Panhypopituitarism, oral ulcer as well as maxillofacial and other osteolytic bone lesions in a young adult



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Panhypopituitarism, oral ulcer as well as maxillofacial and other osteolytic bone lesions in a young adult
An apparently healthy 22‑year‑old man was treated by a dentist due to inflammation of the left mandible. He was a nonsmoker of cigarettes but a cannabis user. Empiric antibiotic therapy and endodontic treatment of tooth 35 were implemented without success. Subsequently, the patient was hospitalized. Weight loss (body mass index, 15.9 kg/m2), polyuria, polydipsia, and ulceration extending from the distal surface of teeth 34 to 36 as well as enlarged submandibular lymph nodes were observed (Figure 1A). Pantomography showed an irregular shape of the mandible (Figure 1B). Computed tomography revealed osteolytic lesions in the left mandible as well as the right maxillary and right iliac bones (Figure 1C). Laboratory investigations showed increased levels of inflammatory markers (C‑reactive protein, 11.2 mg/l; reference range <10 mg/l, erythrocyte sedimentation rate, 12 mm/h), anemia (hemoglobin, 11.1 g/dl; reference range, 13.7–17.5 g/dl), deficiency of thyrotropin, testosterone, and antidiuretic hormone as well as hypoadrenocorticism. A urine test showed a reduced specific gravity of 1.010 g/l. Magnetic resonance imaging showed a tumor arising from the pituitary stalk pressing on the optic tract, with the absence of a normal, hyperintensive signal of the posterior pituitary lobe, and a nonspecific lesion in the right cerebellar peduncle (Figure 1D). Positron emission tomography showed additional foci with increased fluorodeoxyglucose uptake in the right femur, bilateral tibia, fibula, rib 4, and left shoulder blade. Histopathological examination of the specimen obtained from the mandible revealed infiltration of large, bright cells with folded nuclei, and presence of the CD1a antigen. On that basis, multisystem Langerhans cell histiocytosis (MS‑LCH) with critical organ involvement was diagnosed.
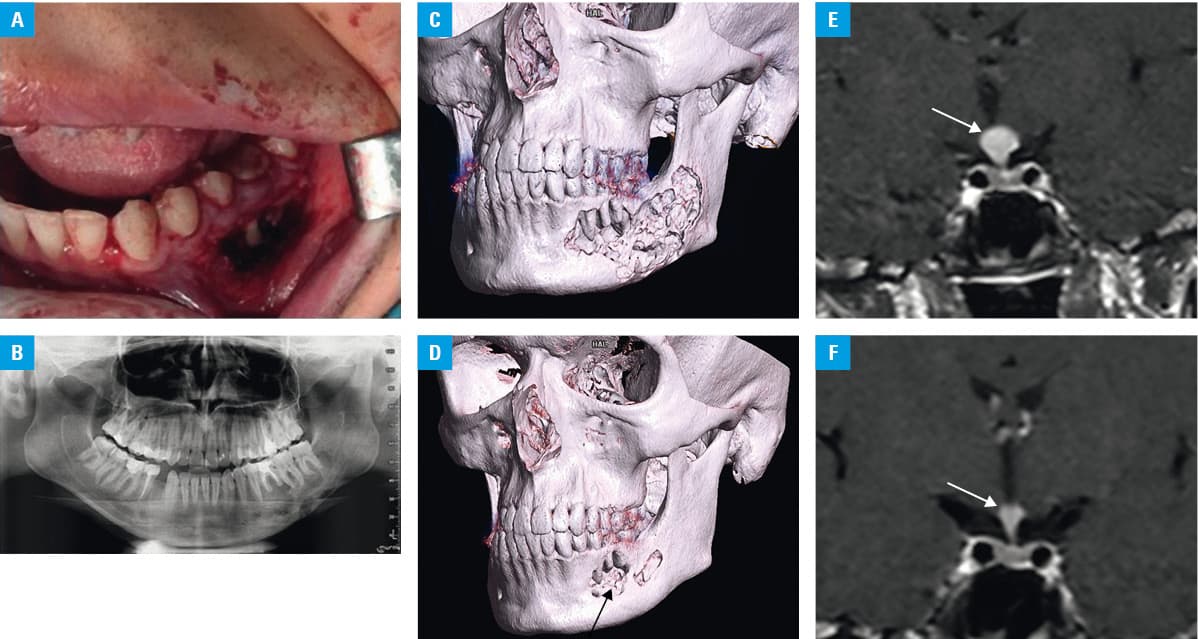
Intravenous cladribine (6 courses at a dose of 6 mg/m2 for 5 days every 4 weeks) and replacement hormone treatment were administered. The general condition of the patient improved with weight gain (25 kg), regression of oral ulceration as well as partial regression of the osteolytic (Figure 1E) and pituitary lesions (Figure 1F).
Langerhans cell histiocytosis is a rare disease caused by proliferation of mutated dendritic cells of myeloid origin. Adult patients with LCH usually present with the involvement of the respiratory (50%–60%), skeletal (60%), and endocrine (40%–70%) systems and the skin (15%–30%). Most commonly, LCH affects young smokers (of tobacco and / or cannabis).1,2 Lesions in the oral cavity may be the first or even the only symptom of LCH. Excessive tooth mobility, absence of periodontal disease, ulcers in the oral cavity, or “floating teeth” on pantomography are suggestive of the disease.3,4
Approximately 20% to 30% of patients with LCH have diabetes insipidus resulting from the involvement of the posterior pituitary; however, panhypopituitarism, as observed in our patient, is very rare in adults. This condition may lead to life‑threatening dehydration.1,2,5 Additionally, in our patient, the lesions in the hypothalamus and the cerebellum were similar, which is extremely rare; lesion regression after treatment proves their histiocytic origin. Treatment of MS‑LCH is based on chemotherapy with cladribine or cytosine arabinoside. The discovery of the role of BRAF mutation in the pathogenesis of LCH enabled the introduction of targeted therapies using BRAF and extracellular signal‑regulated kinase inhibitors.1,2
This case describes MS‑LCH with lesions that are extremely rare in adults (panhypopituitarism, a tumor in the pituitary gland, lesions in the cerebellum and hypothalamus) and a spectacular improvement after cladribine treatment.
- Goyal G, Young JR, Koster MJ, et al. The Mayo Clinic Histiocytosis Working Group consensus statement for the diagnosis and evaluation of adult patients with histiocytic neoplasms: Erdheim‑Chester disease, Langerhans cell histiocytosis, and Rosai‑Dorfman disease. Mayo Clin Proc. 2019; 94: 2054‑2071. | Crossref
- Radzikowska E. Update on pulmonary Langerhans cell histiocytosis. Front Med (Lausanne). 2021; 7: 582581. | Crossref
- Hwang DS, Lee JS, Kim HR, et al. Langerhans cell histiocytosis of the mandible: two case reports and literature review. J Korean Assoc Oral Maxillofac Surg. 2019; 45: 167‑172. | Crossref
- Kim J‑E, Yi W‑J, Heo M‑S, et al. Langerhans cell histiocytosis of the jaw, a mimicker of osteomyelitis on CT and MR images. A retrospective analysis. Medicine (Baltimore). 2019; 98: e16331. | Crossref
- Cantu MA, Lupo PJ, Bilgi M, et al. Optimal therapy for adults with Langerhans cell histiocytosis bone lesions. PLoS One. 2012; 7: e43257. | Crossref
ARTICLE INFORMATION