Should we supplement zinc in COVID-19 patients? Evidence from a meta-analysis
Key words: COVID-19, meta-analysis, SARS-CoV-2, zinc



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Should we supplement zinc in COVID-19 patients? Evidence from a meta-analysis
Introduction: Preliminary retrospective reports showed that zinc supplementation may decrease mortality in patients with COVID‑19, postulating the potential therapeutic efficacy of zinc in the management of the disease.
Objectives: We sought to summarize the studies published to date regarding the antiviral activity of zinc in patients with COVID‑19.
Patients and methods: A meta‑analysis was performed to compare the outcomes of hospitalized patients receiving zinc supplementation and those treated with standard care. The primary outcome was survival to hospital discharge. Secondary outcomes were in‑hospital mortality and length of stay in hospital or intensive care unit (ICU).
Results: Data relating to 1474 patients included in 4 studies were analyzed. Survival to hospital discharge was 56.8% in the zinc group compared with 75.9% in the nonzinc group (P = 0.88). In‑hospital mortality was 22.3% in the zinc group compared with 13.6% in the standard care group (P = 0.16). The mean (SD) length of hospital stay was 7.7 (3.7) days in the zinc group and 7.2 (3.9) days in the standard treatment group (P <0.001). The mean (SD) length of ICU stay was 4.9 (1.7) days in the zinc group and 5.8 (1.9) days in the standard care group (P = 0.009).
Conclusions: Zinc supplementation did not have any beneficial impact on the course of COVID‑19 evaluated as survival to hospital discharge and in‑hospital mortality. The zinc‑supplemented group had longer hospital stay despite shorter ICU stay. At present, there are no evidence‑based data to support routine zinc supplementation in patients with COVID‑19.
What's new?
Zinc supplementation was postulated to decrease mortality in patients with COVID‑19. We performed a meta‑analysis to compare zinc with standard care in this population. Zinc supplementation did not have any beneficial impact on the course of the disease. The zinc‑supplemented group had a longer length of hospital stay. No evidence‑based data support routine zinc supplementation in COVID‑19.
Introduction
Ever since the pneumonia outbreak of unknown origin was reported in China in late 2019, which expanded all over the world, the global healthcare systems have been under severe pressure.1,2 The new virus was called severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2) by the international committee of the Coronavirus Study Group.3 Due to the rapid spread of the disease, it was declared a pandemic by the World Health Organization.4 The major strain on healthcare systems exerted by the virus raised an urgent need for new treatment options to alleviate the SARS‑CoV‑2 pandemic. Efforts were made to administer agents known to restrict viral growth, including zinc. Zinc was shown to inhibit the in vitro reproduction of coronaviruses5 and to participate in the immunological response, especially involving T lymphocytes.6,7 Zinc’s mechanism of action is pleiotropic and associated with multiple pathways that participate in the inflammatory response. The baseline function of zinc is the reduction of the oxidative stress and inflammation.8 Additionally, zinc is associated with the negative feedback loop decreasing the activity of nuclear factor kappa B, thus alleviating sepsis and excessive inflammation9 and potentially reducing the cytokine storm—a phenomenon associated with severe COVID‑19.10 Interestingly, the interaction between the peptidase domain of angiotensin‑converting enzyme 2 and SARS‑CoV‑2 spike protein, which is crucial for the entry of the virus into the cell,11 is also modulated by zinc levels.12
Zinc supplementation was shown to decrease mortality in severe pneumonia.13 At the very beginning of the COVID‑19 pandemic, the idea of chloroquine derivatives as ionophores for intracellular uptake of zinc into lysosomes was postulated.14 Thus, investigators have focused their attention on zinc as a promising agent in the management of COVID‑19. To summarize the studies conducted hitherto into the antiviral activity of zinc in COVID‑19 patients, a meta‑analysis was performed to compare the outcomes of the hospitalized patients receiving zinc supplementation and those treated with standard care.
The primary outcome was survival to hospital discharge. Secondary outcomes were in‑hospital mortality and length of stay in the hospital or intensive care unit (ICU).
Patients and methods
This systematic review and meta‑analysis were carried out following the Preferred Reporting Items for Systematic Reviews and Meta‑Analyses (PRISMA) guidelines and the recommendations of the Cochrane Collaboration.15
Search strategy
Two authors (LS and MP) independently searched PubMed, Scopus, and the Cochrane Library for articles published in English from the inception of the databases until February 10, 2021. The search was performed using the following terms: SARS‑CoV‑2 OR COVID‑19 OR coronavirus AND zinc. The references listed in the identified articles were also reviewed. A manual search for the related articles was conducted in order to identify all eligible studies and achieve minimal publication bias.
Inclusion and exclusion criteria
Studies included in this meta‑analysis fulfilled the following PICOS criteria: 1) participants: patients with a confirmed diagnosis of COVID‑19; 2) intervention: zinc supplementation; 3) comparison: standard care; 4) outcomes: detailed information for survival; and 5) study design: randomized controlled trials, quasi‑randomized or observational studies comparing the effect of zinc and standard care on patient outcomes. Studies were excluded if they were reviews, animal studies, case reports, letters, conference or poster abstracts, or articles not containing original data.
Study selection
The studies were independently screened by 2 authors (LS and MP) who assessed the study titles and abstracts for potential eligibility. After reviewing the full texts, eligible studies were included according to the previously determined study inclusion criteria. Discrepancies in the selection of articles were resolved by consensus with a third reviewer (JS).
Data extraction
Raw data were extracted using a standardized, premade form. Care was taken to avoid including data from duplicate publications. In the event of any suspected data discrepancies, the relevant author was contacted directly. Data extracted from eligible studies included the following characteristics: study and year, country, type of participants, number of participants, types of therapy, mortality rate, adverse event occurrence as well as length of stay in hospital or ICU.
Risk of bias assessment
Two investigators (LS and AG) independently extracted individual study data and assessed studies for risk of bias. Any disagreements were discussed and resolved in a consensus meeting with the third reviewer (MJJ). The risk of bias was assessed using the ROBINS‑I tool in nonrandomized trials16 and the RoB 2 tool in randomized studies.17 The Robins application was used to visualize risk of bias assessments.18 The scale has 7 main domains (confounding, participant selection, classification of interventions, deviation from intended interventions, missing data, outcome measurement, and selection of reported results) and assigns 1 point for each of the following 4 judgments: critical, serious, moderate, and low. The review authors’ judgments about each risk of bias item are provided in Supplementary material, Figures S1–S3.
Statistical analysis
Statistical analysis was performed in Review Manager, version 5.4 (Nordic Cochrane Center, The Cochrane Collaboration, Copenhagen, Denmark). The Mantel‑Haenszel method was used to analyze dichotomous outcomes, and results were reported as risk difference (RD) with 95% CI and 2‑tailed P values. Continuous outcome differences were analyzed using an inverse variance model with 95% CI, and values were reported as mean differences (MD). When the continuous outcome in a study was reported as median, range, and interquartile range, means (SD) were estimated using the formula described by Hozo et al.19 Heterogeneity in each analysis was quantified by the τ2 and I2 statistics. Heterogeneity was detected with the χ2 test with n–1 degrees of freedom, which was expressed as I2. Values of I2 greater than 50% and greater than 75% were considered to indicate, respectively, moderate and significant heterogeneity among studies. A P value of less than 0.05 was considered statistically significant.
Results
Characteristics of the studies included in the meta‑analysis
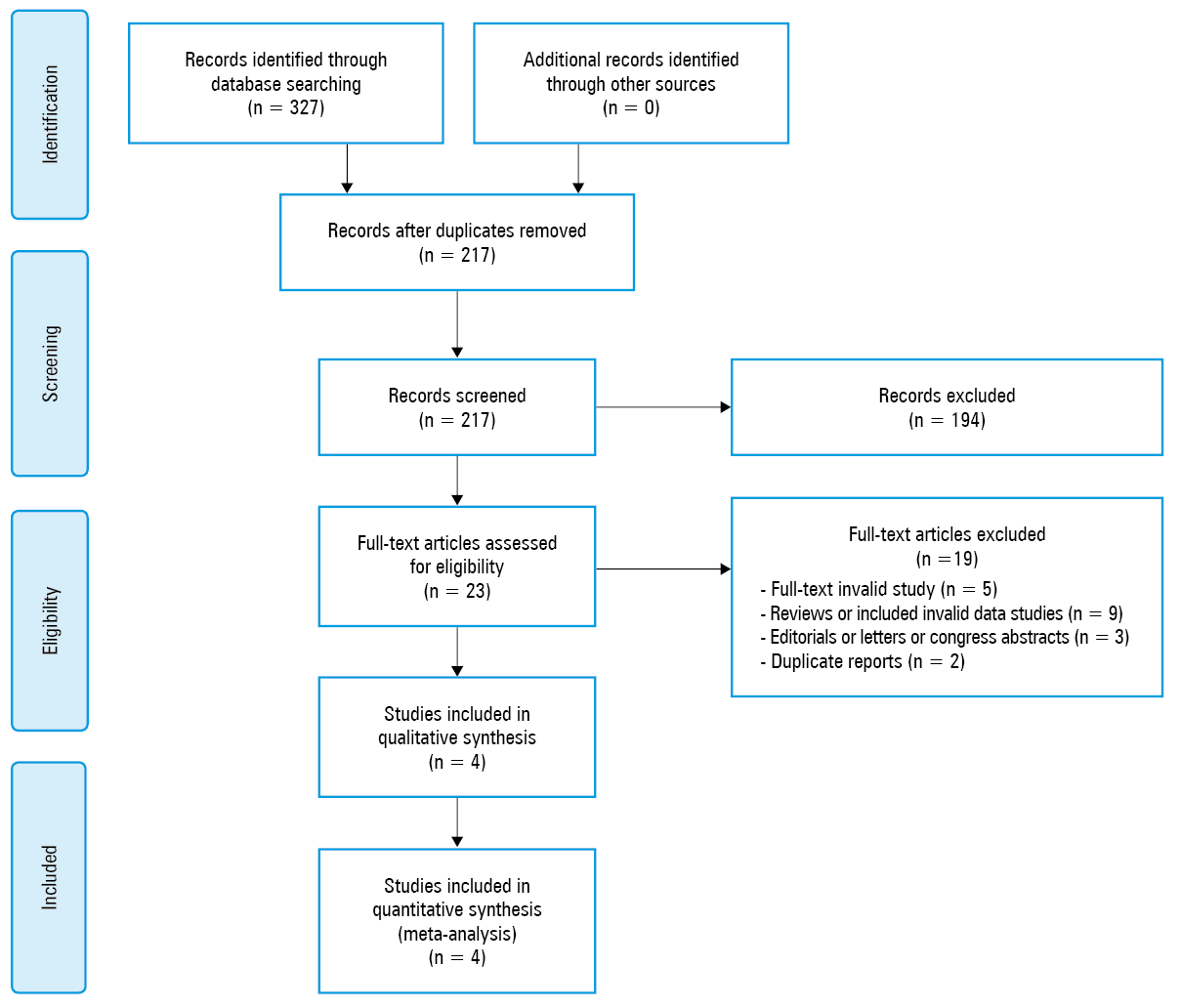
A flow diagram summarizing the literature search is presented in Figure 1. The search of electronic databases initially identified 217 articles for review. Of those, 194 studies were excluded as being unrelated. The remaining 23 articles were carefully examined to determine whether they met the authors’ inclusion criteria. Ultimately, 4 articles that met the inclusion criteria and contained the necessary data for the planned comparison were identified.20-23
In total, 761 patients were treated with zinc supplementation, and 712 with standard care. Three of the studies were conducted in the United States and one in Egypt. The details of the selected trials are summarized in Table 1. The methodology characteristics and comorbidities of patients in the included studies are presented in Supplementary material, Tables S1 and S2, respectively. The mean (SD) age of the patients treated with zinc was 59.7 (15.4) years, compared with 58.6 (17.2) years in the standard care group (MD, –0.89; 95% CI, –5.27 to 3.48; P = 0.69; I2 = 88%).
Parameter | Treatment | Abd‑Elsalam et al20 (2020) | Carlucci et al21 (2020) | Thomas et al22 (2021) | Yao et al23 (2021) |
Abbreviations: NS, not specified | |||||
Country | – | Egypt | United States | United States | United States |
Study design | – | Randomized controlled study | Retrospective analysis | Prospective randomized controlled open‑label trial | Single‑institution retrospective study |
Patients, n | Zinc | 96 | 411 | 58 | 196 |
Standard care | 95 | 521 | 50 | 46 | |
Age, y, mean (SD) | Zinc | 43.48 (14.62) | 63.19 (15.18) | 44.1 (14.8) | 65 (4) |
Standard care | 43.64 (13.17) | 61.83 (15.97) | 42 (14.6) | 71 (7.5) | |
Body mass index, mean (SD) | Zinc | NS | 29.4 (1.3) | 30.4 (3.4) | 28.8 (1.1) |
Standard care | NS | 29.4 (1.2) | 31.5 (3.6) | 26.2 (2) | |
Outcomes
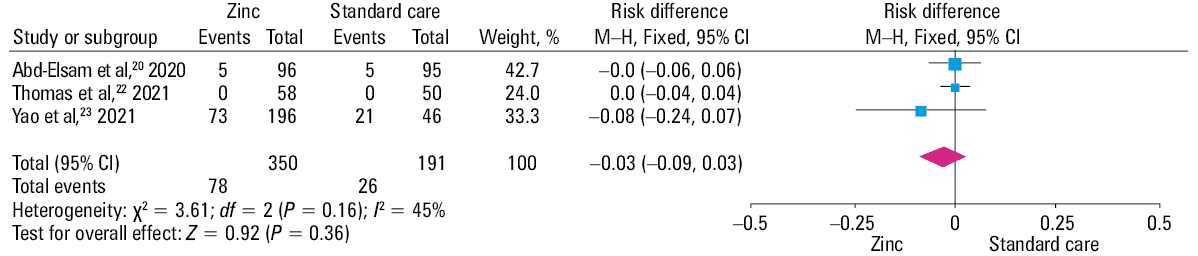
Survival to hospital discharge was reported in 2 studies and was 56.8% in the zinc group compared with 75.9% in the nonzinc group (RD, 0.01; 95% CI, –0.07 to 0.08; P = 0.88; I2 = 0%, Figure 2). Three studies reported in‑hospital mortality, which was 22.3% in the zinc group compared with 13.6% in the standard care group (RD, –0.03; 95% CI, –0.09 to 0.03; P = 0.16; I2 = 45%; Figure 3).

Abbreviations: M–H, Mantel–Haenszel model
Abbreviations: see Figure 2
The mean (SD) length of hospital stay was 7.7 (3.7) days in the zinc group and 7.2 (3.9) days in the standard treatment group (MD, 0.3; 95% CI, 0.18–0.41; P <0.001; I2 = 0%; Supplementary material, Figure S3). The mean (SD) length of ICU stay was reported only by Carlucci et al21 and was 4.9 (1.7) days in the zinc group and 5.8 (1.9) days in the standard care group (MD, –0.9; 95% CI, –1.58 to –0.22; P = 0.009).
Discussion
The main finding of this meta‑analysis is that zinc supplementation has no positive impact on the course of COVID‑19, evaluated in terms of survival to hospital discharge and in‑hospital mortality. The zinc‑supplemented group had a significantly longer hospital ICU length of stay, although the latter result might be questionable due to the considerable discrepancy in the size of the analyzed groups and the predominant role of the study by Carlucci et al21 in this synthesis (weight, 99.5%). Our findings contradict the unambiguous advantages of zinc antiviral activity in clinical practice, both in monotherapy and in combination with hydroxychloroquine / chloroquine, which increases intracellular zinc transport. The National Institute of Health recommends a daily dose of zinc of up to 8 mg for adult women and 11 mg for men,24 while the dose used in clinical trials ranges up to 50 mg daily.25 Overdosing of zinc causes nausea, vomiting, diarrhea, lethargy, and disorders of copper metabolism,26 further discouraging zinc supplementation in COVID‑19 patients.
The study by Carlucci et al21 was the only one to show that the addition of zinc sulfate decreased mortality or transfer to hospice, but only in the case of patients who were never admitted to the ICU. In this study, patients treated with zinc sulfate had higher baseline absolute lymphocyte counts, which is in agreement with previous finding that zinc stimulated lymphocytogenesis.27 Based on the results, it might be hypothesized that zinc is a useful tool in preventing progression of the disease, but once it progresses to the cytokine storm, the zinc activity is no longer viable.28 However, owing to the retrospective design of the study by Carlucci et al,21 caution should be exercised in drawing conclusions. The following randomized controlled trials, that is, Abd‑Elsalam et al20 and Thomas et al,22 failed to reveal any beneficial role for zinc in the therapeutic management of COVID‑19, compared with standard of care.
The hypothesis that there is a relationship between zinc supplementation and COVID‑19 outcomes was based on the results of a retrospective study in a relatively small cohort of 275 patients that showed the median blood zinc level to be significantly lower in COVID‑19 patients with poor clinical outcome than in patients with good clinical outcome (840 mg/l vs 970 mg/l; P <0.0001).29 Based on the results of this meta‑analysis, despite some evidence that low zinc levels are associated with a worse prognosis, at present there are no evidence‑based data to support the concept of zinc supplementation in patients with COVID‑19.
We acknowledge the limitations of our analysis. First, 2 studies provided retrospective data, while only 2 offered prospective data. Also, there was a low number of enrolled individuals in our analysis. Furthermore, there are notable differences in zinc formulation supplements that greatly affect absorption of zinc and might not be mutually compared. For example, oral zinc picolinate supplementation has different absorption compared to zinc citrate, sulphate, or gluconate. Hence, our results should be interpreted with caution. For a definitive answer to this question, it would be necessary to conduct double‑blind placebo‑controlled trials.
Conclusions
Despite early evidence supporting the potential benefits of zinc supplementation in COVID‑19 patients, which was based on retrospective studies and in vitro findings, the effectiveness of zinc supplementation in the treatment of COVID‑19 was not proven in this meta‑analysis.
- Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020; 395: 470‑473. | Crossref
- Dzieciatkowski T, Szarpak L, Filipiak KJ, et al. COVID‑19 challenge for modern medicine. Cardiol J. 2020; 27: 175‑183. | Crossref
- Guo YR, Cao QD, Hong ZS, et al. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID‑19) outbreak – an update on the status. Mil Med Res. 2020; 7: 11. | Crossref
- World Health Organization. Coronavirus disease (COVID‑19) pandemic. https://www.who.int/emergencies/diseases/novel‑coronavirus‑2019. Accessed, March 4, 2021.
- te Velthuis AJ, van den Worm SH, Sims AC, et al. Zn (2+) inhibits coronavirus and arterivirus RNA polymerase activity in vitro and zinc ionophores block the replication of these viruses in cell culture. PLoS Pathog. 2010; 6: e1001176. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION