Association between the geographic region and the risk of familial atrioventricular nodal reentrant tachycardia in the Polish population
Key words: atrioventricular nodal reentrant tachycardia, familial atrioventricular nodal reentrant tachycardia, inherited arrhythmias



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Association between the geographic region and the risk of familial atrioventricular nodal reentrant tachycardia in the Polish population
Introduction: Atrioventricular nodal reentrant tachycardia (AVNRT) is one of the most common regular supraventricular arrhythmias referred for catheter ablation (CA). In Poland, several families with familial AVNRT (FAVNRT) were reported in Podkarpacie Province (PP).
Objectives: We aimed to determine the frequency of FAVNRT in PP compared with other south‑eastern provinces of Poland.
Patients and methods: Clinical data of 1544 patients with AVNRT diagnosed by invasive electrophysiological study between 2010 and 2019 were screened for FAVNRT. From January 2017 to June 2019, patients were asked to provide details on family history and origin to obtain 3‑generation pedigrees. Families with at least 2 members with previous CA of AVNRT were divided into those from south‑eastern provinces (SEPs; including PP and bordering provinces [BPs]) and the remaining parts of Poland (RPP).
Results: There were 932 patients from SEPs and 612 from RPP. FAVNRT was reported in 45 patients (2.91%) from 27 families, with a higher frequency in SEPs than RPP (4.02% vs 1.17%; P = 0.002) and the highest frequency in PP (6.33% vs 2.47% in BPs; P = 0.004). The risk of FAVNRT was higher in PP compared with BPs (odds ratio, 2.67; 95% CI, 1.36–5.23; P = 0.004) and similar in BPs compared with RPP (odds ratio, 2.14; 95% CI, 0.86–5.34; P = 0.1).
Conclusions: A relationship exists between the geographic region and frequency of FAVNRT. A greater distance from PP was associated with less frequent FAVNRT. International cooperation and genetic testing are needed to confirm the genetic impact of FAVNRT in this part of Central Europe.
Introduction
Atrioventricular nodal reentrant tachycardia (AVNRT) is one of the most common types of regular supraventricular tachycardia (SVT) in patients referred for catheter ablation (CA). The frequency of AVNRT in the general population is estimated at 1 in 1000 persons, while its probability in 2 family members reaches about 1 in 1 000 000 persons.1-4
In recent years, there have been several case reports of familial AVNRT (FAVNRT) and a single larger study reporting 24 families with FAVNRT.5 However, the largest population of FAVNRT identified on the basis of CA procedures was reported in south‑eastern Poland in Podkarpacie Province (PP)—15% of patients were family members (33 individuals from 13 families). Also, the largest 3‑generation family with the diagnosis of FAVNRT (6 individuals) identified to date originates from this region.6-12
The aim of this study was to assess the frequency of FAVNRT in PP in comparison with other regions of Poland.
Patients and methods
Data were collected from the multicenter CA registry Elektro and the prospective multicenter registry RareACare. Patients who underwent a CA procedure between January 2010 and December 2016 were asked about their family origin as well as family history of diagnosed arrhythmias or undiagnosed heart palpitations during the follow‑up (from January 2017 to June 2019) to establish if there were any signs of FAVNRT that occurred during the time period after ablation. Additionally, patients diagnosed with AVNRT by electrophysiological study (EPS) between January 2017 and December 2018 were asked about their family origin as well as family history of SVT symptoms or ablations. All CA procedures included in this analysis were performed in 11 centers in Poland, located in the following provinces: Mazovia (1 center), Podkarpacie (3 centers), Świętokrzyskie (3 centers), Lower Silesia (2 centers), and Małopolska (2 centers).
The families with a positive medical history of arrhythmia were divided into 3 groups: 1) with confirmed FAVNRT (at least 2 first‑degree relatives underwent a successful CA of AVNRT or had AVNRT confirmed by invasive EPS); 2) with highly probable FAVNRT (at least a single first‑degree relative underwent a successful CA of AVNRT or had AVNRT confirmed by invasive EPS, and at least one more family member had SVT on electrocardiography [ECG]); and 3) with probable FAVNRT (at least a single first‑degree relative underwent a successful CA of AVNRT or had AVNRT confirmed by invasive EPS, and at least one more family member had a history of undiagnosed heart palpitations). All included families were asked to specify their origin. Data on families with confirmed, highly probable, and probable FAVNRT were collected in the prospective RareACare registry. For all families, pedigree charts were drawn.
During the study, we also recorded other types of SVT that occurred in the families and included them in the pedigree charts (eg, AVNRT and orthodromic atrioventricular tachycardia in first‑degree relatives). In families with confirmed FAVNRT, long‑term ECG monitoring was recommended to each proband with undiagnosed palpitations.
The study was approved by the local ethics committee and complied with the Declaration of Helsinki. All patients provided written informed consent to participate in the study.
Electrophysiological study and catheter ablation
The earliest CA procedures were performed with a fluoroscopy approach with image acquisition set at 4 to 6 frames/s and with the patient placed in the left anterior oblique position. Since January 2012, a minimally invasive nonfluoroscopic imaging MINI CA protocol was used (no‑X‑ray, no‑lead apron, 2‑catheter approach).13-15
Typical or atypical AVNRT was diagnosed on the basis of previously described criteria.15,16
Statistical analysis
Differences in the frequency of FAVNRT between the regions of Poland were presented using 95% CIs. Logistic regression was used to examine the relationship between the geographic location of the provinces of Poland and the prevalence of FAVNTR. To express the increasing risk of FAVNRT associated with the proximity to Podkarpacie Province, we used a way of coding indicator variables proposed by Walter et al.17 The risk of FAVNRT depending on the location of provinces was expressed by means of odds ratio (OR). For descriptive statistics, means and SDs as well as percentages were calculated. A 2‑tailed standard P value of 0.05 was adopted as the level of significance. The analysis was performed with the Statistical Analysis System (version 9.4, SAS Institute, Cary, North Carolina, United States).
Results
A total of 1544 patients (mean [SD] age, 48.4 [16.2] years; women, 74.4%; children, 10.2%) underwent CA of AVNRT between 2010 and 2018. Among them, 45 patients (mean [SD] age, 38.1 [18.3] years; women, 68.9%; children, 17.7%) had first‑degree relatives with diagnosed AVNRT (27 families). Overall, FAVNRT was reported in 2.9% of the study population.
Patient origins
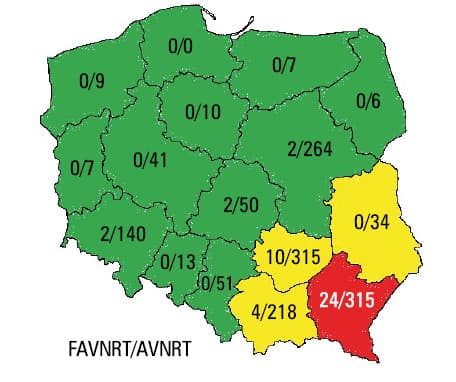
Patients originated from 15 of the 16 Polish provinces and from 7 other countries (Table 1). The most numerous group was from PP, with the largest number of families and family members with FAVNRT. In this province, 6.3% of patients were diagnosed with FAVNRT, followed by 3.2% of patients in Świętokrzyskie, 1.8% in Małopolska, 1.4% in Lower Silesia, and 0.8% in Mazovia Province. In the remaining provinces and countries (including Ukraine as the largest foreign population), no cases of FAVNRT were diagnosed (Figure 1).
Parameter | Total AVNRT population | FAVNRT | |||||
Study population, n (%) | Age, y, mean (SD) | Women, % | Patients, n | Families, n | Age, y, mean (SD) | Women, % | |
a Provinces in south‑eastern Poland
b Other provinces with cases of FAVNRT
Abbreviations: AVNRT, atrioventricular nodal reentrant tachycardia; FAVNRT, familial atrioventricular nodal reentrant tachycardia | |||||||
Polish province | |||||||
Total | 1544 (100) | 48.4 (16.2) | 74.4 | 45 | 27 | 38.1 (18.3) | 68.9 |
Lower Silesiaa | 140 (9.1) | 36.9 (17.6) | 78.6 | 2 | 1 | 25.5 (23.3) | 50.0 |
Kujawy‑Pomerania | 10 (0.7) | 37.7 (18.7) | 50.0 | – | – | – | – |
Łódźb | 50 (3.2) | 51.1 (15.3) | 72.0 | 2 | 1 | 3.5 (18.4) | 100 |
Lublina | 34 (2.2) | 44.4 (18.0) | 73.5 | – | – | – | – |
Lubuskie | 7 (0.5) | 28.5 (20.4) | 57.1 | – | – | – | – |
Małopolskaa | 218 (14.1) | 49.4 (16.4) | 69.7 | 4 | 2 | 43.5 (23.7) | 25.0 |
Mazoviab | 264 (17.1) | 49.3 (17.5) | 76.5 | 2 | 1 | 50.0 | |
Opole | 13 (0.8) | 29.1 (19.1) | 69.2 | – | – | – | – |
Podkarpaciea | 379 (24.6) | 47.4 (16.7) | 68.3 | 24 | 15 | 38.7 (19.3) | 62.5 |
Podlasie | 6 (0.4) | 38.2 (28.8) | 83.3 | – | – | – | – |
Silesia | 51 (3.3) | 34.3 (23.2) | 54.9 | – | – | – | – |
Świętokrzyskiea | 315 (20.4) | 49.5 (15.1) | 82.5 | 10 | 6 | 38.2 (18.2) | 90.0 |
Warmia‑Masuria | 7 (0.5) | 37.1 (20.10 | 57.1 | – | – | – | – |
Wielkopolska | 41 (2.7) | 46.3 (19.9) | 65.9 | – | – | – | – |
West Pomeraniab | 9 (0.6) | 41.4 (19.2) | 77.8 | 1 | 1 | – | 100 |
Other countries | |||||||
Total | 60 (100) | 50.2 (19.7) | 70 | – | – | – | – |
Ukraine | 53 (88.3) | 50.2 (19.4) | 67.9 | – | – | – | – |
Other countries | 7 (11.7) | 52.4 (17.0) | 85.7 | – | – | – | – |
Family pedigrees
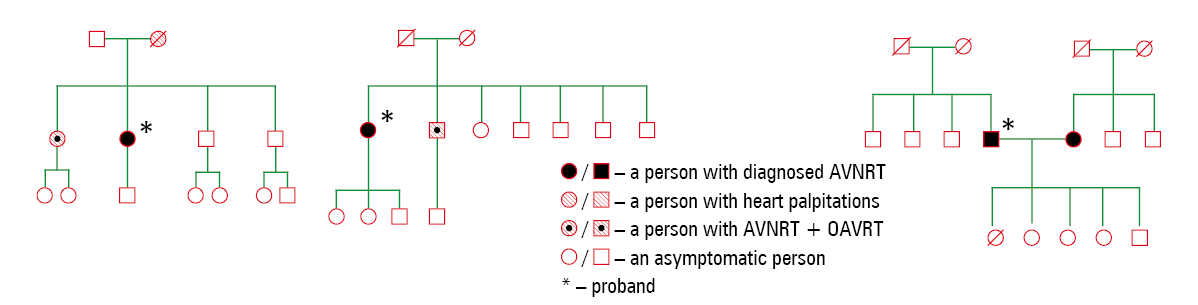
Patients were asked to contact their families to enquire if any of the family members underwent a CA of AVNRT in other electrophysiology centers. There were 45 such patients (mean [SD] age, 38.1 [18.3] years; women, 64%) from 27 families: 15 families with 24 members were from PP; 6 families with 10 members, from Świętokrzyskie; 2 families with 4 members, from Małopolska; and 2 families with 4 members from Mazovia and Lower Silesia Provinces each. For all families, pedigree charts were drawn (Figure 2). Additional pedigree charts were prepared for families in which FAVNRT was diagnosed before 2008 and that were still under observation at the time of the study (Figure 3); data on these patients are not included in the statistical analysis.
In 3 families we noted the phenomenon of a generation gap, with AVNRT absent in one generation and present in the previous and subsequent generations (Figure 2). To our knowledge, this is the first such finding reported in families with FAVNRT. Other family members with a history of heart palpitations remained under observation; however, no progression to fully symptomatic AVNRT was observed in any of those patients and none of them underwent ECG during heart palpitations.
Other forms of familial supraventricular tachycardia
During the study, 2 families were diagnosed with a different type of familial SVT, namely, AVNRT and orthodromic atrioventricular reentrant tachycardia (Figure 4A). Also, in one case, AVNRT was diagnosed in a husband and a wife from unconnected families (a “familial” nonfamilial form of AVNRT) (Figure 4B).
Families with highly probable FAVNRT
At the beginning of the study, 2 families were classified as having highly probable FAVNRT. In both cases, second‑degree relatives underwent EPS. In one case, FAVNRT was confirmed, and in the other, an incorrect diagnosis of sinus tachycardia was found, which led to the exclusion of this family from the group with highy probable FAVNRT.
Families with probable FAVNRT
Five families classified as having probable FAVNRT were under observation; however, none of the family members progressed from heart palpitations to fully symptomatic AVNRT and none of them underwent ECG during heart palpitations. Pedigree charts were drawn for all the families; all of them came from PP.
Frequency of FAVNRT in south‑eastern Poland
Of all the included patients, 932 originated from south‑eastern provinces (SEPs) of Poland (PP and the bordering provinces [BPs]: Lublin, Małopolska, and Świętokrzyskie) (Table 1), while 612 patients came from the remaining parts of Poland (RPP).
The frequency of FAVNRT was significantly higher in SEPs than in RPP (4.02% vs 1.17%; P = 0.002) and it was higher in PP than in BPs (6.33% vs 2.47%; P = 0.004). The frequency of FAVNRT in individual SEPs is presented in Table 2.
Province | Study population, n | Families with FAVNRT, n | Patients with FAVNRT, n | Frequency of FAVNRT, % | 95% CI |
Abbreviations: see Table 1 | |||||
Podkarpacie | 379 | 15 | 24 | 6.3 | 4–9.3 |
Lublin | 34 | 0 | 0 | 0 | 0–10.3 |
Małopolska | 218 | 2 | 4 | 1.8 | 0.5–4.6 |
Świętokrzyskie | 315 | 6 | 10 | 3.2 | 1.5–5.8 |
The risk of FAVNRT in south‑eastern Poland was assessed relative to other geographic regions. In SEPs, the risk was higher compared with RPP (OR, 3.53). It was also higher in PP than in BPs (OR, 2.67; 95% CI, 1.36–5.23; P = 0.004). The risk of FAVNRT was similar in BPs compared with RPP (OR, 2.14; 95% CI, 0.86–5.34; P = 0.1) (Table 3). The highest risk of FAVNRT was reported in PP.
Region | Frequency of FAVNRT, % | OR | 95% CI | P value |
a Lublin, Małopolska, and Świętokrzyskie Provinces
b BPs vs RPP
c PP vs BPs
Abbreviations: BPs, bordering provinces; OR, odds ratio; PP, Podkarpacie Province; RPP, remaining parts of Poland; ; others, see Table 1 | ||||
RPP | 1.17 | – | – | – |
BPsa | 2.47 | 2.14 | 0.86–5.34 | 0.1b |
PP | 6.33 | 2.67 | 1.36–5.23 | 0.004c |
In PP, the frequency of FAVNRT was the highest, while with the increase in the distance from the borders of this province towards Świętokrzyskie, Małopolska, and Lublin Provinces, the frequency of FAVNRT progressively decreased.
Discussion
To our best knowledge, this is the largest study reporting data on families with FAVNRT. It is also a study with the largest number of patients screened (retrospectively and prospectively) for the family history of AVNRT and the first one to include families with highly probable and probable FAVNRT under observation. Moreover, this is the first study conducted in Poland to determine the percentage of diagnosed FAVNRT among patients who underwent CA according to province.
Michowitz et al5 presented data of 1587 patients (614 men [40%]; mean [SD] age, 55 [19] years) who underwent ablation of AVNRT at the Tel Aviv Medical Center. The authors reported 24 families with FAVNRT. However, there was no information on the size and the origin of the families. Each family may have pedigree in others part of Israel and the rest of the word (including the PP region). In our study, according to Statistics Poland, 24 families with 50 members originated from a province with 2 128 687 inhabitants.18 However, the number of families was lower than that in the study by Michowitz et al.5 The families included in our study lived in cities and villages localized near 3 of the 6 electrophysiology centers in PP. Further studies including patient data from other electrophysiology centers as well as from the Polish National Health Fund are needed to fully determine the number of patients with FAVNRT.
Following single‑case reports, a study by Stec et al12 was the first to report a large percentage of patients with FAVNRT in PP. Our study shows that in other parts of southern Poland, there is still a higher percentage of reported FAVNRT compared with Israel and France (4% vs 2% vs 0.7%).5,10 Our study is the first to report a generation gap which may be related to recessive inheritance. In these 3 families, the genetic background behind this gap is still unclear. However, AVNRT can still occur in the future in the generation in which the gap was identified. Such families require more careful monitoring.4-12
Of note, our study showed that not only AVNRT but also other types of supraventricular arrhythmias can occur in first‑degree relatives, for example, AVNRT and orthodromic atrioventricular reentrant tachycardia. To our best knowledge, this has not been reported before.
Due to its rarity, AVNRT is unlikely to occur in 2 individuals that start a family with no genetic transmission to the offspring, such as in the case reported in our study (Figure 4B). To the best of our knowledge, this finding is reported for the first time in the literature.5-13 It confirms the hypothesis of a genetic determinant of FAVNRT because the frequency of this arrhythmia decreased with the increase in distance from the province with the highest prevalence.
So far, the genetic basis of FANVRT in each family remains unclear. However, there have been studies reporting genetic causes of AVNRT. In these studies, sodium and calcium channels as well as other genetic abnormalities were indicated as potentially responsible for the arrhythmia. In one study, 2 families with different genetic abnormalities were reported. It is possible that other undiagnosed genetic abnormalities, maybe involving the same genes in each family, were responsible for such a high frequency of FAVNRT cases in the PP region.19,20
Limitations
Our study has several limitations. Firstly, patients were recruited only from selected electrophysiology centers; therefore, not all families with FAVNRT from PP and BPs as well as RPP were included in this study; some cases might have been missed and the prevalence of FAVNRT in other regions of Poland might be underestimated. Furthermore, in large families, knowledge about the medical history (previous CA procedure, type of arrhythmia) may have been insufficient and some data may have been lost. Finally, arrhythmia may remain undiagnosed in patients with heart palpitations who present with mild or no symptoms.
Conclusions
There is a relationship between the geographic region and the frequency of FAVNRT. Distance from PP (the province with the highest prevalence of FAVNRT) was inversely correlated with FAVNRT frequency. International cooperation and genetic testing are required to confirm the genetic impact of FAVNRT in this part of Central Europe. To begin with, several families with FAVNRT from Podkarpackie, Małopolska, and Świętokrzyskie Provinces will be tested to identify the genetic basis of this phenomenon. Based on the genetic material collected from the families, further genetic tests will be done to explain the heredity of AVNRT.
- Katristis DG, Josephson ME. Classification of electrophysiological types of atrioventricular nodal re‑entrant tachycardia: a reappraisal. Europace. 2013; 15: 1231‑1240. | Crossref
- Gil‑Ortega I, Pedrote‑Martínez A, Fontenla‑Cerezuela A; Spanish Catheter Ablation Registry collaborators. Spanish catheter ablation registry. 14th Official report of the Spanish Society of Cardiology Working Group on Electrophysiology and Arrhythmias (2014). Rev Esp Cardiol (Engl Ed). 2015; 68: 1127‑1137.
- Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS Guideline for the management of adult patients with supraventricular tachycardia: a report of the American College of Cardiology / American Heart Association task force on clinical practice guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2016; 5: 27‑115.
- Brugada J, Katritsis DG, Arbelo E, et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardia. The Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J. 2020; 41: 655‑720.
- Michowitz Y, Anis‑Heusler A, Reinstein E, et al. Familial occurrence of atrioventricular nodal reentrant tachycardia. Circ Arrhythm Electrophysiol. 2017; 10: e004680. | Crossref
ARTICLE INFORMATION