Health risks of dual use of electronic and combustible cigarettes: exposure to acrylamide and glycidamide
Key words: acrylamide, cigarette, e-cigarette, glycidamide, National Health and Nutrition Examination Survey



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Health risks of dual use of electronic and combustible cigarettes: exposure to acrylamide and glycidamide
Introduction: A combustible cigarette is a significant source of acrylamide, which is associated with numerous adverse effects. Electronic cigarette (e‑cigarette) is an emerging smoking device with uncertain health effects.
Objectives: The aim of the study was to explore the exposure risks of acrylamide (AA) by measuring biomarkers, hemoglobin adducts of AA (HbAA) and of glycidamide (HbGA), in serum samples of the general adult population with regard to different smoking status (smoking vs nonsmoking).
Patients and methods: This was a cross‑sectional study of 1657 participants aged 18 years or older from the United States National Health and Nutrition Examination Survey (2015–2016) with recorded patient smoking status and concentrations of HbAA and HbGA. Multivariable linear regression models were used to analyze HbAA and HbGA in different smoking groups (nonsmokers, cigarettes smoking only, e‑cigarettes smoking only, and dual users).
Results: Dual users had the highest HbAA and HbGA concentrations (median [interquartile range], 83.75 [53.28–128.25] pmol/gHb and 61.20 [40.73–89.78] pmol/gHb, respectively). There was a positive association between the use of e‑cigarettes and the HbAA concentration. The standardized β coefficients of HbAA and HbGA between the combustible cigarette smokers and nonsmokers in the fully adjusted model were 0.312 and 0.255 (both P <0.001) and those between the dual users and nonsmokers in the fully adjusted model were 0.396 and 0.342, respectively (both P <0.001).
Conclusions: E‑cigarette users are exposed to AA, and users of both combustible and e‑cigarettes have highest measures of HbAA and HbGA. Aside from the adverse effects caused by e‑cigarette smoking, coexposure risks of combustible cigarettes and e‑cigarettes need to be communicated to the public. Further studies are warranted to aid in health promotion.
What's new?
At present, adverse events associated with the use of electronic cigarettes (e‑cigarettes) have been recognized by public health. In our research, we first explored the effects of e‑cigarettes use on acrylamide exposure with valid biomarkers, hemoglobin‑adducted acrylamide and hemoglobin‑adducted glycidamide. In addition, we analyzed the level of these biomarkers in patients of varying smoking status. More than 70% of e‑cigarette users are dual users. Compared with combustible cigarette smokers and e‑cigarette smokers, there is a stronger correlation between biomarkers and smoking habits in dual users. This indicates that coexposure to combustible cigarettes and e‑cigarettes increases the health hazards associated with exposure to acrylamide.
Introduction
Acrylamide (AA) is a water‑soluble vinyl monomer, which can be produced during cooking of certain foods and is a product of tobacco smoking. The monomer AA is easily polymerized into polypropylene amide. Polypropylene amide is a chemical raw material used in many industries, such as anti‑leakage agents, adhesives, and dyes. AA has also been found in baked and fried carbohydrate‑rich foods, such as french fries, potato chips, breads, and cereals. It is produced by the Maillard browning reaction by reducing sugars and amino acids, asparagine in particular, in food when cooked at high temperatures (>120 °C). AA is metabolized by 2 main pathways: glutathione conjugation and epoxidation to glycidamide (GA).1 The epoxidation reaction to GA is catalyzed by CYP2E1 in rodents. Both AA and GA react with hemoglobin, producing a stable adduct, which can be measured as an indicator of exposure.2 Finally, the metabolites are excreted in the urine in the form of mercapturic acid (AAMA and GAMA) within 24 hours.3,4
AA can be harmful and possible toxic effects include neurotoxicity, reproductive toxicity, genotoxicity, and carcinogenicity. Exposure to AA can induce central and peripheral neuropathy in the human nervous system and lead to nerve paralysis and ataxia symptoms. It has been found that in rodents exposed to higher doses, sperm cell type and motility were affected and neurological symptoms developed, which all lead to a decrease in mating frequency and the number of young rats born.5 A previous study disclosed that AA exposure decreased cell viability and increased excessive oxidative stress and apoptosis in Leydig and Sertoli cells.6
After the cells were treated with AA or GA, DNA bonds were produced, leading to more A→G transitions and G→C transversions. Furthermore, cells treated with GA had more G→T transversions (P <0.001). It was found that the gene mutagenic ability of AA is weak, but the ability to cause chromosome breakage is strong. However, its metabolite (GA) is a potent mutagen and a strong chromosome‑disrupting agent in vitro.7 The International Agency for Research on Cancer lists AA as a 2A carcinogen (probable human carcinogen), defined as limited or insufficient epidemiological evidence, plus sufficient animal experimental evidence. Some studies have found that dietary exposure to AA is associated with certain cancers such as renal cell carcinoma, ovarian cancer, and endometrial cancer.7-9 Exposure assessments of AA require the analysis of metabolites of both AA and GA which are mainly measured in serum (Hb adduct) or urine (AAMA and GAMA). The advantages of analytes such as HbAA and HbGA include longer half‑life and better cost‑effectiveness. The best estimates of daily exposure of AA would be based on a 24‑hour urine specimen, and adjusted for patient’s age, gender, body mass index, dietary habits, renal function, and other factors. However, the collection of 24‑hour samples is difficult and impractical for extensive biomonitoring studies such as NHANES (National Health and Nutrition Examination Survey) by the Centers for Disease Control and Prevention (CDC).10
Cigarette smoke is a significant source of AA. A previous study disclosed that total exposure to AA in the population of smokers is more than 50% greater than that of nonsmokers.11 Since smoking causes many diseases and is a significant public health threat worldwide, promoting smoking cessation is a most crucial intervention that can help to maintain the health of smokers and nonsmokers. In addition, it can lead to great financial savings. Currently, methods for smoking cessation include pharmacological and nonpharmacological interventions. Therapies that aid smoking cessation include nicotine replacement therapy, bupropion, and varenicline.12 In the past decade, with a rapid development and widespread use of electronic cigarettes (e‑cigarettes), many smokers have tried using them in pursuit of quitting combustible cigarettes.13 However, the effect of e‑cigarettes on smoking cessation is conflicting.13-16 Additionally, e‑cigarettes also increase the risk of various diseases.17 Thus, in our study, we enrolled participants with different smoking status (nonsmokers, cigarette smokers, e‑cigarette smokers, and dual users) from the NHANES database from 2015 to 2016 who had HbAA and HbGA concentrations measured. We evaluated the exposure risk of harmful substances in patients with different smoking status.
Methods
Study design and participant selection
We analyzed the adult participants aged 18 or older in the United States from NHANES, conducted between 2015 and 2016. We screened a total of 9971 respondents. We excluded participants younger than 18 years and those who had missing data on smoking status, HbAA and HbGA concentrations, or other covariates (n = 1657). The National Center for Health Statistics Research Ethics Review Board reviewed and approved NHANES, and all participants provided written informed consent.
Smoking status
We divided survey participants into the following 4 groups: cigarette‑smoking only (C‑smokers), e‑cigarette–smoking only (E‑smokers), dual users, and nonsmokers. We defined current C‑smokers as participants who answered “yes” to the questions: “Have you smoked at least 100 cigarettes in your life” and “Do you now smoke cigarettes?”. The current E‑smoker status was based on the answer “yes” to the question: “Have you ever used an e‑cigarette?”, and the participants who fit both definitions were defined as dual users.
Measurement of hemoglobin adducts of acrylamide and glycidamide
Blood samples were obtained from NHANES participants. Measurements of HbAA and HbGA were performed by the Division of Laboratory Sciences, National Center for Environmental Health. Hemoglobin (Hb) adducts of AA and GA, HbAA and HbGA, were measured in human erythrocytes. The reaction products with the N‑terminal valine of the hemoglobin protein chains (N-[2‑carbamoyl‑ethyl] valine and N-[2‑hydroxycarbamoyl‑ethyl] valine for AA and GA, respectively) were measured. Based on the modified Edman reaction, the Edman products were analyzed by high‑performance liquid chromatography coupled with tandem mass spectrometry, and the results were processed. The analytical measurement range of the adducts is 3.9 to 6178 pmol of AA per 1 g of Hb, and 4.9 to 5618 pmol of GA per 1 g of Hb. Samples below this analytical measurement range were not reported. Samples above this range were diluted with 18 megohm‑cm deionized water and then reanalyzed. Evaluations were carried out using quality control samples at a minimum of 3 concentrations.18
Covariates
Races were categorized as “Mexican American”, “non‑Hispanic White”, “non‑Hispanic Black,” or “Hispanic”. Serum alanine aminotransferase (U/l) and glucose (mg/dl) were analyzed with the Beckman Coulter UniCel DxC 800 and DxC 660i Synchron Clinical Systems (Brea, California, United States). The test of serum creatinine (mg/dl) was analyzed on the Beckman UniCel DxC 660i Synchron Access. The alcohol use was assessed based on the answer “yes” to the question “Have you ever had at least 12 alcohol drinks / 1 year?” and body mass index was measured as weight (kg) divided by the square of height (m). Medical conditions interview data provided self- and proxy‑reported health conditions and medical history, including information on coronary heart disease and chronic bronchitis.
Statistical analysis
All data analyses were performed with SPSS (Version 18.0 for Windows, SPSS Inc, Chicago, Illinois, United States). We examined the association between concentrations of HbAA and HbGA and smoking status (C‑smokers, E‑smokers, dual users, and nonsmokers). Differences between groups were determined using analysis of variance for continuous variables, the χ2 test for categorical variables, and the Scheffe test for post‑hoc analysis. The Kolmogorov–Smirnov statistic was used to test the distribution of concentrations of HbAA and HbGA, and the logarithmic transformation was used for data normalization. Linear regression models were used to analyze the relationships of HbAA and HbGA concentrations among 4 subgroups. We fitted 4 nested regression models: model 1 was unadjusted; model 2 was adjusted for age, gender, race / Hispanic origin; and additionally, model 3 was adjusted for creatinine, alanine aminotransferase, serum glucose, and body mass index; and model 4 was further adjusted for coronary heart disease, chronic bronchitis, and alcohol drinking. P values of less than 0.05 were considered to indicate significant differences.
Results
Characteristics of the study participants
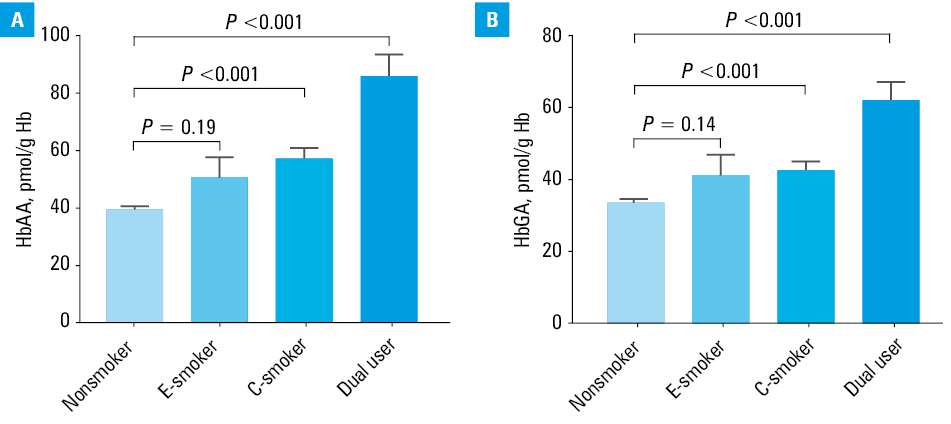
Selected baseline characteristics as well as demographic data of the study participants are provided in Table 1. The median (interquartile range [IQR]) age of nonsmokers was 46 (32–62) years (n = 884; 53.3%). A total of 4% of participants were E‑smokers (n = 67) with a median (IQR) age of 23 (19–29) years; 28.7% were C‑smokers (n = 476) with a median (IQR) age of 59 (43–69) years; 13.9% were dual users (n = 230) with a median (IQR) age of 38 (29–53) years. In C‑smokers, higher prevalence of coronary heart disease and chronic bronchitis was noted according to the questionnaire of medical conditions. The highest concentrations of HbAA (median [IQR], 83.75 [53.28–128.25] pmol/g Hb) and HbGA (median [IQR], 61.20 [40.73–89.78] pmol/g Hb) were observed in the group of dual users. Figure 1 shows the concentrations of HbAA and HbGA in the study subgroups.
Variable | Total (n = 1657) | Nonsmokers (n = 884) | E‑smokers (n = 67) | C‑smokers (n = 476) | Dual users (n = 230) | ||
Data are shown as median (interquartile range) or number (percentage). | |||||||
Age, y | 48 (33–63) | 46 (32–62) | 23 (19–29) | 59 (43–69) | 38 (29–53) | ||
Acrylamide, pmol/g Hb | 42.80 (32.60–65.60) | 37.80 (30.50–49.38) | 45.4 (33.6–68.3) | 47.00 (33.93–94.65) | 83.75 (53.28–128.25) | ||
Glycidamide, pmol/g Hb | 37.40 (27.20–53.55) | 33.20 (25.50–44.60) | 41.00 (28.00–54.80) | 39.90 (27.63–60.23) | 61.20 (40.73–89.78) | ||
Creatinine, mg/dl | 0.84 (0.69–1.00) | 0.80 (0.65–0.96) | 0.80 (0.66–0.99) | 0.89 (0.73–1.05) | 0.85 (0.73–0.99) | ||
Alanine aminotransferase, IU/l | 21 (16–28) | 20 (16–28) | 18 (14–27) | 22 (16–29) | 22 (17–30) | ||
Glucose, mg/dl | 93 (85–104) | 93 (85–103) | 88 (81–95) | 94 (86–111) | 92 (84–104) | ||
Body mass index, kg/m2 | 28.4 (24.5–32.8) | 28.4 (24.3–32.8) | 26.2 (22.0–31.1) | 28.60 (24.80–33.05) | 28.55 (24.80–33.03) | ||
Gender | Male | 821 (49.5) | 348 (42.4) | 34 (4.1) | 297 (36.2) | 142 (17.3) | |
Female | 836 (50.5) | 536 (64.1) | 33 (3.9) | 179 (21.4) | 88 (10.5) | ||
Race | Mexican American | 289 (17.4) | 167 (57.8) | 11 (3.8) | 78 (27) | 33 (11.4) | |
Other Hispanic | 232 (14.0) | 131 (56.5) | 8 (3.4) | 76 (32.8) | 17 (7.3) | ||
Non‑Hispanic White | 544 (32.8) | 243 (44.7) | 25 (4.6) | 170 (31.3) | 106 (19.5) | ||
Non‑Hispanic Black | 336 (20.3) | 166 (49.4) | 17 (5.1) | 105 (31.3) | 48 (14.3) | ||
Other | 256 (15.4) | 177 (69.1) | 6 (2.3) | 47 (18.4) | 26 (10.2) | ||
Past history | Alcohol use | 1033 (62.34) | 420 (47.62) | 50 (74.63) | 368 (77.31) | 195 (84.78) | |
Coronary heart disease | 59 (3.7) | 23 (2.7) | 0 | 26 (5.5) | 10 (4.5) | ||
Chronic bronchitis | 77 (4.8) | 26 (3.1) | 0 | 27 (5.7) | 24 (10.9) | ||
Associations between smoking and concentrations of hemoglobin adducts of acrylamide and glycidamide
The associations of smoking and concentrations of HbAA and HbGA were analyzed with linear regression and the results were described with β coefficients. The effects of e‑cigarette use on the increasing concentration of HbAA (standardized β coefficient, 0.316; P <0.001) in unadjusted model are presented in Table 2. The results of HbGA also remained significant in the unadjusted model (standardized β coefficient, 0.277; P <0.001). In a linear regression in the adjusted model, there was a positive linear association between HbAA and HbGA concentrations and e‑cigarette smoking (all P <0.001). The tests for effect modification by e‑smoking and c‑smoking including interaction terms in the models for HbAA and HbGA were demonstrated in Supplementary material, Figure S1. There was no interaction between e‑smoking and c‑smoking for AA and GA (HbAA P = 0.073). Dual users had higher HbAA and HbGA concentrations than C‑smokers.
Model | Unstandardized β (95% CI) | SE | Standardized β | P value |
a Log‑transformed concentration of hemoglobin adducts of acrylamide
b Model 1: unadjusted
c Model 2: model 1 + age in years at screening, gender, and race / Hispanic origin
d Model 3: model 2 + creatinine, alanine aminotransferase, glucose, and body mass index
e Model 4: model 3 + coronary heart disease, chronic bronchitis, and alcohol use
f Log‑transformed concentration of hemoglobin adducts of glycidamide | ||||
Acrylamidea | ||||
Model 1b | 0.521 (0.439–0.602) | 0.042 | 0.316 | <0.001 |
Model 2c | 0.461 (0.378–0.545) | 0.043 | 0.280 | <0.001 |
Model 3d | 0.461 (0.378–0.544) | 0.042 | 0.280 | <0.001 |
Model 4e | 0.430 (0.347–0.514) | 0.043 | 0.261 | <0.001 |
Glycidamidef | ||||
Model 1 | 0.418 (0.342–0.494) | 0.039 | 0.277 | <0.001 |
Model 2 | 0.356 (0.278–0.433) | 0.040 | 0.235 | <0.001 |
Model 3 | 0.361 (0.284–0.439) | 0.040 | 0.239 | <0.001 |
Model 4 | 0.344 (0.265–0.422) | 0.040 | 0.227 | <0.001 |
The associations between concentrations of HbAA and HbGA and smoking status are presented in Table 3. We applied the multivariable analysis to compare 3 smoking statuses (E‑smokers, C‑smokers, and dual users) with nonsmokers. There was a positive association in C‑smokers with HbAA and HbGA in all models as compared with nonsmokers. The standardized β coefficients of predicted HbAA between C‑smokers and nonsmokers were as follows: model 1, 0.292; model 2, 0.321; model 3, 0.321; model 4, 0.312 (all P <0.001). For HbGA, they were: model 1, 0.204; model 2, 0.261; model 3, 0.258; model 4, 0.255 (all P <0.001). Concentrations of HbAA and HbGA were also positively correlated with dual smoking status. The standardized β coefficients of predicted HbAA compared between dual users and nonsmokers in unadjusted (model 1) and adjusted models (models 2 to 4) were 0.435, 0.403, 0.403, and 0.396 (all P <0.001), respectively; and HbGA in all models were 0.366, 0.342, 0.344, and 0.342 (all P <0.001), respectively. Dual users tended to have higher HbAA and HbGA levels (P for trend <0.001). This result indicates a significant increase in HbAA and HbGA when coexposed to combustible cigarettes and e‑cigarettes compared with combustible cigarette use only.
Model | Smoking status | Acrylamidea | Glycidamideb | ||||||||
Unstandardized β (95% CI) | SE | Standardized β | P value | P value for trend | Unstandardized β (95% CI) | SE | Standardized β | P value | P value for trend | ||
a Log‑transformed concentration of hemoglobin adducts of acrylamide
b Log‑transformed concentration of hemoglobin adducts of glycidamide
c Model 1: unadjusted
d Model 2: model 1 + age in years at screening, gender, and race / Hispanic origin
e Model 3: model 2 + creatinine, alanine aminotransferase, glucose, and body mass index
f Model 4: model 3 + coronary heart disease, chronic bronchitis, and alcohol use | |||||||||||
Model 1c | Nonsmokers | Reference | – | – | – | – | Reference | – | – | – | – |
E‑smokers | 0.144 (–0.033 to 0.320) | 0.09 | 0.038 | 0.11 | <0.001 | 0.095 (–0.074 to 0.264) | 0.086 | 0.028 | 0.27 | <0.001 | |
C‑smokers | 0.398 (0.331–0.465) | 0.034 | 0.292 | <0.001 | 0.256 (0.192–0.320) | 0.033 | 0.204 | <0.001 | |||
Dual users | 0.770 (0.684–0.857) | 0.044 | 0.435 | <0.001 | 0.595 (0.512–0.678) | 0.042 | 0.366 | <0.001 | |||
Model 2d | Nonsmokers | Reference | – | – | – | – | Reference | – | – | – | – |
E‑smokers | 0.010 (–0.167 to 0.186) | 0.09 | 0.003 | 0.92 | <0.001 | –0.051 (–0.218 to 0.117) | 0.085 | –0.015 | 0.55 | <0.001 | |
C‑smokers | 0.439 (0.370–0.507) | 0.035 | 0.321 | <0.001 | 0.327 (0.262–0.392) | 0.033 | 0.261 | <0.001 | |||
Dual users | 0.713 (0.626–0.799) | 0.044 | 0.403 | <0.001 | 0.556 (0.474–0.638) | 0.042 | 0.342 | <0.001 | |||
Model 3e | Nonsmokers | Reference | – | – | – | – | Reference | – | – | – | – |
E‑smokers | –0.006 (–0.180 to 0.168) | 0.089 | –0.002 | 0.95 | <0.001 | –0.048 (–0.215 to 0.120) | 0.085 | –0.014 | 0.58 | <0.001 | |
C‑smokers | 0.438 (0.370–0.505) | 0.034 | 0.321 | <0.001 | 0.323 (0.259–0.388) | 0.033 | 0.258 | <0.001 | |||
Dual users | 0.714 (0.629–0.799) | 0.043 | 0.403 | <0.001 | 0.559 (0.478–0.641) | 0.042 | 0.344 | <0.001 | |||
Model 4f | Nonsmokers | Reference | – | – | – | – | Reference | – | – | – | – |
E‑smokers | –0.017 (–0.192 to 0.159) | 0.089 | –0.004 | 0.85 | <0.001 | –0.047 (–0.215 to 0.121) | 0.086 | –0.014 | 0.58 | <0.001 | |
C‑smokers | 0.426 (0.356–0.496) | 0.036 | 0.312 | <0.001 | 0.320 (0.253–0.387) | 0.034 | 0.255 | <0.001 | |||
Dual users | 0.701 (0.613–0.789) | 0.045 | 0.396 | <0.001 | 0.557 (0.473–0.641) | 0.043 | 0.342 | <0.001 | |||
Discussion
Our research explores the risk of exposure to AA and its derivative GA in patients with varying smoking status. This study was the first to analyze the association between smoking patterns and HbAA and HbGA levels, which are biological markers used to measure the exposure to harmful substances produced during tobacco smoking. According to our results, there is a significant association between C‑smokers and concentrations of HbAA and HbGA. Furthermore, a significant increase in the concentrations of HbAA and HbGA in the dual‑user subgroup was noted. The results suggest disadvantage of using e‑cigarettes, especially among dual users. At present, AA has been found to exist in the smoke of combustible cigarettes and e‑cigarettes.11 Although the long‑term effect of AA from e‑cigarettes remains unclear, exposure to various chemicals and ultrafine particles is more likely to cause permanent damage to the body.
E‑cigarettes were first introduced into the United States market in 2007 and have been rapidly developed since then. In the past decade, e‑cigarettes have gained widespread use among the youth and young adults.16 According to the 2020 National Youth Tobacco Survey, 19.6% of high school students (3.02 million) and 4.7% of middle school students (550 000) reported current e‑cigarette use.19,20 In 2018, 3.2% of American adults were current e‑cigarette users.21 Regulations on e‑cigarettes vary across countries and states, ranging from no rule to a complete ban. Substances identified in e‑liquids and aerosols from informal sources include nicotine, solvent carriers (propylene glycol and glycerol), tobacco‑specific nitrosamines, tetrahydrocannabinol (THC), vitamin E acetate, aldehydes, metals, volatile organic compounds, phenolic compounds, polycyclic aromatic hydrocarbons, flavorings, tobacco alkaloids, and even illicit drugs. Nevertheless, under accurate conditions of use, there is substantial evidence that except for nicotine, exposure to potentially toxic substances from e‑cigarettes is significantly lower compared with combustible tobacco cigarettes.22
The development of e‑cigarettes has roused public health concerns as their health effects are unknown.17,22 The potential acute toxic effects of e‑cigarettes include accidental or intentional ingestion of liquids and physical injuries such as burns or explosion of the devices, which lead to the injury of hands, face, eyes, and mouth.23,24 The relevant lung disease is named EVALI (electronic cigarette or vaping product use–associated lung injury) in the CDC guideline. The incidence of this novel disease gradually increases, which also causes severe outcomes and leads to mortality.25,26 The critical risk factor for EVALI is using an e‑cigarette or a similar product containing THC and vitamin E acetate. The CDC recommends that smokers consider restraining from using e‑cigarette products containing THC. The majority of patients with EVALI report use of products containing THC (75% to 80%).25 The mechanism of vitamin E acetate toxicity is unknown but may be related to pyrolysis by‑products.27 The CDC and the Food and Drug Administration recommend that people not use e‑cigarettes or vaping products containing THC, especially from informal sources like friends, family, or in‑person or online dealers. If C‑smokers choose to use e‑cigarettes as a substitute for cigarettes or quit smoking, they should consult their healthcare professionals and understand the hazards of EVALI.
We divided the general population’s smoking patterns to C‑smokers, E‑smokers, dual users, and nonsmokers. In our study, 77.8% of participants using e‑cigarettes were dual users. In 2015, among the current total number of adult e‑cigarette users, dual users were 58.8%, and former smokers were 29.8%.28 With the high prevalence of dual‑use among e‑cigarettes users, the reasons for using e‑cigarettes are of serious concern.28,29 The primary motivation for using e‑cigarettes for former and current smokers was smoking cessation (42% and 39%, respectively), and this was followed by the belief that e‑cigarettes were healthier than tobacco cigarettes (38% and 33%, respectively).30 Since the initiation of e‑cigarette smoking, only 21% of never‑smokers reported that they planned to quit e‑cigarettes compared with 40% of former smokers and 45% of current smokers.22 Although dual use may have a positive public health impact if it leads to successful smoking cessation, there is no comprehensive information about the impact of e‑cigarette smoking.31,32 The use of e‑cigarettes has been on the rise in the past decade, and the level of government regulations has increased due to the outbreak of EVALI. Relevant prevention and control actions are urgently needed to safeguard public health.20,26,33
The health effects of tobacco use are well documented. Immediate adverse health outcomes of cigarette smoking include physiologic disadvantage, lower self‑reported health, susceptibility to acute illnesses and respiratory symptoms, and absence from school and work. Among the long‑term health effects, diseases caused by smoking include coronary heart disease, cancer, and chronic obstructive pulmonary disease, which are the major causes of death in middle- and upper‑income nations.34,35 Recent studies have shown that dual users are associated with a higher risk of cardiovascular disease than cigarette‑only smokers.36,37 Dual users were significantly more likely to report adverse effects of vaping than E‑smokers (26.2% vs 11.8%; P <0.001). More dual users experienced cough, mouth or tongue sores / inflammation, dizziness, and heart palpitation than E‑smokers.38 Dual users reported the lowest physical activity levels, followed by C‑smokers and then E‑smokers. Moreover, dual users reported having depression more often and had higher anxiety scores compared with C‑smokers.39 Statistics from various countries revealed that E‑smokers are relatively young and have a relatively short smoking history. There are no data on long‑term health outcomes of dual users compared with C‑smokers and E‑smokers. Hence, evaluations of the exposure to substances that may cause adverse health effects and that may be a risk for major diseases need to be studied.
Whether dual users smoke fewer cigarettes per day than C‑smokers varies from study to study. The findings from several recent studies have conflicted on the effectiveness of e‑cigarettes for smoking cessation under real‑world situations.40 The updated Cochrane Database of Systematic Reviews of Electronic cigarettes for smoking cessation in 2021 suggested that e‑cigarettes with nicotine increase quit rates compared with those without nicotine and nicotine replacement therapy (moderate‑certainty evidence). They may work better than no support or behavioral support alone.41 In contrast, e‑cigarette use as a consumer product is not significantly associated with cigarette smoking cessation in the general adult population. Among people who smoke, daily e‑cigarette consumer product use was associated with significantly increased smoking cessation. In contrast, less‑than‑daily e‑cigarette use was associated with substantially less smoking cessation. The provision of free e‑cigarettes was associated with significantly increased smoking cessation in randomized clinical trials of e‑cigarettes as smoking cessation therapy.42 E‑cigarettes with different devices with various capacities or battery power could increase the attractiveness and dependence of e‑cigarettes using. Unlike combustible cigarette smoking, it is more difficult to quantify the intensity of e‑cigarette additions as there is no accurate tool to measure the amount of e‑cigarette use and the intake of nicotine or other substances by these smokers. The frequency of vaping, the intensity of e‑cigarette additions, and the characteristics of e‑cigarettes vary greatly.43 E‑cigarettes may warrant consideration as a prescription drug to be used as part of a clinically supervised smoking cessation intervention, provided that the associated risks commensurate with the benefit.
Most e‑cigarettes are promoted as having reduced harm of second‑hand smoke and as compliant with smoke‑free environment policies. Such misinformation is mainly aimed at young people who may find e‑cigarette use more acceptable, and this may increase the smoking rates among young people. A recent study reported that only a quarter of adolescents who vape tried to quit in the past year.44 The gateway effect of e‑cigarettes is still controversial. Among adolescents who have never smoked, the use of e‑cigarettes may increase the risk of starting to use cigarettes and other combustible products when the purchase of cigarettes becomes legal during the transition to adulthood.45 A meta‑analysis of 17 studies from the United States, United Kingdom, Mexico, Germany, and the Netherlands provided evidence that e‑cigarette use was associated with significantly increased odds of subsequent cigarette smoking initiation (odds ratio, 4.59; 95% CI, 3.60–5.85). However, there was high heterogeneity (I2 = 88%).46
This study has some limitations. First, this was an observational, retrospective analysis of an existing database from a single period, rather than an analysis of long‑term repeated observations with limited causal inferences. A study of the hazards of e‑cigarettes and the exposure of AA needs longitudinal surveys to address this issue. Second, recall error and bias in self‑reported medical histories and smoking status were recognized. Third, we did not have data about lifetime e‑cigarette use, no specific use pattern, and no standard measurements to define current e‑cigarette use. Likewise, participants’ smoking intensities, frequencies, and motivations during the examination were affected by the biopsychosocial background. Fourth, the information about diet impact on AA exposure was limited. Additionally, e‑cigarette users are mostly adolescents, but the study only enrolled participants over 18 years. The adverse effects of smoking in the youth population need further evaluation.
Conclusion
Our work aimed to determine the exposure risk of AA for the ethnic groups with different smoking habits. This study demonstrated the multivariable regression models compared to other smoking groups and HbAA and HbGA concentrations. No significant difference between E‑smokers and nonsmokers in fully adjusted model was noted. We Figured the positive association between C‑smokers and HbAA and HbGA, which is consistent with previous research. Notably, we discovered the substantial relationship of dual users with HbAA and HbGA. The study had no conclusion on the effect of e‑cigarettes on smoking cessation, but it can point out the risks of health hazards. This highlights the harmful results of coexposure of e‑cigarettes and combustible cigarettes and the risks of AA exposure, which may increase the risks of neurotoxicity, carcinogenicity, reproductive toxicity, and genotoxicity. Dual users may be motivated to initiate using e‑cigarettes as they may consider them as smoking cessation tools or due to a lack of awareness of the dangers of e‑cigarettes and their addictive substances. The use of e‑cigarettes requires correct user education and government regulation. Longitudinal studies that explore the hazards of e‑cigarettes are warranted. Furthermore, knowledge about the adverse health effects of e‑cigarette and dual use needs to be furthered by more research and promoted to the public.
- Fennell TR, Sumner SCJ, Snyder RW, et al. Metabolism and hemoglobin adduct formation of acrylamide in humans. Toxicol Sci. 2005; 85: 447‑459. | Crossref
- Ghanayem BI, McDaniel LP, Churchwell MI, et al. Role of CYP2E1 in the epoxidation of acrylamide to glycidamide and formation of DNA and hemoglobin adducts. Toxicol Sci. 2005; 88: 311‑318. | Crossref
- Sumner SC, Fennell TR, Moore TA, et al. Role of cytochrome P450 2E1 in the metabolism of acrylamide and acrylonitrile in mice. Chem Res Toxicol. 1999; 12: 1110‑1116. | Crossref
- Sumner SCJ, Selvaraj L, Nauhaus SK, et al. Urinary metabolites from F344 rats and B6C3F1 mice coadministered acrylamide and acrylonitrile for 1 or 5 Days. Chem Res Toxicol. 1997; 10: 1152‑1160. | Crossref
- Tyl RW, Friedman MA. Effects of acrylamide on rodent reproductive performance. Reprod Toxicol. 2003; 17: 1‑13. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION