R, version 3.6.0 (the R Project for Statistical Computing, Vienna, Austria) with the following packages: rms, survival, survminer, and ggplot2.
Results
Patients
The study group initially comprised 380 patients with confirmed COVID‑19, of whom 125 (32.9%) required HFNO therapy. Of those, 9 patients (7.2%) in whom endotracheal intubation was not the goal of care were excluded. Thus, a total of 116 patients were included in the final analysis (Figure 1). No patient was lost to 30‑day follow‑up.
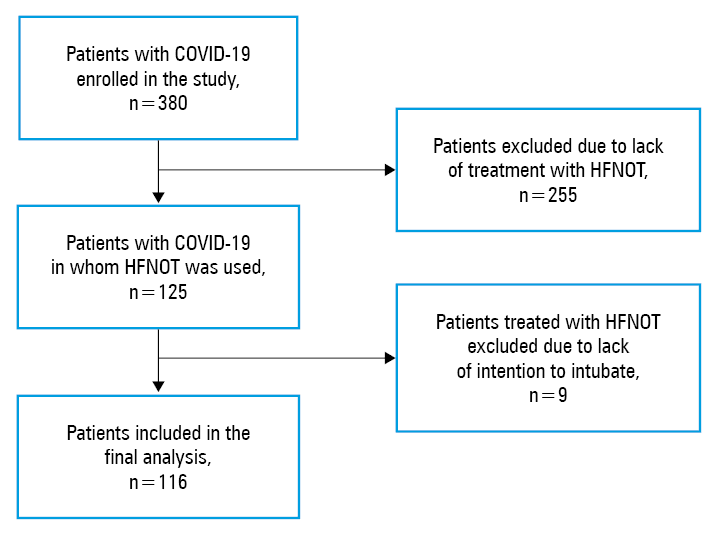
Abbreviations: HFNOT, high‑flow nasal oxygen therapy
The final study group included 91 men (78.4%) and 25 women (21.6%). The median (IQR) age was 61 (51–70) years. The most common comorbidities were hypertension (57.8%), obesity (37.1%), and diabetes (31%). On admission, the median (IQR) Modified Early Warning Score and SpO2/FiO2 ratio were 2 (1–3) and 101.1 (94.7–192.3), respectively. Dexamethasone was administered in 104 patients (89.7%), remdesivir in 71 (61.2%), and convalescent plasma in 17 (14.7%). Detailed demographic and clinical characteristics of the study group are presented in Table 1.
Parameter | Value | ||
Data are presented as median (interquartile range) or number (percentage).
a Patients receiving low‑molecular‑weight heparin
SI conversion factors: to convert D‑dimer to nmol/l, multiply by 5.476; LDH to μkat/l, by 0.0167; pCO2 and pO2 to kPa, by 0.133.
Abbreviations: BMI, body mass index; CRP, C‑reactive protein; HFNO, high‑flow nasal oxygen; IL‑6, interleukin 6; LDH, lactate dehydrogenase; LMWH, low‑molecular‑weight heparin; MEWS, Modified Early Warning Score; pCO2, carbon dioxide; pO2, oxygen; SpO2/FiO2, ratio of blood oxygen saturation to inspired oxygen fraction | |||
Demographic data, measurements, and comorbidities | |||
Age, y | 61 (51–70) | ||
Male sex | 91 (78.4) | ||
BMI, kg/m2 | 29.41 (26.08–32.95) | ||
MEWS score on admission | 2 (1–3) | ||
Hypertension | 67 (57.8) | ||
Chronic heart failure | 14 (12.1) | ||
Coronary artery disease | 17 (14.7) | ||
Diabetes mellitus | 36 (31) | ||
Obesity | 43 (37.1) | ||
Chronic kidney disease | 12 (10.3) | ||
Obstructive lung disease | 13 (11.2) | ||
Laboratory results on admission | |||
D‑dimer, mg/l | 1.17 (0.78–3.29) | ||
LDH, U/l | 522 (392–620.5) | ||
CRP, mg/l | 125.5 (72.4–199.25) | ||
IL‑6, pg/ml | 69.19 (30.52–110.33) | ||
Arterial blood gases | pO2, mm Hg | 65 (56.5–77.55) | |
pCO2, mm Hg | 34 (31.1–38.15) | ||
pH | 7.45 (7.42–7.48) | ||
Lactate, mmol/l | 1.4 (1.2–1.9) | ||
Oxygen requirement and respiratory parameters | |||
SpO2/FiO2 on admission | 101.05 (94.74–192.25) | ||
Initial FiO2 on HFNO, % | 80 (65–90) | ||
Initial respiratory rate on HFNO | 22 (20–28) | ||
Max FiO2 on HFNO, % | 92 (77.5–95) | ||
Initial flow on HFNO, l/min | 60 (50–60) | ||
Max flow on HFNO, l/min | 60 (60–60) | ||
Duration of HFNO therapy, d | 6 (2–9) | ||
ROX index at 12 h of treatment | 5.11 (4.11–6.69) | ||
Pharmacotherapy | |||
Systemic steroids | 104 (89.7) | ||
Remdesivir | 71 (61.2) | ||
Convalescent plasma | 17 (14.7) | ||
LMWHa | Therapeutic dose | 68 (58.6) | |
Intermediate dose | 41 (35.3) | ||
Prophylactic dose | 5 (4.3) | ||
High‑flow oxygen therapy
Among the 116 patients requiring HFNO, the median (IQR) initial flow and FiO2 were 60 (50–60) l/min and 80% (65%–90%), while the median (IQR) maximum values were 60 (60–60) l/min and 92% (77.5%–95%), respectively. The ROX index (n = 113) calculated within the first 12 hours of HFNO therapy was 4.88 or higher in 63 patients (55.8%), 3.85 to less than 4.88 in 30 patients (26.5%), and less than 3.85 in 20 patients (17.7%). More detailed data concerning HFNO therapy and arterial blood gas analysis are presented in Table 1. The median (IQR) duration of hospitalization was 20 (13–29) days, while the median (IQR) length of ICU stay was 10 (6–15.5) days.
Primary outcome
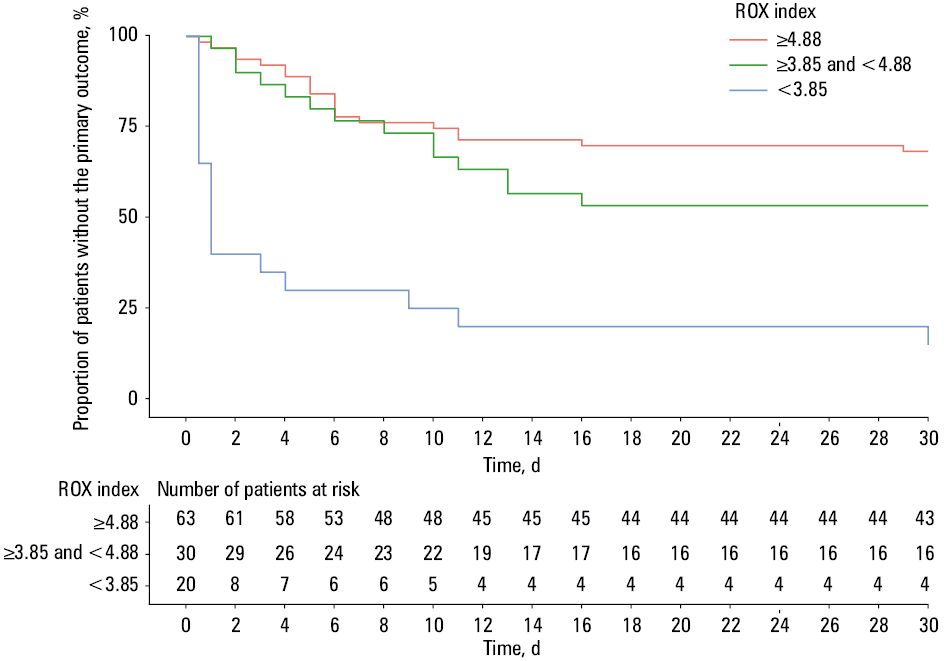
The primary outcome occurred in 54 patients (46.6%). The Kaplan–Meier curves showing the probability of not developing the primary outcome stratified by the ROX index category are presented in Figure 2. Endotracheal intubation was performed in 51 patients (44%). The 30‑day mortality rates were 30.2% (35 out of 116 patients) for the entire study group and 64.7% (34 out of 51 patients) for those requiring endotracheal intubation.
Univariable analysis showed that patients in whom the primary outcome occurred were older (63 vs 58 years; P = 0.01), had higher baseline levels of lactate dehydrogenase (555 vs 504.5 U/l; P = 0.01), higher lactate levels (1.6 vs 1.3 mmol/l; P = 0.03), and a significantly lower ROX index (4.49 vs 5.47; P <0.001) compared with the rest of the study group (Table 2). We did not find any differences in the duration of hospitalization (18 vs 20 days; P = 0.6). There was also no difference in the median time from initiation of HFNO therapy to endotracheal intubation between survivors and nonsurvivors (1 vs 3 days; P = 0.45). The groups did not differ in terms of administration of systemic steroids (93.5% vs 85.2%; P = 0.24), remdesivir (67.7% vs 53.7%; P = 0.18), and convalescent plasma (16.1% vs 13%; P = 0.83).
Parameter | Primary outcome not achieved (n = 62) | Primary outcome achieved (n = 54) | P value | ||
Data are presented as median (interquartile range) or number (percentage).
For conversion factors to SI units, see Table 1.
Abbreviations: see Table 1 | |||||
Demographic data, measurements, and comorbidities | |||||
Age, y | 58 (45–66) | 63 (57.25–72.75) | 0.01 | ||
Male sex | 11 (17.7) | 14 (25.9) | 0.4 | ||
BMI, kg/m2 | 28.73 (25.72–32.65) | 30.42 (27.22–33.06) | 0.23 | ||
MEWS score on admission | 2 (1–2) | 2 (1–3) | 0.01 | ||
Hypertension | 37 (59.7) | 30 (55.6) | 0.8 | ||
Chronic heart failure | 9 (14.5) | 5 (9.3) | 0.56 | ||
Coronary artery disease | 6 (9.7) | 11 (20.4) | 0.17 | ||
Diabetes mellitus | 17 (27.4) | 19 (35.2) | 0.48 | ||
Obesity | 21 (33.9) | 22 (40.7) | 0.57 | ||
Chronic kidney disease | 4 (6.5) | 8 (14.8) | 0.24 | ||
Obstructive lung disease | 7 (11.3) | 7 (13) | 0.78 | ||
Laboratory results on admission | |||||
D‑dimer, mg/l | 1.11 (0.66–3.85) | 1.43 (0.91–2.72) | 0.16 | ||
LDH, U/l | 504.5 (370.75–567.5) | 555 (424–815) | 0.01 | ||
CRP, mg/l | 120.5 (74.28–184.25) | 143.5 (67.53–211.25) | 0.48 | ||
IL‑6, pg/ml | 51.79 (25.12–108) | 80.55 (45.81–117.75) | 0.09 | ||
Arterial blood gases | pO2, mm Hg | 70.2 (59.1–81.75) | 63 (54–70) | 0.005 | |
pCO2, mm Hg | 34.3 (30.9–38.58) | 33.6 (31.2–38) | 0.7 | ||
pH | 7.46 (7.43–7.49) | 7.44 (7.42–7.47) | 0.16 | ||
Lactate, mmol/l | 1.3 (1.02–1.6) | 1.6 (1.28–2.02) | 0.03 | ||
Oxygen requirement and respiratory parameters | |||||
SpO2/FiO2 on admission | 103.89 (100–214.77) | 98.89 (89.47–161.67) | 0.23 | ||
Initial FiO2 on HFNO, % | 75 (60–85) | 86 (70–93) | 0.001 | ||
Initial respiratory rate on HFNO | 22 (20–26) | 24 (20–28) | >0.99 | ||
Max FiO2 on HFNO, % | 85 (70–92) | 95 (93–95) | <0.001 | ||
Initial flow on HFNO, l/min | 60 (50–60) | 60 (60–60) | 0.01 | ||
Max flow on HFNO, l/min | 60 (50–60) | 60 (60–60) | <0.001 | ||
Duration of HFNO therapy, d | 7 (5.25–10.75) | 2 (2–5.75) | <0.001 | ||
ROX index at 12 h of treatment | 5.47 (4.64–7.13) | 4.49 (3.63–5.91) | 0.001 | ||
Pharmacotherapy | |||||
Systemic steroids | 58 (93.5) | 46 (85.2) | 0.24 | ||
Remdesivir | 42 (67.7) | 29 (53.7) | 0.18 | ||
Convalescent plasma | 10 (16.1) | 7 (13.0) | 0.83 | ||
LMWH | Therapeutic dose | 32 (52.5) | 36 (67.9) | 0.072 | |
Intermediate dose | 28 (45.9) | 13 (24.5) | |||
Prophylactic dose | 1 (1.6) | 4 (7.5) | |||
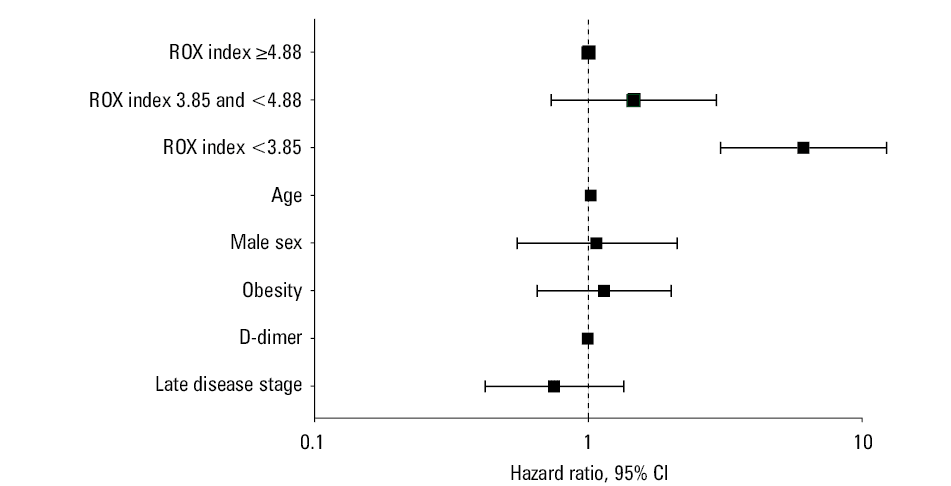
Multivariable analysis revealed that after adjustment for age, sex, obesity, baseline D‑dimer levels, and disease stage, the ROX index below 3.85 was associated with increased mortality (hazard ratio [HR], 6.1; 95% CI, 3.04–12.26), whereas the ROX index between 3.85 and 4.88 was not (HR, 1.46; 95% CI, 0.73–2.93), compared with the ROX index of 4.88 or higher (set as a reference value). The results of multivariable analysis are summarized in Figure 3 and Table 3.
Variable | HR (95% CI) | |
Abbreviations: HR, hazard ratio | ||
ROX index | ≥4.88 | Reference |
≥3.85 and <4.88 | 1.46 (0.73–2.93) | |
<3.85 | 6.10 (3.04–12.26) | |
Age | 1.02 (0.99–1.04) | |
Male sex | 1.07 (0.55–2.11) | |
Obesity | 1.14 (0.65–2.01) | |
D‑dimer | 1.00 (0.98–1.01) | |
Late disease stage | 0.75 (0.42–1.35) | |
Discussion
This single‑center prospective observational study revealed that nearly half of patients with severe COVID‑19 pneumonia eventually required invasive mechanical ventilation and almost a third of these patients died within 30 days from admission to hospital. Moreover, our results suggest that the ROX index is a valuable tool for stratification of HFNO failure risk in this population. To our best knowledge, this is the first study of HFNO therapy in severe COVID‑19 in Europe that was conducted in a cohort including more than 100 patients.
High‑flow nasal oxygen therapy is more than just oxygen supplementation. It constitutes a very well‑tolerated and easy‑to‑apply ventilatory assist device. It is widely accepted in the treatment of hypoxemic respiratory failure and its use is recommended by the Surviving Sepsis Campaign over conventional oxygen therapy in patients with severe COVID‑19 with ARF.15,16 A meta‑analysis of 9 randomized controlled trials of acute hypoxemic respiratory failure in non–COVID‑19 patients requiring HFNO revealed lower intubation rates without any influence on survival. Over half of our patients with baseline high risk for endotracheal intubation eventually avoided the primary outcome, which suggests that HFNO could potentially facilitate the prevention of mechanical ventilation in the COVID‑19 population. However, any final conclusions in this respect are hindered by the lack of a control group. Therefore, randomized controlled trials concerning the efficacy of HFNO in the prevention of intubation among patients with severe COVID‑19 pneumonia are warranted and highly anticipated.
Relatively high intubation and mortality rates observed in our cohort are consistent with the results of other available studies.17-19 Another key clinical aspect concerning the treatment of ARF in the course of COVID‑19 is the optimal timing of intubation. It has been well proven that the delay of intubation in severe ARF is associated with worse outcomes.20 A similar association in the COVID‑19 population remains unclear. In our study, there was no difference between survivors and nonsurvivors in time from admission to endotracheal intubation. Two multi‑center studies revealed contradictory results. A study by Hyman et al21 showed that each additional day between hospital admission and intubation was associated with an increased in‑hospital mortality among patients with severe ARF in the course of COVID‑19, while Dupuis and colleagues revealed that early intubation of patients admitted to ICU due to severe COVID‑19 resulted in increased mortality and number of ICU‑acquired infections.21,22
The most important practical aim of this study was to evaluate potential factors enabling identification of patients at greater risk of HFNO failure early in the course of treatment. The ROX index is considered a useful clinical tool in the prediction of HFNO success defined as avoiding endotracheal intubation among patients with acute hypoxemic respiratory failure.23 It was validated in a multi‑center prospective study in patients with non–COVID‑19 pneumonia and hypoxemic respiratory failure. The values of 2.85 or lower after 2 hours, 3.47 or lower after 6 hours, and 3.85 or lower after 12 hours of treatment were predictors of HFNO failure with a specificity of 98% to 99%. Our study suggests that the ROX index is a valuable predictive parameter among patients with severe COVID‑19 pneumonia. We found that the ROX index values lower than 3.85 measured in the first 12 hours after HFNO initiation, as proposed by Roca et al,14 were associated with a higher rate of intubation and death.
Relatively high intubation and mortality rates observed in our cohort are consistent with the results of other available studies. Compared with a study by Calligaro et al,10 the proportion of patients who required endotracheal intubation was somewhat lower in our study. Additionally, the 30‑day mortality rate in our cohort was 30% and all survivors were discharged from hospital at the time of data analysis, while in the latter study, the in‑hospital mortality rate was 46%. Another important observation is a very high mortality rate among patients requiring mechanical ventilation after HFNO therapy failure in both studies (64% in our study vs 76% in the study by Calligaro et al10). Better clinical outcomes observed in our study might be partially explained by a lower severity of ARF in our sample reflected by lower ROX index values in patients who developed the primary outcome (4.49 vs 2.41) as compared with those who did not (5.47 and 3.26). In another retrospective study involving a smaller cohort (n = 62), the authors observed a similar median ROX index of 5.4. Zucman et al12 reported the need for invasive mechanical ventilation in 63% of the population; however, interestingly, the overall mortality in the ICU was markedly lower and amounted to 17%.
The strength of this study was its prospective design and a relatively large sample collected over a short period of time, with 30‑day follow‑up completed in all participants. Patients with severe COVID‑19 without contraindications received treatment including systemic steroids, low‑molecular‑weight heparin, and remdesivir according to current recommendations; thus, differences in pharmacotherapy were less likely to influence the outcomes. This is the first report on HFNO therapy provided by non‑ICU personnel in a larger cohort.
Limitations
We are aware of the limitations of this study. The lack of randomization and a control group significantly increased the risk of bias. The decision on intubation was not protocolized but was made by an experienced anesthesiologist and pulmonologist according to Polish guidelines, based on the SpO2/FiO2 index, respiratory distress signs, age, and comorbidity status.24 A possible bias in the assessment of ROX as a predictor of the primary outcome was the fact that even though it was not formally calculated, its components (SpO2, FiO2, and respiratory rate) were factors that were taken into account by the physician in making the decision about intubation.
Conclusions
In conclusion, our study suggests that HFNO therapy could potentially be a valuable modality in the treatment of severe hypoxemic ARF in the course of COVID‑19 in a noncritical care environment. More than half of this cohort did not reach the primary outcome defined as intubation and mechanical ventilation or death and were successfully weaned off HFNO. Yet, it must be emphasized that the prognosis for patients in whom HFNO therapy fails and mechanical ventilation is eventually required is poor. Finally, the ROX index was shown to be a useful tool in predicting patients at high risk of HFNO failure.
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID‑19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020; 323: 1239. | Crossref
- Kusza K, Kübler A, Maciejewski D, et al. Guidelines of the Polish Society of Anaesthesiology and Intensive Therapy determining principles, conditions and organisational aspects of anaesthesiology and intensive therapy services [in Polish]. Anestezjologia Intensywna Terapia. 2012; 44: 201‑212.
- Healthcare personnel statistics – physicians. Eurostat Statistics Explained website. https://ec.europa.eu/eurostat/statistics‑explained/index.php?title=Healthcare_personnel_statistics_‑_physicians#Healthcare_personnel. Accessed January 8, 2021.
- Acute Respiratory Distress Syndrome Network; Brower RG, Matthay MA, Morris A, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000; 342: 1301‑1308. | Crossref
- Arentz M, Yim E, Klaff L, et al. Characteristics and outcomes of 21 critically ill patients with COVID‑19 in Washington state. JAMA. 2020; 323: 1612‑1614. | Crossref
ARTICLE INFORMATION