Tuberculosis diagnosed by thoracic surgeons
Key words: radiological evaluation, thoracic surgery, tuberculosis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Tuberculosis diagnosed by thoracic surgeons
Introduction: Tuberculosis is frequently omitted in the diagnostic workup and may be identified accidentally following thoracic surgeries, mostly those targeting lung cancer.
Objectives: This study aimed to assess the clinical characteristics of patients who underwent thoracic surgery that resulted in the diagnosis of tuberculosis and to review lesions initially found on chest imaging in the context of the potential presence of tuberculosis.
Patients and methods: We analyzed medical records of all patients hospitalized at the Department of Thoracic Surgery of the National Tuberculosis and Lung Diseases Research Institute, Warsaw, Poland, between the years 2014 and 2018 (n = 57) in whom tuberculosis was diagnosed. Two radiologists who knew the diagnosis retrospectively analyzed preprocedural chest computed tomography scans of the study patients.
Results: Tuberculosis was diagnosed by culture of specimens obtained during video‑assisted thoracoscopy (21 patients), thoracotomy (24 patients), mediastinoscopy (6 patients), transthoracic fine‑needle biopsy (3 patients), and transbronchial biopsy (1 patient). In the remaining 2 individuals, the diagnosis was established based on the microbiological examination of drained pleural fluid. In 42 patients (73.7%), the diagnosis of tuberculosis was unexpected to thoracic surgeons. Radiological findings suggestive of tuberculosis were present in 38 patients (66.7%). The radiologists who retrospectively analyzed the imaging records suggested tuberculosis in 31 persons (54.3%), whereas those who carried out the initial preprocedural evaluation, in 11 (19.3%).
Conclusions: The majority of the study patients presented with radiological findings encountered in tuberculosis, which should have led to a less invasive diagnostic workup. This highlights the role of radiologists in the identification of the disease.
What's new?
In countries with a low incidence of tuberculosis, including Poland, the disease has been relegated to the background. Therefore, it is frequently ignored in the diagnostic workup and identified accidentally, particularly during thoracic surgeries for lung cancer. Symptoms and radiological findings associated with pulmonary tuberculosis are nonspecific and do not confirm the diagnosis. Radiologists play an important role before surgical intervention, as they may identify the potential presence of tuberculosis, which allows physicians to diagnose the disease using less invasive methods. In this study, we reviewed medical records of all patients with tuberculosis who were hospitalized at the Department of Thoracic Surgery in the years 2014 to 2018 and retrospectively analyzed their preprocedural computed tomography scans. Our findings emphasize the significance of considering tuberculosis in the differential diagnosis of pulmonary disease and point out the need for proper interdisciplinary communication.
Introduction
Tuberculosis is an infectious disease caused by the Mycobacterium tuberculosis complex. Its incidence in Poland is higher than in the majority of the European Union and European Economic Area countries—in which it does not exceed 10 cases per 100 000 population—but it is several times lower than in the 1980s and 1990s, not to mention the tragic epidemiological situation after World War II.1,2
In 2019, 5075 cases of pulmonary tuberculosis were diagnosed in Poland, and the incidence was 13.2 per 100 000 population. Ten years earlier, there were 6992 cases of the disease, and the incidence was 18.3 per 100 000 population. In the last 30 years, the incidence of lung cancer has been higher than 50 cases per 100 000 population. In 2017, the incidence of lung cancer was 56.1 per 100 000 population. A total of 13 798 men and 7747 women developed the disease, and the mortality rate of this malignancy in Poland was 46.8‑fold higher than that of tuberculosis.2,3
In clinical practice, general practitioners and the majority of pulmonologists more frequently meet patients with lung cancer than with tuberculosis. Therefore, tuberculosis has become a disease of somewhat less significance, often not even considered in the diagnostic workup. Cough, which is the most frequent symptom of pulmonary tuberculosis, occurs in numerous diseases of the respiratory system. Systemic manifestations of tuberculosis, such as weight loss and night sweats, are nonspecific for the disease either.4
Tuberculosis should be considered if risk factors for disease reactivation are noted. These include impaired immunity, diabetes, malnutrition, cigarette smoking, and alcohol abuse.5 Features seen on imaging are nonspecific for tuberculosis and do not confirm the diagnosis; however, they may be characteristic enough to suggest the disease. A definitive diagnosis of tuberculosis is established exclusively after microbiological testing confirming the presence of the M. tuberculosis complex in a sample. The most frequently analyzed materials include sputum, bronchial washings, bronchoalveolar lavage fluid, and lung biopsy specimens obtained during fiberoptic bronchoscopy. In patients suspected of tuberculosis with mediastinal and hilar lymph node involvement, diagnosis may be reached through endobronchial ultrasound–guided transbronchial needle aspiration (EBUS‑TBNA) or transesophageal endoscopic ultrasound–guided needle aspiration.6 According to the current recommendations, each sample should undergo molecular testing for the presence of the M. tuberculosis complex.4 The rapid Xpert MTB/RIF test (Cepheid, Sunnyvale, California, United States) allows clinicians to detect the genetic material of the bacilli within 2 hours.
Furthermore, surgical procedures are performed in some patients suspected of tuberculosis in whom the diagnosis has not been established with less invasive methods. However, tuberculosis identified as a result of thoracic surgery usually comes as a surprise.7 In the era of low‑dose computed tomography (CT), tuberculosis may also be detected accidentally in individuals screened for lung cancer—nodules first suspected to be malignant, when removed surgically, turn out to be tuberculomas.8,9
This study aimed to investigate whether the clinical presentation of the disease, risk factors, and, most importantly, lesions initially found on chest CT of patients in whom tuberculosis was diagnosed as a result of thoracic surgery may have indicated the disease earlier and whether radiologists reported such a suspicion.
Patients and methods
The study was approved by the Bioethics Committee at the National Tuberculosis and Lung Diseases Research Institute (KB‑76/2020) and involved the analysis of medical records of patients hospitalized at the Department of Thoracic Surgery between the years 2014 and 2018 in whom tuberculosis was diagnosed by culture. This paper is based on descriptive analysis. We reviewed records entered in the microbiological registries maintained by the Department of Microbiology of the Institute pertaining to all patients of the Department of Thoracic Surgery in whom culture results for the M. tuberculosis complex were positive and who also underwent molecular testing and bacterioscopy to detect acid‑fast bacilli. We collected data on patients’ age, sex, symptoms indicating a possibility of tuberculosis (cough, fever, and weight loss), body mass index, cigarette smoking status, results of the interferon-γ release assay, factors increasing the risk of tuberculosis reactivation (diabetes, immunosuppression, and malnutrition), and surgical procedures resulting in the diagnosis of tuberculosis. Data were obtained on the basis of histological or cytologic examinations of samples (from the lung, pleura, mediastinal and hilar lymph nodes, and pleural fluid) and lesions found on bronchoscopy. Two radiologists who knew the diagnosis retrospectively assessed the chest CT scans, searching for lesions suggestive of tuberculosis (Table 1). When CT scans were not available, chest radiographs were analyzed instead. In each case, it was noted whether the radiologist who read the chest images prior to surgical intervention indicated a possibility of tuberculosis. Thoracic surgeons identified patients in whom the diagnosis of tuberculosis following surgery was unexpected.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ii. Loculated fluid |
iii. Signs of pleural empyema |
|
|
|
Results
The study group included 57 patients in whom thoracic surgeries led to the diagnosis of tuberculosis; in the same time frame, the total number of thoracic surgeries performed at the Department was 11 033. The analyzed group included 30 men (52.6%) and 27 women (47.4%). The mean and median age of the patients was 50.5 and 50 years, respectively (range, 23–84 years). Cough was reported in 14 patients (24.6%), fever in 10 (17.5%), and weight loss in 12 (21.1%). Information about symptoms of the remaining persons was not available. Six patients (10.5%) were treated for diabetes and 11 (19.3%) had a body mass index below 20 kg/m2. According to the available data, 10 individuals (17.5%) smoked cigarettes and 10 (17.5%) underwent immunosuppressive treatment. The results of the interferon-γ release assay were available in 3 patients and were positive in all cases. Fiberoptic bronchoscopy prior to surgical intervention was performed in 33 patients (57.9%), and in 9 (15.8%), lesions indicating previous tuberculosis (scars from lymph node–bronchial fistulas and anthracotic incrustations) were found.
A total of 21 study patients underwent video‑assisted thoracoscopy (VATS); in 9 persons, it was combined with marginal or wedge resection of the lung. In 9 patients, marginal or wedge resection was performed using thoracotomy. Six individuals underwent lobectomy with lymphadenectomy. Tuberculosis was also identified in 2 patients who were operated on because of emphysematous bullae. A single person with confirmed mesothelioma of the pleura underwent pleurectomy and lymphadenectomy and had tuberculosis diagnosed following the examination of pleural fluid. In another person with pleural empyema, fenestration of the chest wall was initially performed and followed by pneumonectomy and thoracoplasty. Decortication was carried out in 3 individuals. Right‑sided resection of the third rib, without decortication, was performed in a patient with pleural empyema penetrating to the rib. A single HIV‑infected person with perforation of the esophagus due to inflammation of enlarged mediastinal lymph nodes underwent thoracotomy and suturing of the perforation. Mediastinoscopy was carried out in 6 patients.
In 3 patients, tuberculosis was diagnosed by transthoracic fine‑needle biopsy, and in a single person, by transbronchial biopsy. Planned VATS was abandoned in 2 individuals with pleural effusion and the intervention was limited to inserting a drain into the pleural cavity. In one of those individuals—a man aged 84 years, in severe general condition—bacilli resistant to isoniazid and rifampicin were cultured from pleural exudate. Six persons (10.5%) from the study group underwent EBUS, but it had not led to the diagnosis of tuberculosis.
Postprocedural complications occurred in 9 patients. A transient decrease in arterial oxygen saturation of up to 83% was observed in a patient after thoracotomy and excision of emphysematous bullae. The accumulation of secretion in the respiratory tract that required bronchoaspiration was noted in 2 study patients (one person after resection of emphysematous bullae and another one after decortication). Fever on the first day following the surgery was reported in a single patient after VATS, and temporary cardiac arrhythmia, in a single person after VATS combined with marginal resection. Three patients needed prolonged pleural drainage because of air or fluid leakage in the pleural cavity (after thoracotomy with resection, VATS with resection, and drain insertion). A single woman after decortication due to pleural empyema developed respiratory failure requiring mechanical ventilation.
Histological examination was carried out in 51 patients (89.5%) and explicitly indicated tuberculosis in 44 individuals (77.2%). Granulomas represented the main morphological feature detected during the microscopic examination of the samples obtained from patients with tuberculosis. Granulomas are made up of epithelial cells corresponding to macrophages modified by cytokines, multinucleated giant cells—the so‑called Langhans cells that are formed as a result of aggregation of several macrophages, and accompanying inflammatory infiltrate including lymphoid cells. Granulomas occur individually or as an aggregate that forms larger conglomerates (nodules). They may be accompanied by necrosis of varying extent or become fibrous.10-13
Mycobacteria accumulated in the necrotized region and in the foci of softening and calcification may be detected by additional tests, mainly Ziehl–Neelsen staining. However, the absence of bacteria on staining does not exclude tuberculosis. To confirm infection suggested by pathomorphological characteristics, it is necessary to perform a microbiological analysis.
ProbTec (Probe Tec Becton, Dickinson and Company, Sparks, Maryland, United States) or Xpert MTB/RIF molecular testing of the material collected during the procedure was conducted in 29 patients (50.9%) and yielded positive results in 24 (42.1%). Bacterioscopy of the obtained specimens was performed in 55 patients (96.5%), and the result was positive in 22 persons (38.6%).
The diagnosis of tuberculosis in 42 patients (73.7%) surprised thoracic surgeons; however, it was expected in the remaining 15 patients (26.3%). The surgeons considered the potential presence of tuberculosis in 5 individuals with pleural effusion, including a single person with accompanying parenchymal consolidations, in whom the radiologist who had examined the patient prior to surgical intervention suggested the possibility of tuberculosis, although lung cancer was also taken into account. The diagnosis of tuberculosis did not astonish clinicians in the case of 4 patients with empyema either; radiologists who participated in the examination suggested the disease in 3 of them. Thoracic surgeons, but not radiologists, also suspected tuberculosis in a patient with multiple pulmonary nodules, accompanying fibrotic lesions, and the tree‑in‑bud sign; in 2 individuals with pulmonary nodules who had undergone antitubercular therapy; in a patient with unilateral parenchymal consolidations with cavitation, the tree‑in‑bud sign, and a radiological suggestion of tuberculosis; in a patient with a nodule in the middle lobe; and in an individual with a nodule in the third segment of the right lung (the latter 2 patients had lesions on fiberoptic bronchoscopy: anthracotic incrustations and scarring after lymph node–bronchial fistulas). The radiologist who carried out the initial assessment of the lesions prior to surgical intervention did not point to the presence of tuberculosis in any of these 2 patients.
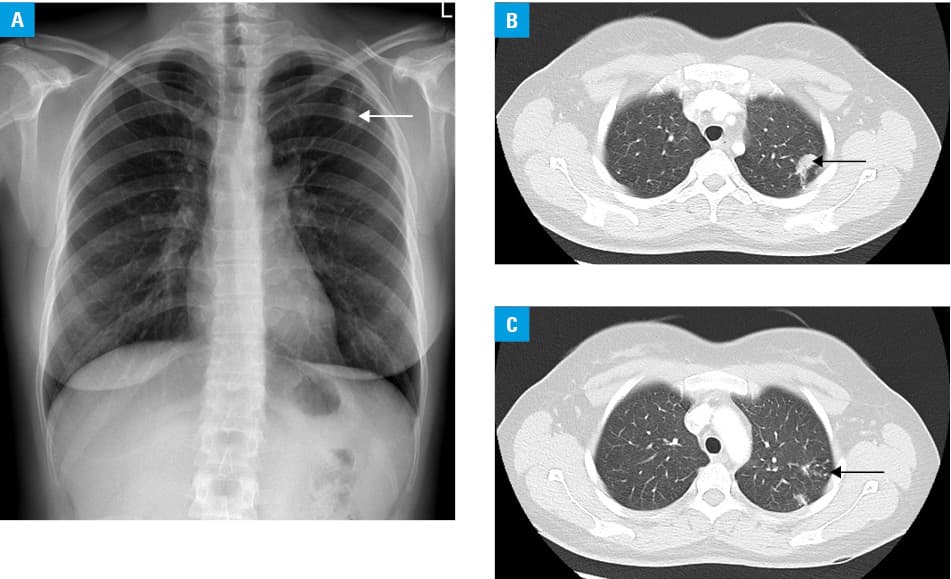
Computed tomography was performed in 50 patients (87.7%) (including 7 individuals in whom only descriptions of CT scans from the healthcare center that had referred them to the Institute were available). In the remaining 7 persons, the radiologists participating in the study based their evaluation on chest radiographs. Parenchymal consolidations were detected in 12 patients (21%): unilateral in 10 persons and bilateral in 2; with features of necrosis in 6 cases (Supplementary material, Figure S1) and located bilaterally in 2 individuals. In 3 patients, consolidations were found in the apex of the left lung, and in 4, in the right one. In 6 cases, consolidations were located in the posterior segment of the right upper lobe, and in other 6, in the apical segment of the right lower lobe. A total of 32 patients had nodules of location typical of tuberculosis: in 5 patients, a solitary nodule was identified, and in 27, multiple nodules were found. None of the study patients had miliary lesions. In 4 persons, features of necrosis were noted in nodules; in a single individual, a distinct thick‑walled cavity was detected on CT (Supplementary material, Figure S1); and 12 patients had calcification. In 11 patients, the tree‑in bud sign was apparent (Figure 1). Fibrotic lesions were found in 18 patients (31.6%) (Supplementary material, Figure S2).
Mediastinal and hilar lymphadenopathy was detected in 12 individuals; in 8 cases, it affected right lower paratracheal lymph nodes (station 4R). In 8 patients with adenopathy, tuberculosis was diagnosed after the examination of specimens from the lymph node; in 3, from the lung; and in 1, from plural fluid. An enhancement pattern typical of tuberculosis was not found on CT in any case. Calcification of lymph nodes was detected in 3 individuals. None of the 12 patients could be considered to have primary tuberculosis, as some lesions indicated previous tuberculosis.
Pleural lesions were noted in 24 patients (42.1%); thickening (also irregular) and calcification, in 13 (22.8%); and lesions suggestive of pleural effusion, in 19 (33.3%)—in 9 persons the fluid was free; in 6, loculated; and in 4, it had features of empyema.
Radiological findings that could have indicated tuberculosis were reported in 38 patients (66.7%); in 32 patients, they were of complex nature (Table 2) and occurred in various constellations (Supplementary material, Figure S3), and in 6, they were of a single type (Table 3). According to the radiologists participating in the study, imaging was suggestive of tuberculosis in 31 patients (54.3% of the study group); the radiologists who did not know the diagnosis postulated such diagnosis in their interpretations prior to thoracic surgery in 11 patients (19.3%). The opinions of the radiologists assessing the examinations prior to surgical procedures corresponded with those of the radiologists participating in the study in 10 cases; in a single patient, a radiologist initially suggested tuberculosis and such possibility was not considered by the radiologists who took part in the analysis.
Lesions | Patients, n | Possibility of tuberculosis suggested by the radiologists participating in the study | Possibility of tuberculosis suggested by the radiologists initially reading the images |
Multiple nodules and scars and the tree‑in‑bud sign | 3 | 3 | 2 |
Multiple nodules and scars with / without cavitation in the nodules | 2 | 1 | 0 |
Multiple nodules and adenopathy in station 4R with / without scars, with / without calcification in the nodules, with / without cavitation in the nodules | 5 | 3 | 0 |
Multiple nodules with cavitation and lymphadenopathy (not in station 4R) | 1 | 0 | 0 |
Unilateral consolidation with cavitation and multiple nodules with / without cavitation, with / without calcification, with / without pleural thickening | 3 | 2 | 1 |
Unilateral consolidation with cavitation and multiple nodules with / without pleural thickening and the tree‑in‑bud sign | 2 | 2 | 2 |
Unilateral consolidation without cavitation and nodules and pleural thickening or scars | 2 | 2 | 0 |
Unilateral consolidation without cavitation and nodules with calcification and free pleural effusion | 1 | 1 | 1 |
Unilateral consolidation without cavitation and nodules and the tree‑in‑bud sign | 1 | 1 | 1 |
Bilateral consolidations with cavitation and multiple nodules and scars and pleural thickening and the tree‑in‑bud sign | 1 | 1 | 1 |
Bilateral consolidations with cavitation and free pleural effusion | 1 | 1 | 1 |
Solitary nodule with calcification and the tree‑in‑bud sign | 1 | 1 | 0 |
Solitary nodule and free pleural effusion | 1 | 0 | 0 |
Solitary nodule with calcification and adenopathy in station 4R with calcification and scars and pleural thickening | 1 | 1 | 0 |
Free pleural effusion with / without scars and the tree‑in‑bud sign | 2 | 2 | 0 |
Free pleural effusion with irregular pleural thickening | 1 | 0 | 1 |
Single cavity of location typical of tuberculosis and multiple nodules | 1 | 1 | 1 |
Pleural empyema and scars and pleural thickening with / without the tree‑in‑bud sign | 2 | 2 | 0 |
Fluid in the pericardium and pleura, consolidation in segment 3 of the left lung | 1 | 1 | 0 |
Lesions | Patients, n | Possibility of tuberculosis suggested by the radiologists participating in the study | Possibility of tuberculosis suggested by the radiologists initially reading the images |
Loculated pleural effusion | 2 | 2 | 0 |
Solitary nodule in the posterior segment of the right upper lobe | 1 | 1 | 0 |
Parenchymal consolidation in the apical segment of the lower lobe | 1 | 1 | 0 |
Satellite nodules (a single bigger nodule surrounded by several smaller ones) in the apical segment of the lower lobe | 1 | 1 | 0 |
Pleural empyema | 1 | 1 | 0 |
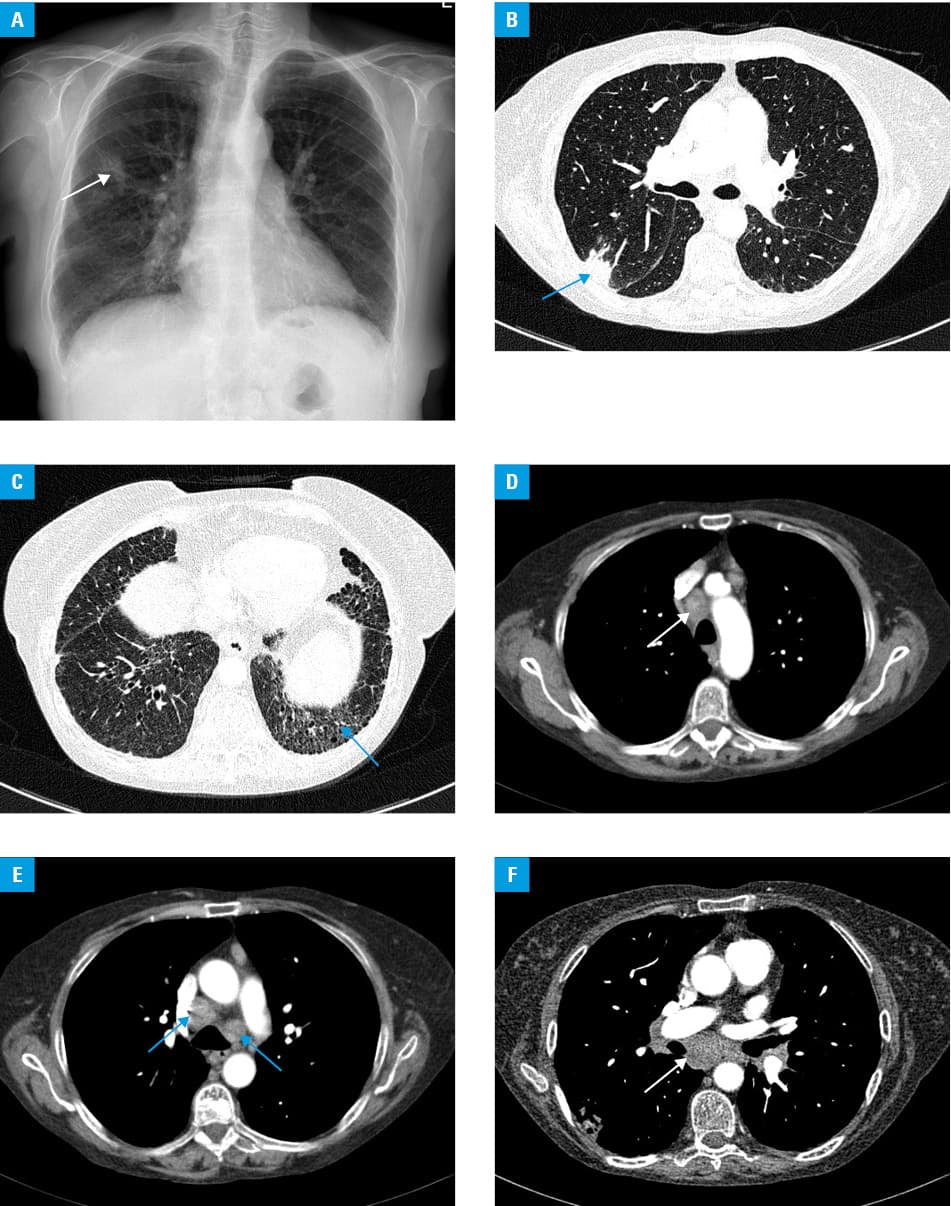
In 7 patients with lesions that could be indicative of tuberculosis, the radiologists participating in the study did not find sufficient reasons for suggesting the disease owing to other concomitant findings (occasionally dominant), nonspecific for tuberculosis. In 3 of those patients, enlargement of mediastinal lymph nodes of various stations was seen, including station 4R; in another patient, isolated enlargement of this lymph node station was observed. The radiologists participating in the study did not consider tuberculosis in those individuals because of premises listed below. One case concerned a woman with identified and treated lymphoma, in whom lymphadenopathy affected multiple lymph node stations. The patient also had newly developed lesions—subpleural foci of parenchymal consolidations with morphologic features of organizing pneumonia and reticular opacities in the basal regions of the lungs, indicative of interstitial fibrosis. Tuberculosis was diagnosed by the examination of lung specimens obtained from lesions suggestive of organizing pneumonia and from subcarinal lymph nodes (other lymph nodes were not examined) (Figure 2). Sarcoidosis was suggested in another woman in whom mediastinal and left hilar lymphadenopathy and parahilar nodular dissemination were identified (tuberculosis was diagnosed by lymph node specimen examination) (Supplementary material, Figure S4). In the third case, a solid nodule in segment 8 as well as scars and calcified nodules in the apexes and middle lobe were found. Furthermore, positron emission tomography with CT (PET‑CT) showed an increased metabolic activity of mediastinal lymph nodes. Samples collected from the lymph nodes during mediastinoscopy confirmed the diagnosis of tuberculosis. Subsequently, right lower lobectomy with lymphadenectomy was carried out and the nodule in segment 8 turned out to be carcinoid (Supplementary material, Figure S3). The fourth patient had prominent features of isolated lymphadenopathy—station 4R (interpretation of the CT scan from outside the Institute), based on which the diagnosis of tuberculosis was established (Supplementary material, Figure S2). The patient also had fibrotic lesions in the lingula and segment 8.
One of the 7 abovementioned patients had a solitary nodule surrounded by small satellite nodules; and 2 others had multiple nodules with and without cavitation, respectively. Free pleural fluid accompanied by irregular pleural thickening and calcification was found in a single patient (the radiologist who performed the initial interpretation of the image suggested tuberculosis).
Discussion
Tuberculosis may be detected as a result of thoracic surgery; however, in such situations, as in the present study, the diagnosis is often unexpected. In countries with a low prevalence of tuberculosis, the disease is not usually suspected to be the cause of lesions in the chest prior to the procedure.7
Pulmonologists who referred our study patients to thoracic surgeons were probably convinced that malignancy accounted for the abnormalities found on imaging. This could be partially a consequence of the fact that the radiologists who described the initial images rarely indicated tuberculosis in differential diagnosis, although otherwise they recognized lesions typical of tuberculosis. Presumably, in some cases, radiological suggestions would facilitate the diagnosis of tuberculosis without surgical intervention. This emphasizes the need for proper interdisciplinary communication of all professionals involved in the diagnostic workup.
Nowadays, rapid molecular tests are available, which do not require a waiting period of several weeks for culture of the M. tuberculosis complex and allow clinicians to eliminate the risk of late diagnosis in the case of cancer. The Xpert MTB/RIF or Xpert MTB/RIF Ultra test detects the genetic material of the M. tuberculosis complex after 2 hours. Testing positive confirms tuberculosis in patients with a positive result of sputum bacterioscopy or significantly increases its probability in those with negative smears.14 In addition, if the radiologist does not suggest that the detected abnormalities may indicate tuberculosis, isolation of infectious patients is delayed, leading to disease transmission.15 However, features considered typical of tuberculosis are not always present on imaging (they were found in 19 of our study patients [33.3%]) and they may mimic malignancy. Moreover, tuberculosis and lung cancer may coexist (even in the same lesion).7,16 In our study, there was a single patient in whom both tuberculosis and lung cancer (carcinoid) were found.
Tuberculosis with mediastinal lymph node involvement may be detected by EBUS‑TBNA.17 The Xpert MTB/RIF test of a sample obtained during EBUS‑TBNA increases the possibility of disease identification.6 The diagnosis of mediastinal lymphadenopathy is also possible using another method, that is, endobronchial ultrasound with endoscopic ultrasound–guided fine‑needle aspiration.18
Before the introduction of less invasive methods, lymphadenopathy was diagnosed by mediastinoscopy.19 Currently, VATS is a modality commonly used to diagnose and treat pulmonary diseases and intrathoracic lesions. It is considered safe, as no deaths or complications were reported in 26 individuals with pleural effusion, including 30.8% with tuberculosis.20 The method was also frequently used in the diagnostic workup of our study patients. Invasive methods for the diagnosis of tuberculosis have a high sensitivity. Histological analysis along with culture of pleural specimens obtained during thoracoscopy were demonstrated to have 100% sensitivity.21
Imaging may indicate tuberculosis and direct further diagnostic evaluation. Chest radiography often enables the detection of tuberculous lesions (Supplementary material, Figure S5). However, the specificity of a chest radiograph in the diagnosis of tuberculosis is limited. The diagnostic efficacy of CT in the detection of tuberculosis is considerable; its sensitivity reaches 91%, and specificity, 76%. High‑resolution CT shows lesions that are not visualized on a radiograph, that is, small nodules, small cavities, and ill‑defined parenchymal opacities, and enables a thorough assessment of the type and distribution of lesions. It is a useful tool in the imaging of mediastinal and hilar lymph nodes.22 Another modality, PET‑CT, uses hybrid devices—a CT scanner and a PET gamma camera—which enables a fusion of morphological and scintigraphic imaging, with fluorine‑18 fluorodeoxyglucose as a tracer. Active tuberculous lesions are characterized by an increased tracer uptake, but it is difficult to differentiate between active tuberculosis and cancer. Based on PET‑CT, tuberculous lesions cannot be distinguished from other infectious inflammatory or granulomatous processes, such as sarcoidosis.7,23,24 As far as our study group is concerned, PET‑CT was not useful for the diagnosis of tuberculosis.
There are 2 distinctive imaging patterns in pulmonary tuberculosis. In primary tuberculosis, mediastinal and hilar lymphadenopathy and homogenous parenchymal consolidation—the Ghon primary focus (sometimes multiple foci), with no remarkable predilection for the defined regions, are observed. Mediastinal and hilar lymphadenopathy in primary tuberculosis occurs more frequently in pediatric patients. Among the middle‑aged and elderly, primary tuberculosis and the associated adenopathy are not reported so frequently. Persons with impaired immunity may more often have adenopathy even in postprimary tuberculosis. Lymphadenopathy is more frequently unilateral, with a predilection for the right side. It often occurs in the paratracheal region, particularly in lower right paratracheal lymph nodes (station 4R) and the hilum. Computed tomography following intravenous contrast administration may show a lymph node pattern typical of active tuberculosis—hypodense lesions due to central necrosis, with intensive enhancement of the peripheral rim (this feature is particularly observed in the case of nodes with a diameter larger than 2 cm).25-27 On the other hand, calcification of lymph nodes is markedly more frequent in nonactive tuberculosis.28 Lymphadenopathy may also occur, although less often, in postprimary tuberculosis. Mediastinal and hilar lymphadenopathy was identified on CT in 31% of patients with primary tuberculosis and in 17% of individuals with postprimary disease.29 In our study group, lymphadenopathy always coexisted with lesions indicating previous tuberculosis, which indicated the postprimary form of the disease.
In postprimary tuberculosis, following the reactivation of an earlier infection with M. tuberculosis, the initial stage is characterized by focal or patchy parenchymal opacities in apical and posterior locations. Lesions are generally bilateral and usually more than one lung segment is affected. Cavities in the area of consolidation are commonly seen in tuberculosis. They can be single or multiple and usually have thick, irregular walls.23,30
In about 5% of cases, tuberculosis involving the lung parenchyma manifests as tuberculoma—a round or oval nodular opacity (rarely multiple) of 0.5 to 4 cm in diameter, usually well circumscribed (occasionally with spiculated margins), often nonenhanced after intravenous contrast administration, and sometimes surrounded by satellite nodules.31,32
Active tuberculosis may also present with poorly defined centrilobular nodules with branching linear opacities suggestive of lesions in the bronchioles. The tree‑in‑bud sign, although remarkable, is nonspecific for tuberculosis. It may appear in mycobacteriosis, bronchiolitis caused by other pathogens, lymphoma, and adenocarcinoma of the lung.22,30-34
Miliary tuberculosis occurs in primary and postprimary disease and indicates the hematogenous spread of tuberculosis. In this type of the disease, CT demonstrates small, disseminated, well‑defined nodules (1–3 mm) of uniform random distribution.30
Tuberculous pleural effusion is generally unilateral; in postprimary tuberculosis, it typically coexists with parenchymal lesions, whereas in primary disease, it may be the only imaging finding. The enhancement of the pleura, a split sign on CT, may indicate the presence of empyema.27,35,36
Calcified Ghon foci and apical nodules are typical of previous primary tuberculosis. They represent a residue of the Simon foci developed during hematogenous dissemination of primary tuberculosis. Calcification may be seen in the pleura, pericardium, and lymph nodes.28,37
Tuberculous lesions can also heal through fibrosis—it was noted on follow‑up radiography of approximately 40% of the cured persons. Fibrosis may manifest as scarring parenchymal fibrotic lesions, apical pleural thickening, bronchiectasis, distortion of the lung architecture: lung volume reduction, hilar retraction, and mediastinal shift toward the affected lung. Pleural thickening, pleural calcification, and fibrothorax constitute residual features of inflammatory exudate.37,38 Patients with lesions indicative of previous tuberculosis who develop new abnormalities should be screened for tuberculosis, as they may have a relapse.15
The implementation of radiomics enables advanced quantitative analysis of images, which can increase diagnostic accuracy and facilitate the decision‑making process, also in terms of differentiating between lung cancer and tuberculosis on CT and PET‑CT.39,40 Screening programs using low‑dose CT improve early detection of lung cancer in high‑risk populations. Pulmonary nodules, also multiple, may be detected in a significant proportion of screened individuals.41 Radiomics is a modality that may also enhance the effectiveness of lung cancer screening programs.42
Conclusions
Tuberculosis of the lungs, hilar and mediastinal lymph nodes, and the pleura may be identified following thoracic surgery. However, in such case the diagnosis is often unexpected and initially not taken into account. It can be partially explained by the fact that symptoms of tuberculosis, such as cough and weight loss, also occur in lung cancer. Pulmonary lesions detected by imaging are nonspecific for tuberculosis, either. Nevertheless, they may suggest the potential presence of the disease. The majority of our study patients had lesions that are frequently encountered in tuberculosis and should prompt less invasive procedures. Microbiological examination along with molecular testing could have confirmed tuberculosis. Such tests were not performed, as the radiologists had not initially indicated tuberculosis as a possible diagnosis, although there were premises suggesting it. Tuberculosis should be considered in the differential diagnosis even in the case of radiological findings not regarded as typical of the disease. This emphasizes the role of radiologists in the identification of tuberculosis. The examination of sputum or specimens obtained during bronchoscopy enables a rapid diagnosis of tuberculosis, without delays associated with the diagnostic workup targeted at lung cancer, and thus helps to avoid surgical interventions in some patients.
- European Centre for Disease Prevention and Control/WHO Regional Office for Europe. Tuberculosis surveillance in Europe 2020 – 2018 data. Stockholm, Sweden: ECDC; 2020.
- Korzeniewska‑Koseła M, ed. Tuberculosis and Lung Diseases in Poland in 2019 [in Polish]. Warsaw, Poland: National Tuberculosis and Lung Diseases Research Institute; 2020.
- Didkowska J, Wojciechowska U, Czaderny K, et al. Cancer in Poland in 2017. Warsaw, Poland: Polish National Cancer Registry. Maria Sklodowska‑Curie Institute – Oncology Centre; 2019.
- Korzeniewska‑Koseła M. Standards for tuberculosis care: summary of guidelines of European Centre for Disease Prevention and Control and European Respiratory Society 2017 and World Health Organization 2018 [in Polish]. Med Prakt. 2018; 11: 1‑5.
- Long R, Njoo H, Hershfield E. Tuberculosis: 3. Epidemiology of the disease in Canada. CMAJ. 1999; 160: 185‑190.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION