Dynamics of humoral response to coronavirus antigens among employees of a designated COVID‑19 hospital: an observational study
Key words: antibodies, COVID-19 pandemic, occupational exposure, occupational safety and health, SARS-CoV-2



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Dynamics of humoral response to coronavirus antigens among employees of a designated COVID‑19 hospital: an observational study
Introduction: During the COVID‑19 pandemic studies on workplace safety of hospital staff taking care of patients with this disease are a high priority. We decided to analyze the results of opportunistic screening for anti–SARS‑CoV‑2 antibodies among employees of a designated COVID‑19 center.
Objectives: The aim of the study was to investigate whether potential exposition to SARS‑CoV‑2 antigens is reflected in the results of serological studies.
Patients and methods: Every employee who performed at least a single test between April 21 and July 20, 2020 was included in the study. The tests assessed the levels of immunoglobulin (Ig) G and IgM+IgA. Employees working in direct contact with COVID‑19 patients and those participating in aerosol‑generating procedures were identified.
Results: The results of 2455 tests taken by 1572 employees were analyzed. A total of 357 participants (22.7%) had at least 1 positive or equivocal result during the study period. Linear mixed models revealed gradual increases in mean levels of both IgG and IgM+IgA antibodies among employees with all negative results. The rate of change was higher among persons who had direct contact with COVID‑19 patients and the highest rate of change was observed among individuals participating in aerosol‑generating procedures.
Conclusions: We detected developing humoral immune response to a new set of coronavirus antigens among the study group. It is possible that employees of designated COVID‑19 centers are regularly exposed to noninfectious doses of SARS‑CoV‑2 or its antigens.
What's new?
During the COVID‑19 pandemic, healthcare professionals have been facing a challenge of working in special conditions. One of the widely discussed topics is occupational safety. We aimed to investigate if working in a designated COVID‑19 hospital is reflected in the results of anticoronavirus antibody panels. We analyzed the results of approximately 2500 tests taken by more than 1500 employees and found that about 1 in 4 persons had a positive or equivocal result. Moreover, we detected gradual increases in the levels of antibodies among workers with negative results. Further analysis revealed that the rate of change of antibody levels was higher among employees working in direct contact with COVID‑19 patients; the highest rate of change was found among medical staff participating in high‑risk procedures. It is possible that healthcare workers have regular contact with coronavirus antigens and the immune response depends on the intensity of the exposure.
Introduction
The first wave of the COVID‑19 pandemic in Poland began in March 2020 and approached its maximum of about 350 daily cases, 25 daily deaths and 3000 hospitalized patients in April and May.1 During that time, patients with COVID‑19 in Poland were treated in hospitals transformed into designated COVID‑19 centers; the Central Clinical Hospital of the Ministry of Interior and Administration in Warsaw was one of the largest of them, hosting over 850 beds in 27 wards and clinics.2 The transformation included reorganization of work, implementation of a training system for the usage of personal protective equipment (PPE), and introduction of procedures targeted on ensuring work safety (especially epidemiological safety).3 A reverse transcriptase–polymerase chain reaction (RT‑PCR) assay was used to check if an employee with symptoms of respiratory tract infection had COVID‑19.
Additionally, as of April 21, 2020, a system of opportunistic screening for anti–SARS‑CoV‑2 antibodies among hospital staff was implemented. In contrast to the RT‑PCR tests, which detect active infections, serological studies check if a person had contact with viral antigens. Little is known about the level of anti–SARS‑CoV‑2 seroprevalence in Poland (particularly during the first wave of the pandemic) and the dynamics of the levels of antibodies among healthcare workers has not been analyzed yet. The aim of the present study was to investigate if potential exposition to SARS‑CoV‑2 antigens is reflected in the results of the screening tests, and whether the antibody levels are dependent on the time of testing and type of work performed.
Patients and methods
Design and setting
This observational study included every employee of the Central Clinical Hospital of the Ministry of Interior and Administration in Warsaw who took at least a single test for the levels of anti–SARS‑CoV‑2 antibodies between April 21 and July 20, 2020. There were no exclusion criteria. All employees of the hospital were followed‑up for development of COVID‑19 symptoms until the end of July 2020. Every employee with symptoms of respiratory tract infection was obligatorily tested for COVID‑19 with RT‑PCR of nasopharyngeal swab specimen. In case of a positive result, employees who had had relevant contact with the infected person (as described by the World Health Organization guidelines)4 were also tested.
The study protocol was approved by the Ethics Committee of the Central Clinical Hospital of the Ministry of Interior and Administration, Warsaw, Poland (no. 209/2020).
System of screening for anti–SARS‑CoV‑2 antibodies
A system of opportunistic screening for anti–SARS‑CoV‑2 antibodies was started on April 21, 2020. Every employee had an opportunity to test serum levels of immunoglobulin (Ig) G as well as combined levels of IgM and IgA with a COVID‑19 enzyme‑linked immunosorbent assay (Vircell Microbiologists, Granada, Spain; G10325 and MA10326). The test was recommended to be repeated approximately every 2 weeks. All samples were assayed and validated according to manufacturer’s instructions. The cutoff values for equivocal and positive results were 6 and 8 U for the IgM+IgA assay and 4 and 6 U for the IgG assay, respectively. All individuals with equivocal or positive test results were tested for COVID‑19 with RT‑PCR of nasopharyngeal swab specimen.
The specificity declared by the manufacturer is 98% and 99% for the IgG and IgM+IgA assays, respectively. The sensitivity depends on time from onset of the disease and amounts to 83% and 87% for IgG and IgM+IgA assays performed 5 days after a positive RT‑PCR result, respectively. The within‑run and between‑run precision coefficients of variation are declared not to exceed 5% and 9%, respectively. The IgG assay is declared not to cross‑react with parainfluenza virus, influenza A and B viruses, adenovirus, respiratory syncytial virus, Mycoplasma pneumoniae, Chlamydophila pneumoniae, Coxiella burnetii, and Legionella pneumophila. The manufacturer declares no cross‑reactivity of the IgM+IgA assay with influenza A and B viruses or Legionella pneumophila, while it was found to partially cross‑react with adenovirus, Mycoplasma pneumoniae, Chlamydophila pneumoniae, Coxiella burnetii, and respiratory syncytial virus.
Study population and data collection
The results of all antibody tests performed between April 21 and July 20, 2020 were obtained from the diagnostic laboratory; the study period was 13 weeks. Data regarding sex, type and place of work, and RT‑PCR results (where applicable) were analyzed. All participants were assessed in terms of having direct contact with COVID‑19 patients and participating in aerosol‑generating procedures.
Statistical analysis
Statistical analysis was performed using the SAS software, version 9.4 (SAS Institute Inc, Cary, North Carolina, United States). Quantitative variables were described using medians and interquartile ranges (IQRs), whereas qualitative variables were expressed as numbers and percentages. We decided to distinguish a subgroup of persons with at least a single positive or equivocal result of either the IgM+IgA or IgG assay. It was compared with the subgroup of Ig‑negative employees by the use of the χ2 test. We used linear mixed models for repeated measures over time by type of work to analyze changes in the levels of IgM+IgA and IgG antibodies among the Ig‑negative subgroup and the impact of direct contact with COVID‑19 patients with fixed effects of time, type of work, and interaction between time and type of work (SAS Proc Mixed). This approach allowed for participants to differ in terms of testing schedules and numbers of tests performed. Analysis of the results of all participants would require the calculation of nonlinear mixed model; we were unable to perform such analysis due to insufficient data quality. Time distribution of positive / equivocal test results and positive results of RT‑PCR assays was also studied. The level of significance was set at a P value of 0.05.
Results
A total of 1572 employees took the opportunity to test the levels of anti–SARS‑CoV‑2 antibodies. Approximately 63% of employees were working in direct contact with COVID‑19 patients (both in the study group and among all employees of the hospital). Since the beginning of the pandemic, 30 persons were diagnosed with COVID‑19. One in 5 tested individuals had a positive or equivocal IgG or IgM+IgA result during the study period. As described above, every such person was tested for COVID‑19 with RT‑PCR of nasopharyngeal swab specimen and 2 tests were positive. These employees were a personal care aide and a medical secretary; they presented no symptoms and epidemiologic investigation did not identify the source of the infection. Both persons had maximum detectable levels of IgM+IgA (40 units), whereas their levels of IgG amounted to 25.5 and 5.8 units, respectively. A total of 17 employees tested the levels of antibodies after COVID‑19; the median (IQR) levels of IgM+IgA and IgG were 12.0 (6.7–17.3) U and 31.6 (20.9–40) U, respectively.
The occupational structure of the study group and all hospital employees was similar; however, the percentage of nurses and midwifes was higher in the study group (33.1% vs 27.8%; P <0.001), whereas the percentage of physicians was lower (11.5% vs 16.1%; P <0.001). The comparison between the study group and all employees of the hospital is presented in Table 1.
Characteristic | All employees | Study group | |||
Total | Employees with negative test results | Employees with positive or equivocal test results | |||
Data are presented as number (percentage).
a Persons with a positive result of the RT‑PCR test
Abbreviations: RT‑PCR, reverse transcriptase–polymerase chain reaction | |||||
Number of employees | 3177 | 1572 | 1215 | 357 | |
Female sex | 2435 (76.6) | 1284 (81.7) | 983 (80.9) | 301 (84.3) | |
COVID‑19a | 30 (0.9) | 19 (1.2) | 0 | 19 (5.3) | |
Direct contact with COVID‑19 patients | Total | 1996 (62.8) | 986 (62.7) | 732 (60.2) | 254 (71.1) |
Physician | 510 (16.1) | 181 (11.5) | 138 (11.4) | 43 (12) | |
Nurse or midwife | 882 (27.8) | 521 (33.1) | 386 (31.8) | 135 (37.8) | |
Other medical staff | 224 (7.1) | 107 (6.8) | 79 (6.5) | 28 (7.8) | |
Support and technical staff | 380 (12) | 177 (11.3) | 129 (10.6) | 48 (13.5) | |
No direct contact with COVID‑19 patients | Total | 1181 (37.2) | 586 (37.3) | 483 (39.8) | 103 (28.9) |
Medical staff | 548 (17.2) | 252 (16) | 207 (17) | 45 (12.6) | |
Nonmedical staff | 633 (19.9) | 334 (21.3) | 276 (22.7) | 58 (16.3) | |
Participation in aerosol‑generating procedures | Yes | – | 332 (21.1) | 253 (20.8) | 79 (22.1) |
No | – | 1240 (78.9) | 962 (79.2) | 278 (77.9) | |
Overall, 2455 samples were tested. A majority of the employees (68.3%) assessed their levels of antibodies only once; 14% repeated the test 3 or more times. The percentage of positive / equivocal samples (either IgM+IgA or IgG) amounted to 18.4%. Sixty‑four out of 277 positive / equivocal IgM+IgA results and 52 out of 259 positive / equivocal IgG results were higher than 2 times the upper limit of the normal range. The results of all tests are summarized in Table 2.
Characteristic | Value | |
Data are presented as number (percentage) unless otherwise indicated.
a Percentage of all persons
b Percentage of all tests
Abbreviations: IgA, immunoglobulin A; IgM, immunoglobulin M; IgG, immunoglobulin G; IQR, interquartile range | ||
Total number of tests | 2455 | |
IgM+IgA, U, median (IQR); range | 2.5 (1.6–4); 0–40 | |
IgG, U, median (IQR); range | 1.9 (1.4–2.8); 0–44.8 | |
Test repetitions per person, n | 1 | 1074 (68.3)a |
2 | 271 (17.2)a | |
≥3 | 227 (14.4)a | |
Persons with a positive / equivocal result | Total | 357 (22.7)a |
Positive IgM+IgA | 104 (6.6)a | |
Equivocal IgM+IgA | 107 (7.4)a | |
Positive IgG | 74 (4.7)a | |
Equivocal IgG | 136 (8.7)a | |
Tests with a positive / equivocal result | Total | 451 (18.4)b |
Positive IgM+IgA | 152 (6.2)b | |
Equivocal IgM+IgA | 125 (5.1)b | |
Positive IgG | 103 (4.2)b | |
Equivocal IgG | 156 (6.4)b | |
The subgroup of employees with positive / equivocal results of antibody tests was analyzed separately. The structure of this group differed from the structure of the subgroup with negative results—254 out of 357 individuals from the former subgroup (71.1%) had contact with COVID‑19 patients as opposed to 732 out of 1215 persons (60.2%) from the latter subgroup (P <0.001). The groups did not differ in terms of percentage of personnel participating in aerosol‑generating procedures (22.1% vs 20.8%, respectively; P = 0.6). Occupational structure of the groups of employees working in direct contact with COVID‑19 patients also did not differ, regardless of the test results (P = 0.9).
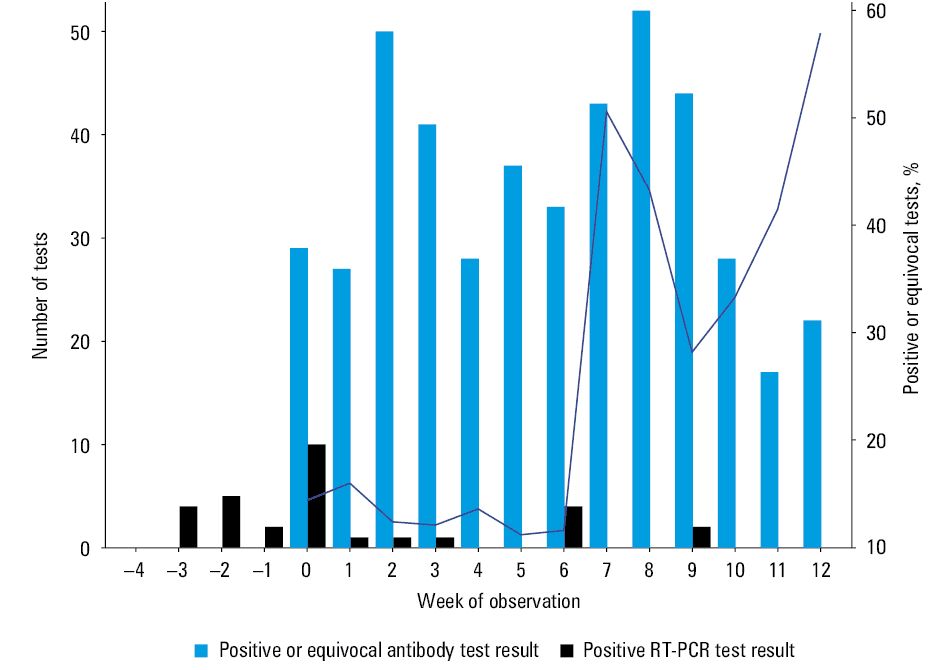
Time distribution of Ig‑positive / equivocal samples and RT‑PCR positive tests is presented in Figure 1. Screening for anti–SARS‑CoV‑2 antibodies started on April 21, 2020 (week 0). About 30 to 50 Ig‑positive / equivocal samples were detected every week by the end of week 10 of the study period. The number of Ig‑positive / equivocal samples in the last 2 weeks of observation was smaller and amounted to approximately 20. The weekly rate of positive / equivocal results was constant during weeks 0 to 6. Starting from the seventh week, the rate increased, with a subsequent temporary fall in weeks 9 and 10.
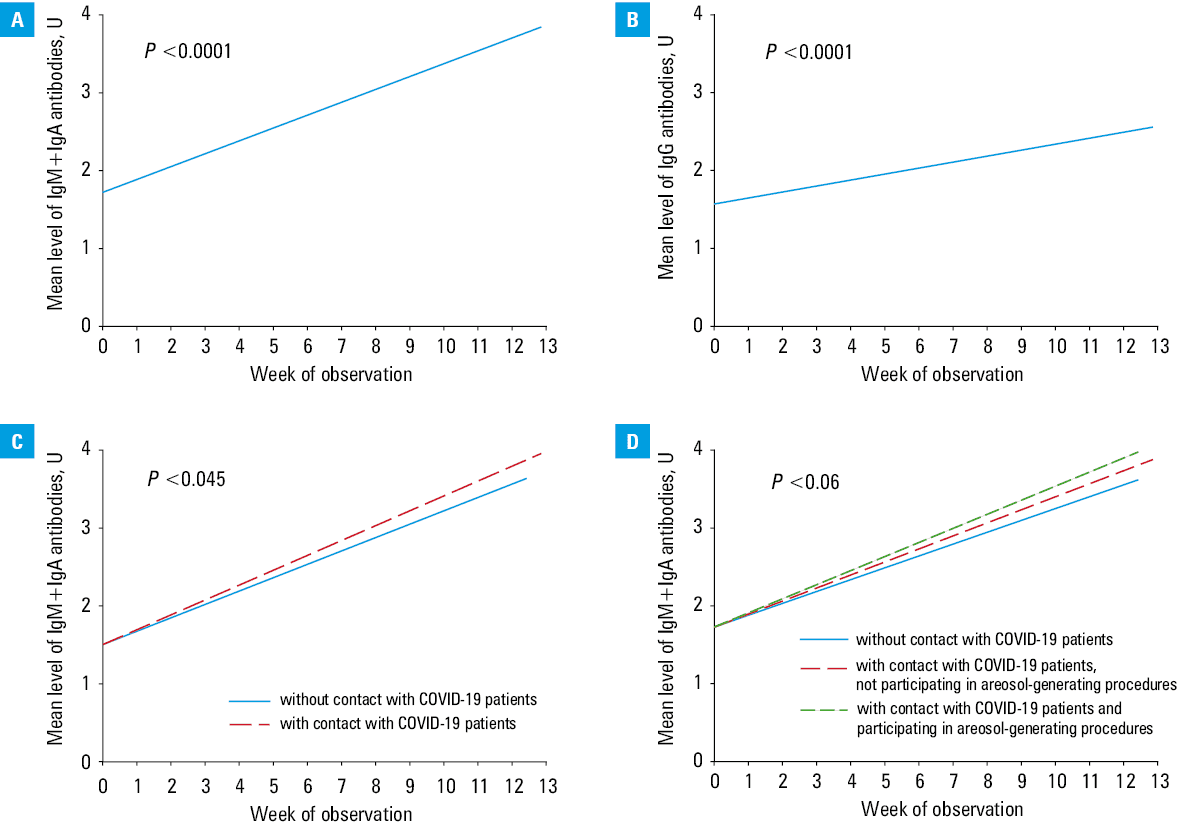
Linear mixed models for repeated measures over time showed that the mean levels of IgM+IgA and IgG antibodies among Ig‑negative employees increased by 0.66 U (P <0.001) and 0.31 U (P <0.001) monthly, respectively (Figure 2A and 2B). Female employees had a higher initial level of IgM+IgA by 0.15 U (P = 0.045), while monthly rate of change did not differ between the sexes. Further analysis revealed an interaction between time and type of work: monthly increase in the level of IgM+IgA antibodies was higher by 0.09 U among personnel working in direct contact with COVID‑19 patients (P = 0.045) (Figure 2C). The difference in monthly increase in the level of of IgG antibodies was not significant (P = 0.17) We further divided the group of participants working in direct contact with COVID‑19 patients in terms of participating in aerosol‑generating procedures. The linear mixed model showed a difference of 0.06 U in the monthly rate of change of IgM+IgA antibodies between individuals participating and not participating in aerosol‑generating procedures and those without direct contact with COVID‑19 patients (P = 0.06). Employees participating in aerosol‑generating procedures had the highest monthly rate of change of IgM+IgA antibodies (Figure 2D). Covariance structure analysis revealed that the model fully explained the differences in individual rates of change.
Discussion
The main objective of the study was to investigate the dynamics of the levels of anti–SARS‑CoV‑2 antibodies amongst employees of a large, designated COVID‑19 hospital. We found that during 13 weeks of the study period 357 out of 1572 (22.7%) persons who took part in screening had positive or equivocal levels of IgM+IgA or IgG antibodies. Amongst them, only 17 were diagnosed with COVID‑19 before and in 2 cases RT‑PCR test was positive. We also found gradual increases in mean levels of antibodies of both classes amongst the remaining 1215 employees (increase in the levels of IgM+IgA was steeper). The results suggest the presence of developing immune response to a new set of antigens among the study group. It is possible that employees of designated COVID‑19 centers have regular contact with noninfectious amounts of SARS‑CoV‑2 or its antigens (small amounts of SARS‑CoV‑2 were detected in social and storage areas as well as in ventilation systems)7-9, which is reflected in the results of serological studies. Of note, due to the fact that screening for antibodies was voluntary, with no formal requirement of serial testing, only about one‑third of participants were tested twice or more times; however, the statistical analysis accounted for this issue.
Further analysis revealed that groups of employees with positive or equivocal and negative results of serological test differed significantly. Namely, the percentage of persons working in direct contact with COVID‑19 patients was higher amongst the group with positive / equivocal test results. The rate of increase in the levels of IgM+IgA was also higher among persons working directly with COVID‑19 patients. The highest rate of increase in the IgM+IgA levels was observed among employees participating in aerosol‑generating procedures. Therefore, it seems that the groups differed also in terms of exposure to the viral antigens; the difference cannot be explained by the presence of the virus in social or storage areas and ventilation systems, because they are commonly used. The effectiveness of PPE does not reach 100%10,11 and doffing procedures are also imperfect,12,13 which may lead to additional exposure to SARS‑CoV‑2 antigens among employees working in “red zones.” Moreover, wearing PPE is not obligatory during contact with convalescents, who are known to produce viral antigens for weeks after diagnosis.14
Our findings suggest that even incidental contact with viral antigens leads to the production of specific antibodies. During the epidemic, more and more people have contact with viral antigens, even without getting infected (eg, too short / small exposure to evoke infection, inhalation of inactive virions or antigens only). Therefore, we can expect growing percentages of persons with positive results of antibody tests. Unfortunately, the seroprevalence among healthcare professionals in Poland has not yet been studied. Moreover, we did not find a study on longitudinal changes in seroprevalence among the general Polish population; only a series of cross‑sectional studies has been published to date. On that basis, it can be observed that the percentage of persons with IgG antibodies has increased from about 4.3%, as assessed in July and August 2020 (a group of police officers),15 to approximately 18% in December 2020 and 25% in February 2021 (a project called West Pomeranian Monitoring and Prevention Program of Coronavirus SARS‑CoV‑2 and COVID‑19 Disease [Zachodniopomorski Program Monitorowania i Prewencji Epidemii Coronawirusa SARS‑CoV‑2 i Choroby COVID‑19], unpublished data).16,17 When it comes to seroprevalence of anti–SARS‑CoV‑2 antibodies among healthcare workers as well as risk factors of elevated levels of immunoglobulins (direct contact with COVID‑19 patients, participating in aerosol‑generating procedures), our findings are consistent with a recent meta‑analysis.18
It is noteworthy that the weekly number of tests decreased 2 to 3 times starting from week 7. This may be due to 2 factors. The first is the start of a holiday season (including a 4‑day long weekend in the seventh week). The second is a change in the general approach to the pandemic—the first wave was over, and people tended to forget about coronavirus. Considering that the number of positive / equivocal results remained high despite a decline in the weekly number of tests, we can suspect that if the same number of tests continued to be performed, the number of observed positive / equivocal results would be amplified.
Our observational study has several limitations. The relation between the levels of anti–SARS‑CoV‑2 antibodies and immunity to COVID‑19 remains unknown. The system of screening for antibodies was opportunistic, which may have resulted in selection bias, even despite the presented comparison of occupational structure. It cannot be ruled out that cross‑reactions with other viruses and bacteria were detected. However, the specificity of the test, as declared by the manufacturer, is high and other pathogens have been common for decades; therefore, the mean levels of antibodies should remain stable. We did not detect differences between the rate of change of IgG antibody levels between participants who work in direct contact with COVID‑19 patients and those who do not. The possible explanation is a slower response of this class of antibodies leading to smaller effect size and insufficient power of the study.
Our analysis revealed that healthcare workers employed in a designated COVID‑19 center are developing humoral immune response to SARS‑CoV‑2, even without getting infected. Taking into account the close association between the presence of anti–SARS‑CoV‑2 antibodies and a substantially reduced risk of infection and severe COVID‑19,19 we can expect that the seropositive employees are protected from severe course of the disease. Additionally, contact with coronavirus antigens within the community may contribute to achieving herd immunity in an analogous way. However, these hypotheses are yet to be tested. Our findings also confirm the efficacy of wearing PPE in preventing infection with SARS‑CoV‑2.
- Raciborski F, Pinkas J, Jankowski M, et al. Dynamics of the coronavirus disease 2019 outbreak in Poland: an epidemiological analysis of the first 2 months of the epidemic. Pol Arch Intern Med. 2020; 130: 615‑621. | Crossref
- Nowak B, Szymański P, Pańkowski I, et al. Clinical characteristics and short‑term outcomes of patients with coronavirus disease 2019: a retrospective single‑center experience of a designated hospital in Poland. Pol Arch Intern Med. 2020; 130: 407‑411. | Crossref
- Król Z, Szymański P, Bochnia A, et al. Transformation of a large multi‑speciality hospital into a dedicated COVID‑19 centre during the coronavirus pandemic. Ann Agric Environ Med. 2020; 27: 201‑206. | Crossref
- World Health Organization. Risk assessment and management of exposure of health care workers in the context of COVID‑19. https://apps.who.int/iris/handle/10665/331496. Accessed December 3, 2020.
- Vircell S.L. COVID‑19 ELISA IgG, manufacturer information. https://www.abacusdx.com/media/VIRCLIA_G1032.pdf. Accessed April 10, 2021.
ARTICLE INFORMATION