Optimal medical therapy in patients with stable coronary artery disease in Poland: the ISCHEMIA trial experience
Key words: cardiovascular risk factors, optimal medical therapy, stable coronary artery disease



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Optimal medical therapy in patients with stable coronary artery disease in Poland: the ISCHEMIA trial experience
Introduction: Optimal medical therapy (OMT) is the cornerstone of treatment for stable coronary disease with the ISCHEMIA trial showing similar outcomes using OMT with or without an initial invasive approach.
Objectives: To describe OMT goal attainment in Polish ISCHEMIA participants compared with other countries.
Patients and methods: Among 5179 trial participants, 333 were randomized in Poland. The median follow‑up was 3.2 years. OMT targets were: not smoking, high‑intensity statin therapy, low‑density lipoprotein cholesterol (LDL‑C) of less than 70 mg/dl, systolic blood pressure of less than 140 mm Hg, aspirin therapy, and ACEI / ARB, and β-blocker therapy if indicated.
Results: Compared with 36 other countries, at randomization, patients in Poland were older (67 [62–75] y vs 65 [58–71] y); P <0.001), more often female (30% vs 22%; P = 0.002), with a longer history of angina (3 [1–9] y vs 1 [0–3] y; P <0.001), and there were more cases of prior myocardial infarction (32% vs 18%; P <0.01) and revascularization (PCI, 40% vs 19%; CABG, 11% vs 3%; P <0.001 for both). The number of OMT goals attained increased from baseline to follow‑up visits (5 [4–5] vs 6 [5–6]; P <0.001) in Poland and other countries alike (P = 0.89 vs P = 0.14). In Poland, significant improvements were achieved regarding high‑intensity statin therapy (27% vs 50%), LDL‑C <70 mg/dl (29% vs 65%), and systolic blood pressure of less than 140 mm Hg (63% vs 81%) (P <0.001 for all), whereas not‑smoking (89% vs 89%), aspirin (90% vs 88%), ACEI / ARB (93% vs 95%), and β-blocker therapy (94% vs 90%) remained high.
Conclusions: With regular surveillance and contemporary medical therapy, high OMT goal attainment was achievable among the participants of the ISCHEMIA trial in Poland relative to other countries. There is still room for improvement in LDL‑C and blood pressure management.
What's new?
Optimal medical therapy (OMT) has been the cornerstone of treatment in patients with stable coronary artery disease; however, its proper application remains challenging. Herein, a snapshot of OMT patterns is presented in participants of the ISCHEMIA trial from Poland in comparison with other countries worldwide at the time of their randomization into the trial and at the last follow‑up visit. It demonstrates the achievable level of OMT goal attainment with the use of contemporary treatment methods and multifaceted, team efforts. In particular, significant improvements were achieved regarding high‑intensity statin therapy, low‑density lipoprotein cholesterol levels of less than 70 mg/dl, and systolic blood pressure of less than 140 mm Hg. Although such a high level of goal attainment sets a benchmark for OMT, there is still space for further improvement with introduction and timely adoption of novel treatment methods.
Introduction
Management of patients with stable coronary artery disease (CAD) aims at cardiovascular event risk reduction and symptom relief. Optimal medical therapy (OMT) consisting of lifestyle changes, cardiovascular risk factor control, and medication adherence has been the mainstay of treatment this population.1 Coronary revascularization has been reserved mainly for patients with documented myocardial ischemia or persistent symptoms despite OMT. While the prognostic gains of goal‑directed OMT are indubitable, those of coronary revascularization remain under discussion.1-3 The recent multinational ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial did not demonstrate prognostic benefits of early coronary catheterization and revascularization, where feasible, in patients with stable CAD and at least moderate ischemia on noninvasive stress testing. In that trial, OMT was the major focus, regardless of the randomized strategy assignment. A high level of OMT goal attainment requires long‑term, multidisciplinary efforts which, as shown by registry data and randomized clinical trials, may be difficult to achieve.4 Concerns about the status of OMT in patients with stable CAD have also been voiced with regard to the Polish healthcare system.5,6
The ISCHEMIA trial gives a unique opportunity to take a glimpse at the patterns of OMT in high‑risk patients with stable CAD in Poland at the time of randomization into the study and learn what OMT standards are achievable in a controlled environment such as that of a clinical trial with the use of widely available, contemporary, guideline‑directed treatment methods.
The aim of this study was to present OMT goal attainment in the participants of the ISCHEMIA trial randomized in Poland in comparison with those in other countries worldwide.
Patients and methods
The ISCHEMIA trial
The current study is the analysis of the ISCHEMIA trial (ClinicaLtrials.gov identifier: NCT01471522). The detailed rationale and design of the trial as well as its results have been published previously.7‑10 In brief, the trial enrolled patients with stable CAD, at least moderate ischemia on stress testing, and obstructive CAD, with the exclusion of left main stenosis of 50% or greater. Patients were randomized to one of the 2 treatment strategies: 1) an initial invasive strategy of cardiac catheterization and optimal revascularization, if feasible, in addition to OMT, and 2) an initial conservative strategy of OMT alone, with catheterization reserved for failure of OMT.
OMT was advised in keeping with concurrent medical practice guidelines with updates considered when the guidelines changed during the trial. Efforts were made to keep a high level of OMT equally in both arms of the study. The trial was approved by institutional ethics committees and all study participants gave informed consent to participate in the study.
Optimal medical therapy goals
There were the following 7 main OMT goals: 1) not smoking; 2) high‑intensity statin therapy (atorvastatin, 40–80 mg or rosuvastatin, 20–40 mg); 3) low‑density lipoprotein cholesterol (LDL‑C) levels of less than 70 mg/dl; 4) systolic blood pressure (SBP) of less than 140 mm Hg; 5) aspirin therapy; 6) use of an angiotensin‑converting enzyme inhibitor (ACEI) / angiotensin receptor blocker (ARB) in patients with hypertension, diabetes, estimated glomerular filtration rate of less than 60 ml/min, or left ventricular ejection fraction of less than 40%; 7) use of a β-blocker in patients with a history of myocardial infarction or left ventricular ejection fraction of less than 40%. The achievement of OMT goals was reinforced by encouraging collaboration among the site study team and the participants’ personal physician. Study teams were trained to provide lifestyle counseling regarding smoking cessation, nutrition, physical activity, and medication adherence. Pedometers were offered to study participants to encourage regular exercise. Dedicated ISCHEMIA algorithms were introduced to site teams that outlined recommended lipid lowering and blood pressure therapy. A Clinical Coordinating Center Risk Factor Management Team oversaw OMT goal attainment progress at all sites globally, provided monthly site‑specific OMT reports to study teams, and used various communication methods to encourage medical therapy optimization, such as investigator meetings, webinars, monthly newsletters, emails, dedicated phone calls with study site teams, in‑person meetings with individual investigators to review participant‑level data and provide specific feedback. Participants were provided cards and key tags that list the risk factor goals.
Patients were followed‑up at 1.5, 3, 6, and 12 months after randomization and every 6 months thereafter until the trial ended. In‑clinic visits were recommended and if not feasible, visits by phone and by proxy were allowed. All of the above ISCHEMIA trial–specific recommendations and measures to attain OMT goals were equivalent for Poland and other countries. All sites participating in the trial were selected according to the site selection criteria presented previously with the ISCHEMIA trial rationale and design.7
In the current analysis, OMT goal attainment of participants randomized in Poland were compared with all other countries at 2 timepoints in the trial: 1) the randomization visit; 2) the last follow‑up visit. The assessment of change in OMT goal attainment between the randomization and last follow‑up visits was also performed in the subgroup of study participants randomized in Poland.
Statistical analysis
We summarized categorical and continuously measured baseline participant characteristics using frequencies with percentages and medians with interquartile ranges (IQRs), respectively. Characteristics of Polish participants and those from the rest of the world were compared using the χ2 test for categorical variables, and the Kruskal–Wallis for continuous variables. For 2‑by‑2 comparisons involving expected cell counts less than 5, we used the Fisher exact test. To assess changes between baseline and follow‑up among Polish participants, we used paired sample tests, with exact tests for symmetry for categorical variables, and the Wilcoxon matched‑pairs signed‑ranks test for continuous variables. For the number of OMT goals, to handle zero cell counts, categories 0 to 3 goals, 4 goals, 5 goals, and 6 to 7 goals were constructed. We assessed statistical significance using a type 1 error rate of 0.05. All analyses were conducted in R statistical software (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline characteristics
There was a total of 333 ISCHEMIA trial participants randomized in Poland versus 4846 participants randomized in the remaining 36 countries across 5 continents worldwide as listed in Supplementary material, Table S1. The median time from randomization to last follow‑up visit was 3.2 years (3.84 years for participants in Poland vs 3.19 years for participants in other countries; P <0.001). The comparison of baseline patient characteristics between the 2 groups is presented in Table 1. Compared with other countries, ISCHEMIA participants in Poland were older (67 vs 65 years), more often female (30% vs 22%) and White (99% vs 64%), with a greater frequency of hypertension (88% vs 72%), former smoking (57% vs 44%), prior myocardial infarction (32% vs 18%), prior coronary revascularization (51% vs 22%), atrial fibrillation / flutter (12% vs 4%), and peripheral vascular disease (8% vs 4%), presented with more anginal symptoms and longer duration of angina as evidenced by Canadian Cardiovascular Society Angina Score and Seattle Angina Questionnaire. (Table 1).
Characteristics | Poland (n = 333) | Other countries (n = 4846) | P value | |
Data are presented as number of patients / total number of patients (percentage) unless otherwise indicated.
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin receptor blocker; BMI, body mass index; CABG, coronary artery bypass grafting; CCS, Canadian Cardiovascular Society Angina Score; DBP, diastolic blood pressure; HbA1c, glycated hemoglobin A1c; IQR, interquartile range; LDL‑C, low‑density lipoprotein cholesterol; MI, myocardial infarction; NYHA, New York Heart Association functional classification; OMT, optimal medical therapy; PCI, percutaneous coronary intervention; SAQ, Seattle Angina Questionnaire; SBP, systolic blood pressure | ||||
Age, y, n; median (IQR) | 333; 67 (62–75) | 4846; 65 (58–71) | <0.001 | |
Female sex | 99/333 (30) | 1069/4846 (22) | 0.002 | |
White race | 329/333 (99) | 3074/4796 (64) | <0.001 | |
Hypertension | 290/331 (88) | 3499/4830 (72) | <0.001 | |
Diabetes | 133/333 (40) | 2031/4846 (42) | 0.52 | |
Prior MI | 108/333 (32) | 883/4829 (18) | <0.001 | |
Smoking status | Never smoked | 108/333 (32) | 2100/4841 (43) | <0.001 |
Former smoker | 189/333 (57) | 2137/4841 (44) | ||
Current smoker | 36/333 (11) | 604/4841 (12) | ||
Reduced ejection fraction | ≥45% | 315/332 (95) | 4638/4842 (96) | 0.52 |
<45% | 17/332 (5) | 204/4842 (4) | ||
Atrial fibrillation / flutter | 40/333 (12) | 181/4840 (4) | <0.001 | |
Prior carotid surgery or stent | 14/333 (4) | 149/4839 (3) | 0.33 | |
Prior stroke | 12/333 (4) | 139/4845 (3) | 0.55 | |
Prior peripheral vascular disease | 25/333 (8) | 179/4835 (4) | 0.001 | |
Prior coronary revascularization PCI | 132/333 (40) | 918/4842 (19) | <0.001 | |
Prior coronary revascularization CABG | 37/333 (11) | 166/4846 (3) | <0.001 | |
CCS | None | 31/333 (9) | 1004/4844 (21) | <0.001 |
I | 60/333 (18) | 1329/4844 (27) | ||
II | 211/333 (63) | 2311/4844 (48) | ||
III | 31/333 (9) | 199/4844 (4) | ||
IV | 0/333 | 1/4844 | ||
NYHA | I | 78/186 (42) | 921/1830 (50) | 0.04 |
II | 108/186 (58) | 909/1830 (50) | ||
III | 0/186 | 0/1830 | ||
IV | 0/186 | 0/1830 | ||
SAQ angina frequency score, n; median (IQR) | 331; 80 (70–100) | 4316; 90 (70–100) | 0.09 | |
SAQ physical limitation score, n; median (IQR) | 312; 75 (58–92) | 3994; 83 (67–100) | <0.001 | |
SAQ quality of life score, n; median (IQR) | 331; 50 (38–75) | 4310; 63 (38–88) | 0.001 | |
Duration of angina, y, n; median (IQR) | 297; 3 (1–9) | 3981; 1 (0–3) | <0.001 | |
Degree of ischemia on stress testing | None or mild | 74/327 (23) | 532/4778 (11) | <0.001 |
Moderate or severe | 253/327 (77) | 4246/4778 (89) | ||
OMT | ||||
Number of the main 7 OMT goals met, n; median (IQR) | 243; 5 (4–6) | 3346; 5 (4–6) | 0.89 | |
“No smoking” goal met | 297/333 (89) | 4237/4841 (88) | 0.42 | |
“On high‑intensity statin” goal met | 80/301 (27) | 1831/4639 (39) | <0.001 | |
“LDL‑C <70 mg/dl” goal met | 95/329 (29) | 1526/4611 (33) | 0.13 | |
“SBP <140 mm Hg” goal met | 210/332 (63) | 3150/4818 (65) | 0.47 | |
“On aspirin” goal met | 301/333 (90) | 4552/4842 (94) | 0.01 | |
“On ACEI / ARB” goal met | 282/302 (93) | 2836/3986 (71) | <0.001 | |
“On β-blocker” goal met | 103/110 (94) | 805/913 (88) | 0.12 | |
Other OMT characteristics | ||||
On antiplatelet therapy | 303/333 (91) | 4569/4842 (94) | 0.02 | |
On anticoagulants | 37/332 (11) | 166/4799 (3) | <0.001 | |
On antiplatelet or anticoagulant | 326/333 (98) | 4652/4842 (96) | 0.13 | |
On ACEI / ARB | 303/333 (91) | 3113/4840 (64) | <0.001 | |
On β-blockers | 295/333 (89) | 3866/4840 (80) | <0.001 | |
On calcium channel blockers | 103/110 (94) | 805/913 (88) | 0.12 | |
On statins | 321/333 (96) | 4583/4841 (95) | 0.21 | |
On ezetimibe | 8/333 (2) | 204/4842 (4) | 0.14 | |
On other hypolipidemic medications | 1/333 | 36/4842 (1) | 0.73 | |
HbA1c <7% | 122/170 (72) | 2159/3269 (66) | 0.15 | |
SBP <30 mm Hg and DBP <90 mm Hg | 116/332 (35) | 1919/4818 (40) | 0.09 | |
BMI, kg/m2, n; median (IQR) | 330; 29 (26–32) | 4794; 28 (25–31) | <0.001 | |
Baseline optimal medical therapy goal attainment
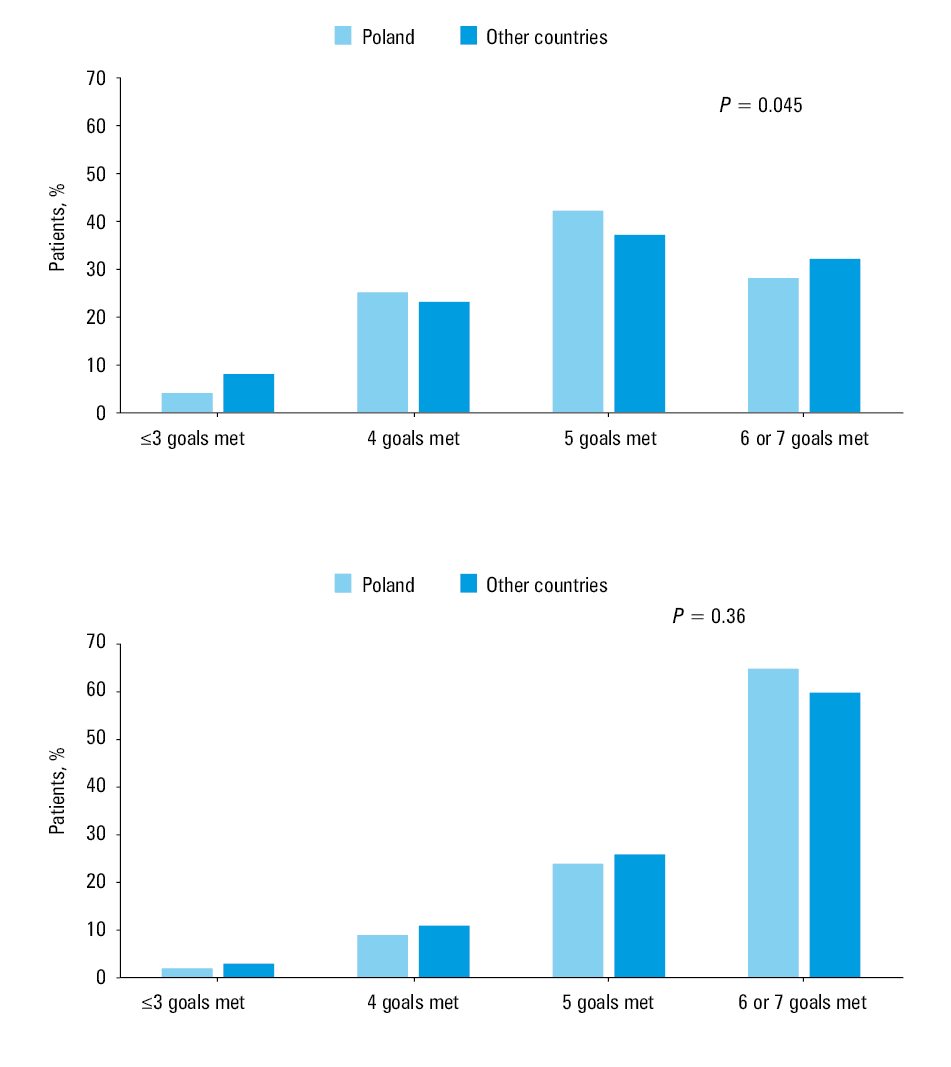
The median number of the 7 main OMT goals attained at randomization was 5, similarly in Poland and the rest of the world (P = 0.89). The distribution of the number of OMT goals achieved is presented in Figure 1A. Compared with other countries, participants in Poland received less high‑intensity statin therapy (27% vs 39%), but more ACEI / ARB treatment (93% vs 71%) (P <0.0001 for both). The 2 groups had similarly suboptimal results with regard to the attainment of LDL‑C levels of less than 70 mg/dl and blood pressure of less than 140 mm Hg (29% vs 33% and 63% vs 65%, respectively; P = 0.13 and P = 0.47, respectively).
Follow‑up optimal medical therapy goal attainment
The median number of the main OMT goals met increased from 5 at baseline to 6 at the last follow‑up visit (P <0.001), similarly in Poland and other countries (Table 2). The distribution of the number of OMT goals achieved is presented in Figure 1B.
OMT | Poland (n = 333) | Other countries (n = 4846) | P value |
Data are presented as number of patients / total number of patients (percentage) unless otherwise indicated.
Abbreviations: see Table 1 | |||
Number of the 7 OMT goals met, n; median (IQR) | 264; 6 (5–6) | 3346; 6 (5–6) | 0.14 |
“No smoking” goal met | 282/316 (89) | 4080/4513 (90) | 0.56 |
“On high‑intensity statin” goal met | 159/321 (50) | 3014/4674 (64) | <0.001 |
“LDL‑C <70 mg/dl” goal met | 208/318 (65) | 2661/4565 (58) | 0.02 |
“SBP <140 mm Hg” goal met | 259/321 (81) | 3559/4641 (77) | 0.12 |
“On aspirin” goal met | 282/321 (88) | 4363/4676 (93) | <0.001 |
“On ACEI / ARB” goal met | 279/293 (95) | 2801/3840 (73) | <0.001 |
“On β-blocker” goal met | 95/106 (90) | 744/889 (84) | 0.15 |
Other OMT characteristics | |||
On antiplatelet | 282/321 (88) | 4381/4676 (94) | <0.001 |
On anticoagulant | 41/321 (13) | 301/4671 (6) | <0.001 |
On ACEI / ARB | 300/321 (93) | 3169/4675 (68) | <0.001 |
On antiplatelet or anticoagulant | 310/321 (97) | 4535/4677 (97) | 0.83 |
On β-blockers | 291/321 (91) | 3703/4675 (79) | <0.001 |
On calcium channel blockers | 141/321 (44) | 1675/4677 (36) | 0.01 |
On statins | 308/321 (96) | 4447/4676 (95) | 0.58 |
On ezetimibe | 77/321 (24) | 1145/4677 (24) | 0.90 |
On other hypolipidemic medications | 1/333 | 36/4842 (1) | 0.73 |
HbA1c <7% | 153/211 (73) | 2437/3578 (68) | 0.21 |
SBP <130 mm Hg and DBP <90 mm Hg | 162/321 (50) | 2351/4641 (51) | 0.99 |
BMI, kg/m2, n; median (IQR) | 319; 28 (26–31) | 4576; 27 (25–31) | <0.001 |
In particular, in Poland, an improvement was observed regarding the use of high‑intensity statin therapy (27% vs 50%), LDL‑C levels of less than 70 mg/dl (29% vs 65%) and SBP of less than 140 mm Hg (63% vs 81%) (P <0.001 for all). The frequency of other main OMT goals met remained similarly high. Ezetimibe use increased from 2% at randomization to 24% at the last follow‑up visit (P <0.001) (Table 3).
OMT | Baseline (n = 333) | Follow‑up (n = 333) | P value |
Data are presented as number of patients / total number of patients (percentage) unless otherwise indicated.
Abbreviations: NA, not applicable ; others, see Table 1 | |||
Number of the 7 OMT goals met, n; median (IQR) | 243; 5 (4–6) | 264; 6 (5–6) | <0.001 |
“No smoking” goal met | 297/333 (89) | 282/316 (89) | 1.00 |
“On high‑intensity statin” goal met | 80/301 (27) | 159/321 (50) | <0.001 |
“LDL‑C <70 mg/dl” goal met | 95/329 (29) | 208/318 (65) | <0.001 |
“SBP <140 mm Hg” goal met | 210/332 (63) | 259/321 (81) | <0.001 |
“On aspirin” goal met | 301/333 (90) | 282/321 (88) | 0.24 |
“On ACEI / ARB” goal met | 282/302 (93) | 279/293 (95) | 0.26 |
“On β-blockers” goal met | 103/110 (94) | 95/106 (90) | 0.42 |
Other OMT characteristics | |||
On antiplatelet | 303/333 (91) | 282/321 (88) | 0.12 |
On anticoagulant | 37/332 (11) | 41/321 (13) | 0.19 |
On antiplatelet or anticoagulant | 326/333 (98) | 310/321 (97) | 0.42 |
On ACEI / ARB | 303/333 (91) | 300/321 (93) | 0.15 |
On β-blockers | 295/333 (89) | 291/321 (91) | 0.35 |
On calcium channel blockers | 119/333 (36) | 141/321 (44) | 0.004 |
On statins | 321/333 (96) | 308/321 (96) | 0.79 |
On ezetimibe | 8/333 (2) | 77/321 (24) | <0.001 |
On other hypolipidemic medications | 1/333 | 1/333 | NA |
HbA1c <7% | 122/170 (72) | 153/211 (73) | 0.22 |
SBP <130 mm Hg and DBP <90 mm Hg | 116/332 (35) | 162/321 (50) | <0.001 |
BMI, kg/m2, n; median (IQR) | 330; 29 (26–32) | 319; 28 (26–31) | 0.002 |
Of note, compared with other countries, Poland achieved higher LDL‑C goal attainment (65% vs 58%; P = 0.02) with a lower frequency of high‑intensity statin therapy (50% vs 64%; P <0.001). The frequency of ACEI / ARB for specific indications remained higher in Poland as compared with other countries (95% vs 73%; P <0.001). There was a slightly lower frequency of aspirin use in Poland (88% vs 94%; P <0.001), however, with greater prevalence of atrial fibrillation and long‑term anticoagulation (Table 2).
Discussion
This analysis aimed to describe OMT goal attainment in high‑risk patients with stable CAD who were randomized to the ISCHEMIA trial in Poland in comparison with the trial participants randomized in other countries worldwide. Overall, despite being burdened with more cardiovascular risk factors, greater frequency of prior myocardial infarction, more prior coronary revascularization procedures, and longer duration of angina, study participants in Poland did not differ regarding the median number of OMT goals met at randomization. In particular, they presented with similarly low LDL‑C and blood pressure goal attainment, with less frequency of high‑intensity statin but more ACEI/ARB use. At the last follow‑up visit, the median number of OMT goal attainment improved similarly in patients randomized in Poland and other countries.
Low‑density lipoprotein cholesterol goal
Over the median 3.8 years of follow‑up, a significant improvement was achieved regarding LDL‑C levels of less than 70 mg/dl goal (from 29% to 65% of patients at goal), where Poland topped other countries. Although with significant increments, the percentage of high‑intensity statin use in Poland remained inferior. It is noteworthy that 4% of patients in Poland did not receive any statin with similar numbers noted in other countries. Given high attention paid to statin therapy in the trial, lower numbers would probably be difficult to achieve. At the same time, ezetimibe use increased from 2% to 24%, which together with the increase in high‑intensity statin use translated into the reported significant gain in LDL‑C levels of less than 70 mg/dl. Novel lipid lowering drugs were by and large not used in the ISCHEMIA trial participants, and with the LDL‑C threshold being already shifted downwards in the highest–risk population with CAD, policies to make these therapies available to wider groups of patients should urgently be implemented.1,11 As part of the European Society of Cardiology (ESC) EURObservational Research Programme (EORP), the EUROASPIRE V (European Action on Secondary and Primary Prevention by Intervention to Reduce Events) survey was carried out from 2016 to 2017. A total of 7575 patients from 27 countries were enrolled 6 to 24 months (median, 1.12 years) after a hospitalization for CABG or PCI in the setting of chronic CAD or acute coronary syndrome.12 In EUROAPSIRE V, the percentage of patients who achieved LDL‑C level of less than 1.8 mmol/l (70 mg/dl) was as low as 29% (31.2% of 202 survey participants from Poland), with 13.9% of the cohort remaining without any lipid lowering therapy (9.7% among 402 participants from Poland) and 49.9% treated with high‑intensity statin (58.5% among 400 participants from Poland).12 Furthermore, only 55% of the EUROASPIRE V population were discharged on a high‑intensity statin. At the time of the follow‑up survey, 2.7% were on a high‑intensity statin and ezetimibe combination. A more recently published POLASPIRE survey included 1148 patients in Poland and applied a very similar methodology to the EUROASPIRE V registry. In the POLASPIRE cohort, 5.6% of patients did not receive any lipid lowering medication at hospital discharge with the percentage increasing to 9.7% at the median 1‑year follow‑up. At the time of survey, only 38% reached LDL‑C target of 1.8 mmol/l, with 2.5% receiving ezetimibe.5
Blood pressure goal
There was a significant improvement in SBP at target (from 63% to 81%) over the follow‑up, with similar progress made in other countries. In ISCHEMIA, the target for optimal blood pressure changed during the trial when the respective American guidelines changed the SBP goal from less than 140 mm Hg to less than 130 mm Hg.13 Accounting for the lower thresholds, the percentage of patients with blood pressure at target in Poland was only 50% at the last follow‑up visit compared with 81% with the original target of 140 mm Hg. Although the numbers were much better compared with those from the EUROASPIRE V cohort, where only 29% achieved blood pressure of less than 130/80 mm Hg and 68% of less than 140/90 mm Hg, they should still trigger a call for further improvement regarding optimal blood pressure control in high‑risk patients with CAD.15
Other optimal medical therapy targets
While reading the median numbers of OMT goal attainment, it is important to note that the 7 OMT targets included aspirin use. The percentage of aspirin use remained inferior in Poland. However, with significantly greater frequency of AF among the trial participants in Poland, many patients remained on oral anticoagulation without antiplatelet therapy. Such treatment is in line with the current ESC guidelines2 and when accounted for, the same number of patients were receiving antiplatelet therapy and / or antigoaculation in both groups.
There was a high percentage of ACEI / ARB use in Poland at last follow‑up, superior to other countries. This finding was consistent with the results of the European CLARIFY (Prospective Observational Longitudinal Registry of Patients With Stable Coronary Artery Disease) registry.14 β-Blocker and nonsmoking goals were met in the great majority of study participants at both time periods in both groups. There was only a marginal improvement in patients with diabetes and glycated hemoglobin A1c (from 72% to 73% in Poland, and 66% to 68% in other countries) which might indicate the need for closer collaboration with diabetologists in efforts to further improve glycemic control in patients with CAD. However, the percentage is much better compared with the EUROASPIRE V survey, in which only 54% presented with glycated hemoglobin A1c levels of less than 7%.15
Summary and perspective
In general, the results of the current analysis illustrate that with a structured, multidisciplinary effort, the achievable level of OMT goal attainment is outstanding compared with that of the recently reported “real‑world” settings of the European healthcare systems, Poland included. The causes underlying this undertreatment are multiple, but efforts are urgently due to identify them and implement strategies to address them on national and international levels. Data such as presented herein may help provide guidance to the policy makers ranging from central and local national authorities, through medical associations to patient groups. This is to optimize and fully implement resources and tools that are readily available, with proven efficacy and safety, with the Polish participants of the ISCHEMIA trial setting a benchmark of what is possible. At the same time, novel treatment methods are needed to make the OMT targets within reach to all patients with CAD, also those who fail to achieve goals despite maximally titrated OMT as well as those who do not tolerate standard treatment due to side effects or remain on the outskirts of the state‑of‑the‑art OMT for economic, logistic, or educational reasons.
Limitations
This is a descriptive study and the comparisons were not adjusted for differences in baseline patients’ characteristics; however, the trial enrollment criteria deemed the study population similar and all baseline differences between the groups have been reported and can be considered by the readers in data interpretation. In line with the ISCHEMIA trial policies, we did not report country‑specific patient outcomes in this study. Due to the sample size limitations, analyses of subgroups depending on the randomized strategy assignment or other subgroup analyses were not performed. The reported level of OMT goal attainment was achieved across ISCHEMIA sites during the trial and thus is not representative of daily clinical practice. Data for changes in diet and physical activity were not available.
Conclusions
In conclusion, with regular surveillance and contemporary medical therapy, high OMT goal attainment was achievable among ISCHEMIA participants in Poland relative to other countries. There is still room for improvement regarding lipids and blood pressure management.
- Knuuti J, Wijns W, Saraste A, et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020; 41: 407‑477.
- Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016; 37: 2315‑2381.
- Navarese EP, Lansky AJ, Kereiakes DJ, et al. Cardiac mortality in patients randomised to elective coronary revascularisation plus medical therapy or medical therapy alone: a systematic review and meta‑analysis. Eur Heart J. 2021 May 18. [Epub ahead of print]. | Crossref
- Kotseva K, Wood D, De Bacquer D, et al. EUROASPIRE IV: a European Society of Cardiology survey on the lifestyle, risk factor and therapeutic management of coronary patients from 24 European countries. Eur J Prev Cardiol. 2016; 23: 636‑648.
- Jankowski P, Kosior DA, Sowa P, et al. Secondary prevention of coronary artery disease in Poland. Results from the POLASPIRE survey. Cardiol J. 2020; 27: 533‑540. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION