Effects of cardiac rehabilitation on risk factor management and quality of life in patients with ischemic heart disease: a multicenter cross‑sectional study
Key words: cardiac rehabilitation, ischemic heart disease, propensity score matching, risk factors, secondary cardiovascular prevention



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Effects of cardiac rehabilitation on risk factor management and quality of life in patients with ischemic heart disease: a multicenter cross‑sectional study
Introduction: While cardiac rehabilitation (CR) improves survival outcomes in patients with ischemic heart disease (IHD), the long‑term benefits of short‑term programs are still discussed.
Objectives: The aim of the study was to assess the impact of CR on risk factor management in a multicenter real‑life registry of patients with IHD.
Patients and methods: We included patients aged 80 years or younger who had been hospitalized due to acute coronary syndrome or for a myocardial revascularization procedure and interviewed 6 to 18 months later. Control of risk factors was compared between patients who participated in CR and those who did not. Propensity score matching was used to account for differences in patient characteristics between the groups.
Results: Of 1012 interviewed patients (28.6% women), 35.6% were referred for CR and 76.1% of them completed the program. Those referred were younger (P <0.001), employed (P <0.001), have presented with ST‑segment elevation myocardial infarction (P <0.001), had hypertension (P <0.001), and were current smokers (P <0.001). Logistics regression revealed that patients who participated in CR were more likely to stop smoking (odds ratio [OR], 2.42; 95% CI, 1.33–4.14), achieve acceptable glucose control (OR, 1.70; 95% CI, 1.02–2.83), and better quality of life (β = 0.12; 95% CI, 0.00–0.24) compared with those who did not participate in CR.
Conclusions: Cardiac rehabilitation is moderately effective if performed only once and without a continuous support program. Further efforts to increase referrals for CR in patients with IHD must be accompanied by a long‑term strategy to sustain the beneficial effects.
What's new?
The benefits of cardiac rehabilitation (CR) programs in the management of risk factors in patients with chronic coronary syndromes is underreported in Poland. This is the first multicenter study to investigate the referral and participation patterns of CR in Poland. We found the rate of referral to CR in Poland was low, particularly in the elderly, unemployed, and in patients after elective percutaneous coronary intervention. There was a significant positive effect of CR on aspects of secondary prevention approximately 1 year after the acute coronary event or elective revascularization: smoking habit, blood glucose level, and quality of life. The observed effects may be limited by the fact that patients only participated in a single course of CR. Therefore, we suggest a single course of CR should be accompanied by a more prolonged schedule to sustain such benefits.
Introduction
Cardiac rehabilitation (CR) is one of the core elements of secondary prevention in patients with ischemic heart disease (IHD), aiming to improve risk factors, reduce hospital readmission, and produce a more favorable survival outcome. Two large meta‑analyses of 34 and 18 randomized controlled trials have shown that CR reduces recurrent cardiovascular events and improves mortality rates in patients with myocardial infarction.1,2 Moreover, CR has also been shown to improve patients’ quality of life and ability to return to work quickly.1
International guidelines recommend that all patients who have had a planned revascularization procedure or have acute coronary syndrome (ACS), chronic stable angina, or heart failure should engage in a CR program to reduce subsequent events.3,4 Moreover, recently revised practice guidelines urge for a “comprehensive rehabilitation” program covering a range of aspects: exercise training aimed at improving clinical profiles (optimization of blood pressure, lipid and glucose levels, and weight), healthy heart education (appropriate diet and smoking cessation), and psychological counseling to reduce stress and improve quality of life.3,5,6 These comprehensive efforts are intended to foster better cardiovascular risk management than could be achieved by supervised exercise alone.
In Poland, cardiovascular disease is one of the major causes of mortality, accounting for 46% of total deaths in 2010,7 with nearly half of these attributable to IHD. To address this serious situation, healthcare experts have been trying to promote a preventive approach through CR and lifestyle changes. In addition, there has been an increase in the efforts to manage care for patients with IHD, including increased access to CR programs.8 To our knowledge, there are no multicenter studies to investigate disparities in referral rates and participation in CR and the effectiveness of CR in Poland.
However, referrals for CR programs and the impact of such programs in the real world have been suboptimal9 both in Europe10 and the USA.11 A summary of a large cross‑sectional survey carried out by the pan‑European group, EUROASPIRE (European Action on Secondary and Primary Prevention by Intervention to Reduce Events), reported that CR referral rates and hence participation rates in Europe remain low.12,13 Thus, there is the need for urgent action to increase referral and enrollment rates in CR programs.
This study assessed the effectiveness of CR in a patient population enrolled in a CR program in 14 cardiology centers from 4 different regions of Poland, all of which participated in the EUROASPIRE.
Patients and methods
The POLASPIRE is a parallel program run by Polish centers involved in the EUROASPIRE V. In total, 403 patients chosen from the POLASPIRE survey contributed to the Polish subset of the EUROASPIRE V. The detailed methodology of this survey has been described previously.14,15 A multicenter cross‑sectional study was conducted between 2016 and 2017 on Polish patients from 4 geographical areas (Kraków, Katowice, Warszawa, Białystok) and from 14 cardiology departments. For each department, medical records were reviewed retrospectively of patients aged between 18 and 80 years who had been hospitalized for 1) coronary artery bypass graft surgery (CABG), 2) elective percutaneous coronary intervention (PCI), 3) acute myocardial infarction (International Classification of Diseases, Tenth Revision codes I21 and I22), or 4) unstable angina. Eligible patients were invited for an interview and follow‑up examination 6 to 18 months after being discharged. In addition to the patients from the EUROASPIRE V database, we also enrolled additional patients from participating centers during the same period, using the same methodology as well as inclusion and exclusion criteria.
All patients provided written informed consent to take part in the study. The study was approved by the local ethics committees in each regional center.
Cardiac rehabilitation management
Patients were asked to report their level of participation in CR at the time of the interview using the following options: 1) did not attend; 2) attended at least one session; 3) attended more than half of the sessions; or 4) completed all of the recommended sessions. In Poland, full participation means that patients received a comprehensive program of in‑hospital rehabilitation of between 2 to 6 weeks, which included exercise training, dietary guidance, medication review, smoking cessation advice, and stress management. Due to the design of the study and the short duration of enrollment, we only included participants in the treatment group who declared that they completed all of the CR sessions, to reliably assess the effects of CR.
Study variables
We used interviews to obtain participants’ self‑reported information on a range of health and lifestyle‑related issues, detailed below. Each patient’s body mass index (BMI) was calculated using their height and weight measured in a straight standing position without shoes and heavy items. Obesity was defined as a BMI of 30 kg/m2 or greater. A low educational level was defined as having completed only primary school level education or less. A persistent smoker was defined as a patient reported to have been a smoker in the month before the index event who was either still smoking at the time of the interview or who had levels of exhaled carbon monoxide exceeding 10 ppm. Blood pressure was measured twice on the right arm in a sitting position at 5‑minute intervals, and the mean was used for analyses. Increased blood pressure was defined as blood pressure of 140/90 mm Hg or greater. Total cholesterol, high‑density lipoprotein cholesterol (HDL‑C), low‑density lipoprotein cholesterol (LDL‑C), triglycerides, and glycated hemoglobin (HbA1c) were measured in fasting venous blood samples. An elevated LDL‑C concentration was defined as 1.8 mmol/l or greater, and HbA1c was considered acceptable if lower than 7%, as per the relevant guidelines.5 Depression and anxiety were assessed using the Hospital Anxiety and Depression Scale (HADS) with a score of less than 8 points considered normal. Quality of life was assessed using a Health‑Related Quality of Life (HRQoL) questionnaire consisting of 2 domains, physical (10 items) and emotional (4 items). Generic health status was assessed using the EQ‑5D questionnaire which comprises a 5‑dimension code describing the patient’s state of health in 5 domains, which was converted into a single index ranging from “0” (dead) to “1” (perfect health), with Germany used as the country of reference.16
Follow‑up and outcome assessment
The main outcome in this study was the achievement of risk factor management goals and self‑reported lifestyle changes at interview. The secondary outcome was interactions between CR participation and time points.
Propensity score matching method
We performed propensity score matching (PSM) to account for potential bias resulting from an imbalance in the covariate distribution between the groups that had been referred for and who participated in CR and those who were not referred and did not participate in CR, both of which could be influenced by decisions taken by physicians and patients. We used multivariable logistic regression to obtain a propensity score (PS) for each CR participant and then were able to search the database for nonreferred CR patients with the same or nearly the same PS match.17 The variables included in generating the PS were age at index event, gender, center code, type of event, education status, obesity, BMI, and smoking status.
Statistical analysis
The distribution of study variables was analyzed using the Shapiro–Wilk test, with a P value of less than 0.05 indicating normal distribution. Categorical variables were described using proportion and compared using the χ2 test. Continuous variables were expressed using mean and median values and compared using the Mann–Whitney test for data without a normal distribution and t test for variables with a normal distribution.
We used the χ2 test to compare the distribution of the baseline characteristics of patients who had been referred for CR with those not referred for CR. Multivariable logistic regression was used to identify predictors of CR participation in those referred for CR. Univariable logistic and linear regression models were constructed to estimate the effect of CR in those who participated in CR and those who did not participate from the dataset of propensity score‑matched groups.
A generalized linear model (GLM) was used, rather than a simple linear regression model, to adequately account for correlated data due to repeated measurements (pre and post) of the same study participants. This model encompassed 3 effects: 1) CR effect describing baseline difference between those who participated in CR and those who did not, 2) time effect describing interview‑baseline difference, and 3) the main effect, that is, time‑CR interaction effect, which describes whether there is a different time effect in the CR group compared with the no‑CR group and highlights the differences in outcome variables during follow‑up between the CR groups.
The multiple imputation method was used to deal with missing values (ranging from 5% to 20%). All the variables mentioned were included in the imputation model, and 10 imputation sets were then created.18,19 The imputation set was used to analyze and report study outcomes in both univariable regression model and GLM.
A 2‑tailed P value of less than 0.05, and a 95% CI for odds ratios that did not include 1, were considered statistically significant. All analyses were performed using IBM SPSS statistics software, version 25 (IBM, Armonk, New York, United States).
Results
We assessed 1012 patients who were interviewed 6 to 18 months after their index event and who had provided complete information on their participation in CR (Table 1). Of these, women accounted for less than 30% of patients. The median age of patients at the time of hospitalization was 65 years, and the majority of the patients had been hospitalized in teaching hospitals (83%). Almost 40% of the patients had been recruited following elective PCI (n = 377). Other common index events were: non–ST‑segment elevation myocardial infarction (NSTEMI) in 217 patients (21.4%), unstable angina in 215 (21.2%), and ST‑segment elevation myocardial infraction (STEMI) in 160 (15.8%) (Table 1). Overall, one‑third of patients had been referred for a CR program (35.6%), and 76.1% of these completed all the recommended sessions.
Variable | Total (n = 1012) | Cardiac rehabilitation status | P valuea | ||
Not referred (n = 652) | Referred (n = 360) | ||||
Categorical data are presented as numbers (percentages) and continuous data as medians (interquartile ranges).
a P values are reported as obtained after exclusion of missing values.
b Primary educational level denotes at most primary school level of education, higher educational level denotes completion of secondary school, high school, technical or vocational training, college, or postgraduate study.
Abbreviations: ACE, angiotensin converting enzyme; AMI, acute myocardial infarction; BMI, body mass index; CABG, coronary artery bypass graft; DBP, diastolic blood pressure; HDL‑C, high‑density lipoprotein cholesterol; LDL‑C, low‑density lipoprotein cholesterol; NSTEMI, non–ST‑segment elevation myocardial infarction; PAD, peripheral artery disease; PCI, percutaneous coronary intervention; SBP, systolic blood pressure; STEMI, ST‑segment elevation myocardial infarction; UA, unstable angina | |||||
Age at index event | 65 (60–71) | 67 (61–72) | 62 (57–68) | <0.001 | |
Center | Nonteaching hospitals | 172 (17) | 114 (17.5) | 58 (16.1) | 0.57 |
Teaching hospitals | 840 (83) | 538 (82.5) | 302 (83.9) | ||
Region | Białystok | 238 (23.5) | 75 (11.5) | 163 (45.3) | <0.001 |
Kraków | 398 (39.3) | 296 (45.4) | 102 (28.3) | ||
Katowice | 150 (14.8) | 102 (15.6) | 48 (13.3) | ||
Warsaw | 226 (22.3) | 179 (27.5) | 47 (13.1) | ||
Sex | Male | 723 (71.4) | 458 (70.2) | 265 (73.6) | 0.25 |
Female | 289 (28.6) | 194 (29.8) | 95 (26.4) | ||
Education statusb | Primary level | 125 (12.5) | 84 (12.9) | 41 (11.5) | 0.52 |
Higher level | 879 (87.5) | 565 (87.1) | 314 (88.5) | ||
Unknown | 8 | 3 | 5 | ||
Employment status | Unemployed | 663 (66.1) | 471 (72.2) | 192 (54.7) | <0.001 |
Employed | 340 (33.9) | 181 (27.8) | 159 (45.3) | ||
Unknown | 9 | 0 | 9 | ||
Index event | CABG | 43 (4.2) | 19 (2.9) | 24 (6.7) | <0.001 |
PCI | 377 (37.3) | 286 (43.9) | 91 (25.3) | ||
STEMI | 160 (15.8) | 56 (8.6) | 104 (28.9) | ||
NSTEMI | 217 (21.4) | 115 (17.6) | 102 (28.3) | ||
UA | 215 (21.2) | 176 (27.0) | 39 (10.8) | ||
Previous event | CABG | 75 (13.6) | 58 (14.2) | 17 (12) | 0.5 |
PCI | 333 (60.8) | 241 (59.2) | 92 (65.2) | 0.2 | |
AMI | 255 (47) | 195 (48.4) | 60 (43.2) | 0.28 | |
UA | 55 (10.4) | 47 (12) | 8 (5.7) | 0.03 | |
Angina pectoris | 206 (39) | 172 (44.1) | 34 (24.6) | <0.001 | |
Stroke | 58 (10.7) | 45 (11.2) | 13 (9.4) | 0.55 | |
PAD | 42 (7.8) | 33 (8.2) | 9 (6.4) | 0.49 | |
Heart failure | 40 (7.5) | 37 (9.3) | 3 (2.2) | <0.001 | |
Smoking habit | Nonsmoker | 356 (38.8) | 236 (39.5) | 120 (37.6) | <0.001 |
Former smoker | 312 (34) | 225 (37.6) | 87 (27.3) | ||
Current smoker | 249 (27.2) | 137 (22.9) | 112 (35.1) | ||
Unknown | 54 | 41 | 95 | ||
Obesity | 395 (39) | 265 (40.6) | 130 (36.1) | 0.05 | |
Weight, kg | 82.7 (74–94) | 83 (74–93) | 82.5 (74–94) | 0.86 | |
BMI, kg/m2 | 29 (26.2–32.2) | 29 (26.2–32.1) | 28.9 (26–32.6) | 0.96 | |
Diabetes | 317 (31.3) | 200 (30.7) | 117 (32.5) | 0.24 | |
Hypertension | 880 (87) | 587 (90) | 293 (81.4) | <0.001 | |
SBP, mm Hg | 136 (123–150) | 136 (123.5–150) | 135 (120.7–150) | 0.18 | |
DBP, mm Hg | 80 (72–88) | 80 (74–88) | 80 (71–88) | 0.32 | |
Hyperlipidemia | 817 (80.7) | 524 (80.4) | 293 (81.4) | 0.51 | |
LDL‑C, mmol/l | 2.4 (1.8–3.3) | 2.4 (1.7–3.2) | 2.5 (1.9–3.4) | <0.01 | |
HDL‑C, mmol/l | 1.1 (0.9–1.3) | 1.1 (0.9–1.4) | 1.1 (0.9–1.3) | 0.02 | |
Triglycerides, mmol/l | 1.3 (0.9–1.8) | 1.2 (0.9–1.8) |
| 0.38 | |
Medication prescribed | Antiplatelets | 999 (98.7) | 643 (98.6) | 356 (98.9) | 0.71 |
β-Blockers | 931 (92) | 599 (91.9) | 332 (92.2) | 0.84 | |
ACE inhibitors | 773 (76.4) | 478 (73.3) | 295 (81.9) | <0.001 | |
Statins | 960 (94.9) | 614 (94.2) | 346 (96.1) | 0.18 | |
Calcium channel blockers | 272 (26.9) | 188 (28.8) | 84 (23.3) | 0.05 | |
Diuretics | 512 (50.6) | 309 (47.4) | 203 (56.4) | <0.001 | |
Anticoagulants | 147 (14.5) | 114 (17.5) | 33 (9.2) | <0.001 | |
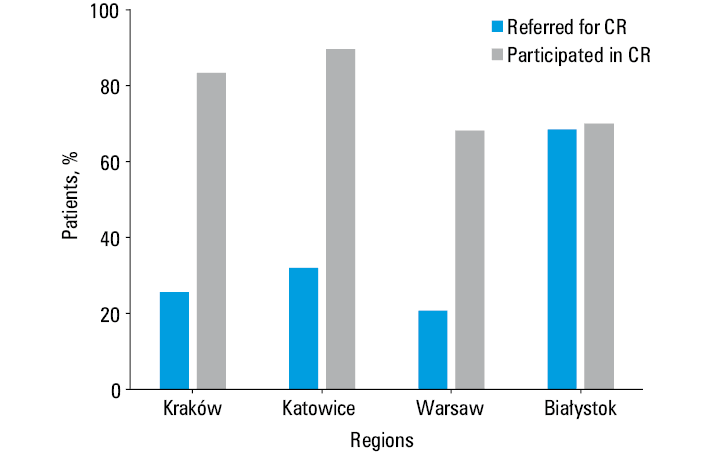
Physicians were more likely to refer younger than older patients (median [IQR] age, 62 [57–68] years vs 67 [61–72] years, respectively), and employed as compared with unemployed patients (P <0.001) to CR. The rates of CR referral and participation differed considerably between regions (Figure 1). Clinically, the patients referred were more likely to have presented with STEMI (P <0.001), CABG (P <0.001), or hypertension (P <0.001), and were more likely to be taking angiotensin‑converting enzyme (ACE) inhibitors (P <0.001), diuretics (P <0.001), and anticoagulants (P <0.001) at the time of hospital discharge. One‑third of smokers at the time of the index event (35.1%) were referred for CR (P <0.001). Among the patients referred for CR, obese patients were twice as likely to participate in CR (OR, 2.32; 95% CI, 1.07–5) than the nonobese. In addition, a higher level of education was marginally associated with CR participation (OR, 2.05; 95% CI, 0.99–4.27) (Table 2). After PSM, we revealed that patients who participated in CR were 2‑fold more likely to stop smoking (OR, 2.42; 95% CI, 1.33–4.14) and to achieve appropriate glucose control (OR, 1.70; 95% CI, 1.02–2.83) than those who did not participate in CR (Table 3). A marginal improvement was observed in the physical domain of the quality of life score in patients who participated in CR (β coefficient = 0.12; 95% CI, 0.00–0.24). Overall, there were no significant changes in lipid concentrations and systolic blood pressure during follow‑up that were affected by CR (Table 4). We further performed sensitivity analyses to examine the effects of PSM compared to conventional methods, which showed that both produced very similar results.
Variable | Overall (n = 360) | Did not participate in CR (n = 86) | Participated in CR (n = 274) | P value (group comparison) | Multivariablea OR (95% CI) | |
Categorical data are presented as numbers (percentages) and continuous data are presented as median (interquartile range).
a Multivariable model adjusted for: age at index event, center, gender, index event, education status, occupation status, smoking habit, obesity, and diabetes). Missing value was treated as “unknown” subcategory in the multivariable logistics regression model.
Abbreviations: ACS, acute coronary syndrome; CR, cardiac rehabilitation; OR, odds ratio | ||||||
Age at diagnosis, y | 62 (57–68) | 62 (58–68) | 62 (57–68) | 0.92 | 0.99 (0.96–1.03) | |
Center | Nonteaching hospitals | 58 (16.1) | 18 (20.9) | 40 (14.6) | 0.16 | 1 |
Teaching hospitals | 302 (83.9) | 68 (79.1) | 234 (85.4) | 1.7 (0.87–3.29) | ||
Sex | Female | 95 (26.4) | 19 (22.1) | 76 (27.7) | 0.3 | 1 |
Male | 265 (73.6) | 67 (77.9) | 198 (72.3) | 0.76 (0.42–1.4) | ||
Index event | Planned revascularization | 115 (31.9) | 28 (32.6) | 87 (31.8) | 0.88 | 1 |
ACS | 245 (68.1) | 58 (67.4) | 187 (68.2) | 1.02 (0.58–1.8) | ||
Education status | Primary level | 41 (11.5) | 14 (16.5) | 27 (10) | 0.1 | 1 |
Higher level | 314 (88.5) | 71 (83.5) | 243 (90) | 2.05 (0.99–4.27) | ||
Unknown | 5 | 1 | 4 | – | ||
Occupation status | Unemployed | 192 (54.7) | 45 (52.9) | 147 (55.3) | 0.7 | 1 |
Employed | 159 (45.3) | 40 (47.1) | 119 (44.7) | 0.9 (0.48–1.66) | ||
Unknown | 9 | 8 | 1 | – | ||
Smoking habit | Nonsmoker or former smoker | 207 (64.9) | 46 (63) | 161 (65.4) | 0.42 | 1 |
Current smoker | 112 (35.1) | 27 (37) | 85 (34.6) | 1.04 (0.57–1.87) | ||
Unknown | 41 | 13 | 28 | – | ||
Hypertension | No | 34 (10.4) | 10 (12.5) | 24 (9.7) | 0.47 | – |
Yes | 293 (89.6) | 70 (87.5) | 223 (90.3) | |||
Unknown | 33 | 6 | 27 | |||
Hyperlipidemia | No | 29 (9) | 6 (7.9) | 23 (9.3) | 0.69 | – |
Yes | 293 (91) | 70 (92.1) | 223 (90.7) | |||
Unknown | 38 | 10 | 28 | |||
Obesity | No | 159 (55) | 47 (67.1) | 112 (51.1) | 0.01 | 1 |
Yes | 130 (45) | 23 (32.9) | 107 (48.9) | 2.08 (1.15–3.76) | ||
Unknown | 71 | 16 | 55 | – | ||
Diabetes | No | 198 (62.9) | 46 (60.5) | 152 (63.6) | 0.62 | 1 |
Yes | 117 (37.1) | 30 (39.5) | 87 (35.4) | 0.8 (0.45–1.4) | ||
Unknown | 45 | 10 | 35 | – | ||
Variable | No CR (n = 274) | CR (n = 274)a | OR (95% CI)b | β coefficient (95% CI)c | P value |
Categorical data are presented as numbers (percentages) and continuous data are presented as median (interquartile range).
a Completed all the recommended sessions.
b Odds ratio reported for a propensity score‑matched population.
c β Coefficients reported for a propensity score‑matched population.
d For patients smoking in the month before the recruiting event.
e Patient exercise duration >20 minutes per week.
| |||||
Stopped smokingd | 31 (33) | 49 (54.4) | 2.42 (1.33–4.14) | – | <0.001 |
Physically activee | 49 (18.6) | 36 (13.7) | 0.71 (0.44–1.13) | – | 0.15 |
Body weight | |||||
BMI <25 kg/m2 | 38 (14.1) | 40 (14.8) | 1.07 (0.66–1.73) | – | 0.76 |
BMI <30 kg/m2 | 149 (55.2) | 158 (58.5) | 1.14 (0.81–1.60) | – | 0.45 |
Weight, kg | 85.8 (75.3–94.9) | 85 (75–94) | – | –0.23 (–2.79 to 2.31) | 0.85 |
BMI, kg/m2 | 29.4 (26.7–32.7) | 29 (26.4–32.5) | – | 0.32 (–0.48 to 1.12) | 0.43 |
Blood pressure | |||||
BP <140/90 mm Hg | 238 (87.8) | 237 (87.5) | 0.96 (0.57–1.61) | – | 0.89 |
SBP, mm Hg | 131 (120–146) | 130 (120–145) | – | –1.06 (–4.29 to 2.16) | 0.51 |
DBP, mm Hg | 80 (73–87) | 80 (73.5–87.5) | – | 0.49 (–1.27 to 2.26) | 0.58 |
Cholesterol control | |||||
LDL‑C <1.8 mmol/l | 109 (40.7) | 95 (35.1) | 0.78 (0.55–1.11) | – | 0.17 |
LDL‑C, mmol/l | 1.9 (1.54–2.6) | 2 (1.6–2.59) | – | 0.03 (–0.12 to 0.18) | 0.7 |
HDL‑C, mmol/l | 1.23 (1.06–1.47) | 1.24 (1.03–1.49) | – | –0.01 (–0.07 to 0.04) | 0.58 |
Triglycerides, mmol/l | 1.29 (0.95–1.79) | 1.27 (0.91–1.76) | – | –0.05 (–0.24 to 0.14) | 0.59 |
Glucose control | |||||
HbA1c <7% | 195 (81.9) | 224 (88.5) | 1.7 (1.02–2.83) | – | 0.04 |
HbA1c | 6 (5.6–6.4) | 5.8 (5.6–6.2) | – | 0.02 (–0.46 to 0.52) | 0.9 |
Medication | |||||
Antiplatelets | 250 (92.3) | 262 (95.6) | 1.83 (0.88–3.8) | – | 0.1 |
β-Blockers | 235 (86.7) | 248 (90.5) | 1.46 (0.85–2.49) | – | 0.16 |
ACE inhibitors | 192 (70.8) | 208 (75.9) | 1.29 (0.88–1.89) | – | 0.18 |
Lipid‑lowering | 241 (88.9) | 246 (89.8) | 1.09 (0.63–1.88) | – | 0.74 |
Quality of life | |||||
Anxiety HADS <8 | 8 (3) | 10 (3.8) | 1.25 (0.48–3.23) | – | 0.63 |
Depression HADS <8 | 32 (11.9) | 39 (14.7) | 1.27 (0.77–2.11) | – | 0.33 |
Emotional HRQoL | 2 (1.5–2.2) | 2 (1.5–2.2) | – | 0 (–0.09 to 0.90) | 0.94 |
Physical HRQoL | 2.2 (1.7–2.7) | 2.4 (1.8–2.8) | – | 0.12 (0–0.24) | 0.05 |
EQ‑5D QoL | 0.9 (0.8–0.9) | 0.9 (0.8–0.9) | – | 0 (–0.01 to 0.02) | 0.65 |
Parameter | No CR (n = 274) | CR (n = 274) | Interaction between CR and measurement time (95% CI) | P valuea | ||
Baseline | Interview | Baseline | Interview | |||
Categorical data are presented as numbers (percentages) and continuous data are presented as means (SD).
a P value derived from the interaction between cardiac rehabilitation and measurement time point.
b β Coefficient for continuous outcomes.
c Odds ratio for categorical outcomes.
| ||||||
Weight, kg | 85.9 (15) | 85.4 (15) | 84.9 (4.9) | 85.1 (15.3) | 0.32 (–1.58 to 2.23)b | 0.74 |
SBP, mm Hg | 139 (20) | 133 (19) | 136 (21) | 132 (18) | 1.57 (–2.6 to 5.75)b | 0.46 |
DBP, mm Hg | 82 (11) | 80 (10) | 79 (12) | 80 (10) | 3.17 (0.81–5.53)b | <0.001 |
LDL‑C, mmol/l | 2.7 (1.3) | 2.2 (1) | 2.7 (1.1) | 2.2 (0.9) | –0.02 (–0.25 to 0.2)b | 0.83 |
HDL‑C, mmol/l | 1.2 (0.4) | 1.2 (0.3) | 1.1 (0.3) | 1.2 (0.3) | 0.02 (–0.05 to 0.1)b | 0.52 |
Triglycerides, mmol/l | 1.5 (1.2) | 1.5 (1.3) | 1.5 (0.9) | 1.4 (0.9) | 0.00 (–0.2 to 0.13)b | 0.93 |
Antiplatelet agent | 268 (98.9) | 250 (92.3) | 270 (98.5) | 262 (95.6) | 2.42 (0.54–10.9)c | 0.24 |
β-Blocker | 250 (92.3) | 235 (86.7) | 253 (92.3) | 248 (90.5) | 1.44 (0.78–2.66)c | 0.24 |
ACE inhibitors | 198 (73.1) | 192 (70.8) | 227 (82.8) | 208 (75.9) | 0.72 (0.47–1.11)c | 0.14 |
Statin | 262 (96.7) | 241 (88.9) | 264 (96.4) | 246 (89.8) | 1.2 (0.44–3.29)c | 0.71 |
Discussion
We present several findings of interest regarding CR referrals in Poland. First, the rate of referrals between 2016 and 2017 was relatively low, with only 35.6% of relevant cardiac patients referred for CR. Second, there were significant disparities in CR referral rates between regions, but little or no difference between teaching and nonteaching hospitals. Third, CR was most often recommended for those with acute myocardial infarction (STEMI, 28.9% and NSTEMI, 28.3%). Obesity was a strong predictor of participation in CR. Finally, patients who participated in CR were twice as likely to quit smoking, achieve a favorable glucose concentration, and have an improved quality of life (in the physical domain) than those who did not take part in CR.
The challenge is that, despite growing evidence from meta‑analyses, systematic reviews, and multicenter studies showing that CR improves the prognosis for IHD patients in terms of reduced hospital readmissions, recurrent events, and mortality,2,20-22 there is still a low acceptance of CR overall in Poland. Our results confirm that there is a huge gap in referrals and enrollments between hospital discharge and participation in CR. Only just over one‑third (35.6%) of study patients were advised to participate in CR after their index cardiovascular event, of whom just under 77% completed full sessions: in other words, fewer than 30% of the study population completed the recommended CR sessions. These Figures on CR participation in Poland are even lower than those in both the EUROASPIRE III and IV reports covering 27 countries in Europe, which similarly showed a low proportion of patients (≤50%) being advised to take part in CR and only around one‑third doing so.12,13 These differences in participation levels could be due to the patients’ clinical profile, healthcare systems, and the accessibility of CR services in different countries.
Another finding from our study is that CR was most often assigned to patients with acute conditions, particularly those diagnosed with STEMI (65%) or NSTEMI (47%), while the referrals for those who had undergone planned PCI were lower (24.1%). In contrast, a study from the USA using data from the ACTION‑Get registry showed that about 50% of patients were referred for CR overall, with enrollment rates of 84.5% for patients with STEMI, 75.9% for those with NSTEMI, and 60% for those having undergone PCI.23
In summary, there are significant disparities in the levels of CR referral and participation between the USA, Europe, and specifically Poland. What is not clear is whether these low referral and participation rates are due to low physician awareness of the benefits of CR, limited access to CR facilities, patients declining to participate, or a combination thereof. The fact that CR services after ACS or PCI are covered by the public healthcare system in Poland8 makes it all the more surprising that CR has been so underused. One possible explanation is that, as one of the fastest‑aging societies in the EU with 5.9 million people aged 65 years and older,7 basic healthcare facilities and hospitals may face problems in managing these large numbers of patients and the costs of treatment involved. As a consequence, hospitals may try to keep the number of admissions and basic health care referrals to a minimum, and prioritize those most in need.7 Also, there is evidence that poor uptake of CR may be due to the reluctance of physicians to refer patients, lack of CR facilities, and / or lack of funding.1,23,24 In Poland, this was the motivation for the introduction of a country‑wide program of managed care after myocardial infarction, including compulsory CR programs.5 The hope is that this program will improve communication between physicians and patients, which in turn may improve the uptake of CR as well as optimize secondary prevention.
Further noteworthy observations from our study are that younger, employed, smoking patients, and those on ACE inhibitors were more likely to be advised to take part in CR. Advising patients in employment to participate in CR makes sense since CR can help cardiac patients to improve their condition and quality of life to a point where they can go back to work. Concerning age, physicians are perhaps less inclined to refer the elderly for CR due to frailty and possible difficulties they might face in commuting to the hospital.5,25 To reduce these age‑related disparities, alternative approaches such as home‑based CR for elderly and frail patients should be considered and ideally included in a country‑wide program.26
Our findings show that more than half of the patients participating in CR were smokers, which is consistent with the results of the EUROASPIRE IV (OR, 1.48; 95% CI, 1.25–1.74). Moreover, those participating in CR were more than twice as likely to give up smoking than nonparticipants. There is previous evidence from landmark trials that smoking may even outweigh the beneficial effects of statins. These studies showed that the risk of mortality observed in nonsmokers not receiving statins was similar to that of smokers on statins.27 Our results and those of others13 showing the beneficial impact of CR programs performed in individuals quitting smoking could help boost efforts to encourage more persistent smokers to participate in CR and attend sessions regularly.
Our study confirms positive effects of CR. It showed an approximately 2‑fold reduction of average blood glucose levels (HbA1c <7%) in those taking part and completing all the sessions. Moreover, patients who participated in CR showed marginal increases in HRQoL in at least 1 domain. This finding is similar to 2 earlier observational studies that reported significant improvements in quality of life at 6‑month28 and 1‑year29 follow‑up. However, neither of these studies adjusted for confounding factors, unlike our study, which applied comprehensive adjustments through the PSM method. Our results therefore provide substantial novel evidence to confirm these findings. However, the observed effects on the attainment of secondary prevention targets are still smaller than expected. We need to search for innovative strategies to improve and sustain the beneficial effects of CR.30
This study is subject to several limitations. The main one is potential recall bias, given that the bulk of data on CR participation and its effects was obtained from patients’ self‑reported questionnaires. Another limitation is that patients volunteered to participate in the study, so individuals more concerned about their health might have been more likely to participate. Finally, since the data was gathered in Poland, the results may not be representative of all countries.
Nonetheless, our findings contribute to the evidence supporting the introduction of the managed healthcare policy for patients with IHD in Poland, which aims to increase CR uptake and participation rates in Poland as well as involving multidisciplinary teams (physicians, nurses, exercise scientists, nutritionists, and psychologists) to improve the prognosis of patients with IHD.8,21 Our statistical approach, using the PSM method to control confounding variables as well as systematically dealing with missing values using multiple imputations, greatly enhances the statistical power and strength of the study findings, notwithstanding the modest size of the sample groups.
Conclusions
The present study showed that a relatively small number of patients with IHD are referred for CR in Poland. Most patients had an improved lifestyle after participation in CR, with the main identified long‑term benefits being an increase in the rates of those giving up smoking and a better quality of life score in the physical domain. Our findings point to an urgent need to incorporate CR into optimized long‑term care programs to help sustain the benefits for patients with IHD.
- Lawler PR, Filion KB, Eisenbery MJ. Efficacy of exercise‑based cardiac rehabilitation post‑myocardial infarction: a systematic review and meta‑analysis of randomized controlled trials. Am Heart J. 2011; 162: 571‑584.e2. | Crossref
- van HG, Deckers J, Tay HY, et al. Lessons from contemporary trials of cardiovascular prevention and rehabilitation: a systematic review and meta‑analysis. Int J Cardiol. 2017; 232: 294‑303. | Crossref
- Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016; 37: 2315‑2381.
- Smith SC, Benjamin EJ, Bonow RO, et al. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation endorsed by the World Heart Federation and the Preventive Cardiovascular Nurses Association. J Am Coll Cardiol. 2011; 58: 2432‑2446. | Crossref
- Piepoli MF, Corra U, Adamopoulos S, et al. Secondary prevention in the clinical management of patients with cardiovascular diseases. Core components, standards and outcome measures for referral and delivery: a policy statement from the cardiac rehabilitation section of the European Association for Cardiovascular Prevention & Rehabilitation. Endorsed by the Committee for Practice Guidelines of the European Society of Cardiology. Eur J Prev Cardiol. 2014; 21: 664‑681.
ARTICLE INFORMATION